Vous aimerez peut-être aussi
- Belair-Manor Final July 2019 CalendarDocument1 pageBelair-Manor Final July 2019 CalendarasbriglioPas encore d'évaluation
- Bel-Air Manor June 2019 CalendarDocument1 pageBel-Air Manor June 2019 CalendarasbriglioPas encore d'évaluation
- BA Open Position Report 5-21-19Document1 pageBA Open Position Report 5-21-19asbriglioPas encore d'évaluation
- BA Open Position Report 4-17-19Document1 pageBA Open Position Report 4-17-19asbriglioPas encore d'évaluation
- Bel-Air Manor April 2019 CalendarDocument1 pageBel-Air Manor April 2019 CalendarasbriglioPas encore d'évaluation
- BA Open Position Report 3-26-18Document1 pageBA Open Position Report 3-26-18asbriglioPas encore d'évaluation
- Bel-Air Manor March 2019 CalendarDocument1 pageBel-Air Manor March 2019 CalendarasbriglioPas encore d'évaluation
- CH Open Position Report 1-11-18Document1 pageCH Open Position Report 1-11-18asbriglioPas encore d'évaluation
- Bel-Air Manor February 2019 CalendarDocument1 pageBel-Air Manor February 2019 CalendarasbriglioPas encore d'évaluation
- BA Open Position Report 2-19-19Document1 pageBA Open Position Report 2-19-19asbriglioPas encore d'évaluation
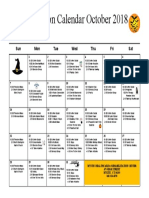
- Bel-Air Manor Oct 2018 Rec CalendarDocument1 pageBel-Air Manor Oct 2018 Rec CalendarasbriglioPas encore d'évaluation
- MH Open Positions 3-01-19Document1 pageMH Open Positions 3-01-19asbriglioPas encore d'évaluation
- CH 2019 Feb ActivitiesDocument1 pageCH 2019 Feb ActivitiesasbriglioPas encore d'évaluation
- AM Jan Calendar 2019Document1 pageAM Jan Calendar 2019asbriglioPas encore d'évaluation
- BA Open Position Report 1-11-19Document1 pageBA Open Position Report 1-11-19asbriglioPas encore d'évaluation
- Mystic Recreation Calendar October 2018Document1 pageMystic Recreation Calendar October 2018asbriglioPas encore d'évaluation
- BA Open Position Report 10-08-18Document1 pageBA Open Position Report 10-08-18asbriglioPas encore d'évaluation
- BA Open Position Report 12-07-18Document1 pageBA Open Position Report 12-07-18asbriglioPas encore d'évaluation
- MM Open Position Report 10-10-18Document2 pagesMM Open Position Report 10-10-18asbriglioPas encore d'évaluation
- LC October 2018 2ndDocument1 pageLC October 2018 2ndasbriglioPas encore d'évaluation
- LC October 2018 ManorDocument1 pageLC October 2018 ManorasbriglioPas encore d'évaluation
- LC October 2018 4thDocument1 pageLC October 2018 4thasbriglioPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- MyLabX5 160000160 V04 LRDocument5 pagesMyLabX5 160000160 V04 LRVishnu0049Pas encore d'évaluation
- Adolescent GangsDocument289 pagesAdolescent GangsReuben EscarlanPas encore d'évaluation
- NBME 16 Complete PDFDocument112 pagesNBME 16 Complete PDFSilar Khan67% (18)
- Manual Steamvection ThermasolDocument6 pagesManual Steamvection ThermasolJosse RuizPas encore d'évaluation
- Specialty Pharmaceutical Biotechnology Sales in Sarasota FL Resume Jeffrey MinettDocument1 pageSpecialty Pharmaceutical Biotechnology Sales in Sarasota FL Resume Jeffrey MinettJeffreyMinettPas encore d'évaluation
- SRP Batch 1Document32 pagesSRP Batch 1eenahPas encore d'évaluation
- Magellan Code ChangesDocument15 pagesMagellan Code ChangesdaringdreuPas encore d'évaluation
- BCG - The Future of Jobs in The Era of AI - 2021 - NeiDocument40 pagesBCG - The Future of Jobs in The Era of AI - 2021 - NeiHevertom FischerPas encore d'évaluation
- Soal Bahasa InggrisDocument2 pagesSoal Bahasa Inggrisana fauziahPas encore d'évaluation
- Endocrine SystemDocument41 pagesEndocrine SystemAtteya Mogote AbdullahPas encore d'évaluation
- Meghan Baxendell Resume January 2017 OnlineDocument3 pagesMeghan Baxendell Resume January 2017 Onlineapi-323081470Pas encore d'évaluation
- Daftar PustakaDocument1 pageDaftar PustakaDaffa ArkanantaPas encore d'évaluation
- LESSON 1 - The Global North and SouthDocument9 pagesLESSON 1 - The Global North and SouthJeff Jeremiah PereaPas encore d'évaluation
- Stem Cells and The Regenerative Therapy Following Lameness Resulting From Equine Tendon InjuryDocument15 pagesStem Cells and The Regenerative Therapy Following Lameness Resulting From Equine Tendon InjuryCharlotte ButlerPas encore d'évaluation
- Your Wellness Profile: Laboratory ActivitiesDocument4 pagesYour Wellness Profile: Laboratory Activitiesdusty kawiPas encore d'évaluation
- VtM2nded1 Page PDFDocument1 pageVtM2nded1 Page PDFJoseph CortesPas encore d'évaluation
- Emergency Response Procedures Manual - PT. Saberindo Pacific - 2011Document15 pagesEmergency Response Procedures Manual - PT. Saberindo Pacific - 2011Indah Rida Afriyanti100% (1)
- 19-CPS Student Induction Presentation-RAZAK FinalDocument18 pages19-CPS Student Induction Presentation-RAZAK FinalbaderPas encore d'évaluation
- Toxicology Procedures ManualDocument206 pagesToxicology Procedures ManualDrMd IdrisPas encore d'évaluation
- Tetanus Treatment: Vitria DwiayuDocument12 pagesTetanus Treatment: Vitria DwiayuvitriaPas encore d'évaluation
- A. Differential Diagnosis:: Bone MetastasisDocument3 pagesA. Differential Diagnosis:: Bone MetastasisDonna DumaliangPas encore d'évaluation
- Business Studies 05Document22 pagesBusiness Studies 05Nepomuk Balthasar HaindlPas encore d'évaluation
- Post-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceDocument17 pagesPost-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceMari PaoPas encore d'évaluation
- Portfolio In: Morong National High SchoolDocument5 pagesPortfolio In: Morong National High SchoolSophrina Jazmynrose CruzPas encore d'évaluation
- Antinociceptic Activity of Talisay ExtractDocument22 pagesAntinociceptic Activity of Talisay ExtractRein Paul Pascua TomasPas encore d'évaluation
- Chest Drains Al-WPS OfficeDocument16 pagesChest Drains Al-WPS OfficeisnainiviaPas encore d'évaluation
- Daftar Pustaka: PenyakitDocument9 pagesDaftar Pustaka: Penyakitmagdalena kristantiPas encore d'évaluation
- The X Factor 11Document31 pagesThe X Factor 11writerguy78Pas encore d'évaluation
- 2016 Article InternationalEcoHealthOneHealtDocument139 pages2016 Article InternationalEcoHealthOneHealtMauricio FemeníaPas encore d'évaluation
- Is Our Brain Really Necessary-LorberDocument3 pagesIs Our Brain Really Necessary-Lorberbigjon1359100% (1)