Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Video Recap of Alleles and Genes by Amoeba SistersDocument3 pagesVideo Recap of Alleles and Genes by Amoeba Sistersur100% (2)
- Schizophrenia Case StudyDocument14 pagesSchizophrenia Case Studykristinanicole47100% (3)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Emergency and Disaster NursingDocument13 pagesEmergency and Disaster Nursingkarenkaren09Pas encore d'évaluation
- Unit 2 Poisons and PoisoningDocument16 pagesUnit 2 Poisons and PoisoningKhar Mel GoPas encore d'évaluation
- MCPS Sports Concussion Data 2014-15Document1 pageMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdPas encore d'évaluation
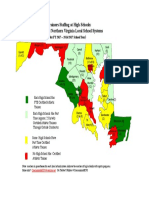
- Projected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCDocument1 pageProjected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCConcussion_MCPS_MdPas encore d'évaluation
- MCPS Sports Concussion Data 2013-14Document1 pageMCPS Sports Concussion Data 2013-14Concussion_MCPS_MdPas encore d'évaluation
- 2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfDocument5 pages2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfConcussion_MCPS_MdPas encore d'évaluation
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Document11 pagesParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdPas encore d'évaluation
- MCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Document1 pageMCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- LCPS Response To Parents Re Inova-Brain Sentry Research ProposalDocument2 pagesLCPS Response To Parents Re Inova-Brain Sentry Research ProposalConcussion_MCPS_MdPas encore d'évaluation
- NFL 2010 Letter Re Concussion LegDocument2 pagesNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdPas encore d'évaluation
- MCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Document2 pagesMCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Document73 pagesMCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Concussion_MCPS_MdPas encore d'évaluation
- MCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Document2 pagesMCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalDocument5 pagesBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdPas encore d'évaluation
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Document9 pagesMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Document6 pagesMCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Tobacco-Free SCH PolicyDocument2 pagesMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdPas encore d'évaluation
- Minutes of MD ST BD of Ed Meeting, 4-22-2014Document47 pagesMinutes of MD ST BD of Ed Meeting, 4-22-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentDocument1 pageTemplate 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentConcussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Penalties For Tobacco Use at SchoolDocument2 pagesMCPS (MD) Penalties For Tobacco Use at SchoolConcussion_MCPS_MdPas encore d'évaluation
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Document1 pageTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdPas encore d'évaluation
- MPSSAA HeadsUp Media Release, 5-5-2014Document1 pageMPSSAA HeadsUp Media Release, 5-5-2014Concussion_MCPS_MdPas encore d'évaluation
- PPE Ath W/ Special Needs-Suppl History FormDocument1 pagePPE Ath W/ Special Needs-Suppl History FormConcussion_MCPS_MdPas encore d'évaluation
- Template 1-B, MCPS Athletics Injury Reports 2013-2014Document2 pagesTemplate 1-B, MCPS Athletics Injury Reports 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Document9 pagesMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Document1 pageTemplate 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Concussion_MCPS_MdPas encore d'évaluation
- Template 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Document1 pageTemplate 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdPas encore d'évaluation
- Template 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Document2 pagesTemplate 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Document1 pageTemplate 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS Reg For Reporting Student InjuriesDocument2 pagesMCPS Reg For Reporting Student InjuriesConcussion_MCPS_MdPas encore d'évaluation
- HoCo MD BOE Agenda 01-23-14Document2 pagesHoCo MD BOE Agenda 01-23-14Concussion_MCPS_MdPas encore d'évaluation
- MCPS Student Injury Report FormDocument2 pagesMCPS Student Injury Report FormConcussion_MCPS_MdPas encore d'évaluation
- First Aid Plan ConstructionDocument13 pagesFirst Aid Plan ConstructionUmair KhanPas encore d'évaluation
- Block Placement Report: Submitted To (Block Placement Coordinator) : MR Bhat IqbalDocument32 pagesBlock Placement Report: Submitted To (Block Placement Coordinator) : MR Bhat IqbalSherry SherPas encore d'évaluation
- Sick Role: BY DR P.N. KarimiDocument10 pagesSick Role: BY DR P.N. KarimiGerald Limo Arap ChebiiPas encore d'évaluation
- Chapter 22: Young Adult Edelman: Health Promotion Throughout The Life Span, 8th EditionDocument10 pagesChapter 22: Young Adult Edelman: Health Promotion Throughout The Life Span, 8th Editionmarvado10100% (1)
- Bipolar Disorder Resource CompendiumDocument98 pagesBipolar Disorder Resource Compendiummonts1234Pas encore d'évaluation
- Chapter 1-5 PDFDocument77 pagesChapter 1-5 PDFEstebanPas encore d'évaluation
- GENEVA Apple Rootstocks Comparison Chart PDFDocument3 pagesGENEVA Apple Rootstocks Comparison Chart PDFEugeniu GudumacPas encore d'évaluation
- MAPEH - Part 4: Key Health ConceptsDocument13 pagesMAPEH - Part 4: Key Health ConceptsLergen B. AguilarPas encore d'évaluation
- Accepted Manuscript: Complementary Therapies in MedicineDocument24 pagesAccepted Manuscript: Complementary Therapies in MedicineAndrea BarresiPas encore d'évaluation
- City of Galveston RFP Employee Health Insurance Addendum #3Document75 pagesCity of Galveston RFP Employee Health Insurance Addendum #3garbagepatchPas encore d'évaluation
- Food Adulteration: A Review: March 2017Document5 pagesFood Adulteration: A Review: March 2017Payal GandhiPas encore d'évaluation
- Prayer Points - Feb 2013Document4 pagesPrayer Points - Feb 2013doorkeepersPas encore d'évaluation
- 4 Agroecology IPMDocument16 pages4 Agroecology IPMZahara AmalinaPas encore d'évaluation
- CBCDocument12 pagesCBCDaNa Al-jomah100% (1)
- Incisions For Open Abdominal Surgery - UpToDate2020 PDFDocument36 pagesIncisions For Open Abdominal Surgery - UpToDate2020 PDFGerii Pucllas VillarPas encore d'évaluation
- The Mpact: Smok NGDocument1 pageThe Mpact: Smok NGsabaPas encore d'évaluation
- Coffee Production in The PhilippinesDocument23 pagesCoffee Production in The PhilippinesRamilArtatesPas encore d'évaluation
- Chapter-4: Ocean DevelopmentDocument6 pagesChapter-4: Ocean DevelopmentDHARMAVARAPU NAGESWARIPas encore d'évaluation
- Ayurveda Medicine of the GodsDocument20 pagesAyurveda Medicine of the Godsramdas2430Pas encore d'évaluation
- Medical Physics - RespiratoryDocument9 pagesMedical Physics - RespiratoryAhmad wastiPas encore d'évaluation
- Knowledge About Diabetic ComplicationsDocument5 pagesKnowledge About Diabetic ComplicationsAdmasu BelayPas encore d'évaluation
- Phytochemical Analysis and Uses of Mimosa pudica LinnDocument4 pagesPhytochemical Analysis and Uses of Mimosa pudica LinnaisahPas encore d'évaluation
- Assignment 2 Biol 1700 Fall 2020Document20 pagesAssignment 2 Biol 1700 Fall 2020api-535587985Pas encore d'évaluation
- Genomics in India - Kapil Khandelwal - EquNev CapitalDocument5 pagesGenomics in India - Kapil Khandelwal - EquNev CapitalKapil KhandelwalPas encore d'évaluation
- Judi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Document66 pagesJudi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Judi Januadi Endjun, MD, ObsGynPas encore d'évaluation
- No Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanDocument16 pagesNo Nama Barang Stok Awal Barang Masuk Barang Keluar Sisa Stock Harga SatuanNurmalasari SaryPas encore d'évaluation