Vous aimerez peut-être aussi
- Pharmacology of HypertensionDocument4 pagesPharmacology of HypertensionFlower100% (1)
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Drug ChartDocument20 pagesDrug Chartstarobin100% (1)
- Diabetes Topic DiscussionDocument9 pagesDiabetes Topic DiscussionSamPas encore d'évaluation
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresPas encore d'évaluation
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Document48 pagesNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanPas encore d'évaluation
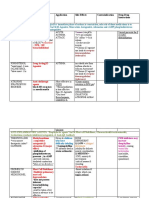
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinPas encore d'évaluation
- Know Common Disease ManagementDocument14 pagesKnow Common Disease Managementcdx25Pas encore d'évaluation
- Squamous Cell Carcinoma-Well DifferentiatedDocument4 pagesSquamous Cell Carcinoma-Well DifferentiatedYukankolmi OyoPas encore d'évaluation
- Pharmacology Final Study GuideDocument9 pagesPharmacology Final Study GuideMichaelaPas encore d'évaluation
- Top Drugs: 1. ACETAMINOPHEN (Tylenol)Document12 pagesTop Drugs: 1. ACETAMINOPHEN (Tylenol)epingPas encore d'évaluation
- C. Anti-Hypertensive Drugs.Document10 pagesC. Anti-Hypertensive Drugs.Nabeel AsifPas encore d'évaluation
- Class IV Antidysryth Mic DrugsDocument29 pagesClass IV Antidysryth Mic DrugsFluffy_icePas encore d'évaluation
- R: K D, M, S T: Xprep EY Rugs Nemonics Tudy IPSDocument18 pagesR: K D, M, S T: Xprep EY Rugs Nemonics Tudy IPSKPas encore d'évaluation
- Heart Failure Topic DiscussionDocument11 pagesHeart Failure Topic Discussionapi-665372449Pas encore d'évaluation
- Module 4 - Basic Pharmacology UpdateDocument42 pagesModule 4 - Basic Pharmacology UpdateWin Htet0% (1)
- Pharmacy Operations: Licensure, Registration and CertifiacationsDocument5 pagesPharmacy Operations: Licensure, Registration and CertifiacationsHitomi Shiroshita100% (1)
- Infection Control QuestionsDocument2 pagesInfection Control QuestionsNhor BasmalaPas encore d'évaluation
- Laryngeal Trauma: Dr. Ida Sjailandrawati Harahap, SP.T.H.T.K.LDocument19 pagesLaryngeal Trauma: Dr. Ida Sjailandrawati Harahap, SP.T.H.T.K.LNoni100% (1)
- Pharma ChartsDocument33 pagesPharma ChartsNooreen Hussain100% (1)
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Pharmacology CNS DrugsDocument15 pagesPharmacology CNS DrugsM Youssif Elkady100% (1)
- To The Point PharmacologyDocument5 pagesTo The Point PharmacologyDR AbidPas encore d'évaluation
- Pharmacology Mnemonics (Part 01) by M IhtishamDocument32 pagesPharmacology Mnemonics (Part 01) by M Ihtishammuhammad ihtisham ul hassan100% (1)
- 2016 EMS Protocols IOWADocument104 pages2016 EMS Protocols IOWATasi'ah Nashirah NurPas encore d'évaluation
- Common Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesDocument2 pagesCommon Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesjthsPas encore d'évaluation
- All Other ClassificationsDocument6 pagesAll Other ClassificationsCorey100% (1)
- Drugs Interaction1Document13 pagesDrugs Interaction1Akshay MandhotraPas encore d'évaluation
- DyslipidemiaDocument44 pagesDyslipidemiaenri100% (1)
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumPas encore d'évaluation
- Management of HyperlipidemiaDocument39 pagesManagement of HyperlipidemiaRajgopal100% (2)
- Advantage of FDC Atozet-Sv - EditDocument31 pagesAdvantage of FDC Atozet-Sv - EditSuardy Ciayadi100% (1)
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraPas encore d'évaluation
- Potts DiseaseDocument3 pagesPotts DiseasePaul Stephen PinedaPas encore d'évaluation
- FormularyDocument49 pagesFormularyvijay kumarPas encore d'évaluation
- Atozet Slide Deck New-PresentationDocument49 pagesAtozet Slide Deck New-PresentationMustafa JaradatPas encore d'évaluation
- Common DrugsDocument15 pagesCommon DrugsKate Penelope DalidPas encore d'évaluation
- Prescribing Medicine in Pregnancy, by Australian Drug Evaluation CommitteeDocument90 pagesPrescribing Medicine in Pregnancy, by Australian Drug Evaluation Committee徐承恩100% (1)
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaPas encore d'évaluation
- PharmacokineticsDocument7 pagesPharmacokineticsJan KarnowskiPas encore d'évaluation
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Name: Ma. Princess P. Seril DATE: DECEMBER 5, 6, 8, 9-2011 GROUP: 53 Area: Alimannao Rhu Clinical Instructor: Evelyn C. Cristobal, RNDocument2 pagesName: Ma. Princess P. Seril DATE: DECEMBER 5, 6, 8, 9-2011 GROUP: 53 Area: Alimannao Rhu Clinical Instructor: Evelyn C. Cristobal, RNRoshin TejeroPas encore d'évaluation
- Nursing Care Plan For Risk For Compromised Human Dignity NCPDocument3 pagesNursing Care Plan For Risk For Compromised Human Dignity NCPderic100% (2)
- Malabsorption A Clinical ApproachDocument42 pagesMalabsorption A Clinical ApproachMunish DograPas encore d'évaluation
- ISTDP Coughlin KatzmanDocument4 pagesISTDP Coughlin Katzmanmilane84Pas encore d'évaluation
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsDocument57 pagesDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaPas encore d'évaluation
- Vancomycin ReviewDocument26 pagesVancomycin Reviewkhangsiean89Pas encore d'évaluation
- Letter of RecomendationDocument2 pagesLetter of RecomendationJorge Luis Sánchez Alarcón100% (1)
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasPas encore d'évaluation
- Sem 5/unit-3 Autocoids & Related DrugsDocument28 pagesSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudPas encore d'évaluation
- Pharmacology MnemonicsDocument26 pagesPharmacology MnemonicsArthur JamesPas encore d'évaluation
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanPas encore d'évaluation
- Mnemonic PharmaDocument13 pagesMnemonic Pharmamanoj kumarPas encore d'évaluation
- Agents Causing Coma or SeizuresDocument3 pagesAgents Causing Coma or SeizuresShaira Aquino VerzosaPas encore d'évaluation
- ALD WITH ASCITES by VaibhavDocument22 pagesALD WITH ASCITES by VaibhavSandeep ChakravarthyPas encore d'évaluation
- Osmotic DiureticsDocument30 pagesOsmotic Diureticsrhimineecat71100% (1)
- Beta BlockersDocument1 pageBeta BlockersShrikant ThakurPas encore d'évaluation
- Introduction To Pharmacoepidemiology 2015 PDFDocument20 pagesIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapPas encore d'évaluation
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 pagesNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraPas encore d'évaluation
- Drugs Acting On The AnsDocument57 pagesDrugs Acting On The AnsAnonymous iG0DCOfPas encore d'évaluation
- DyslipidemiaDocument55 pagesDyslipidemiaearldioborrinagaPas encore d'évaluation
- Nutrition of The Cardiovasculer SystemDocument37 pagesNutrition of The Cardiovasculer SystemAdit KurniadiPas encore d'évaluation
- IT 9 - Nutrition of CV System - SHPDocument37 pagesIT 9 - Nutrition of CV System - SHPPraditya BriyandiPas encore d'évaluation
- Nutrition of The Cardiovasculer System: Syarif Husin Blok 10Document37 pagesNutrition of The Cardiovasculer System: Syarif Husin Blok 10Desi OktarianaPas encore d'évaluation
- Dyslipidemia 2008Document80 pagesDyslipidemia 2008Pucca' JernyPas encore d'évaluation
- Drugs For HyperlipidemiaDocument29 pagesDrugs For Hyperlipidemiasultan khabeebPas encore d'évaluation
- Hypolipidemic AgentsDocument39 pagesHypolipidemic AgentsAC ACPas encore d'évaluation
- LDL WhoDocument12 pagesLDL WhoReza HariansyahPas encore d'évaluation
- HYPERLIPIDEMIADocument33 pagesHYPERLIPIDEMIAatiqullah tarmiziPas encore d'évaluation
- Final Ortho Case YashikaDocument47 pagesFinal Ortho Case YashikaYashika GuptaPas encore d'évaluation
- Patient Positioning in Lateral Position in The Perioperative SettingDocument27 pagesPatient Positioning in Lateral Position in The Perioperative SettingjeenaalexPas encore d'évaluation
- Kelly Morrison Edited ResumeDocument2 pagesKelly Morrison Edited Resumeapi-355985174Pas encore d'évaluation
- HCFA 2007 Annual ReportDocument20 pagesHCFA 2007 Annual ReportHCFAMAPas encore d'évaluation
- Millers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Document44 pagesMillers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Adriana VickPas encore d'évaluation
- Adrenergic AgonistsDocument22 pagesAdrenergic AgonistsEthar LovePas encore d'évaluation
- The Use of Blenderized Tube Feeding in Pediatric Patients: Evidence and Guidelines For Dietetic PracticeDocument31 pagesThe Use of Blenderized Tube Feeding in Pediatric Patients: Evidence and Guidelines For Dietetic PracticeLaura Schoenfeld, MPH, RD100% (1)
- Adrenal Cortex Case StudyDocument21 pagesAdrenal Cortex Case StudyMaya Vil0% (1)
- Clinical Case Aki Presentation EportfolioDocument32 pagesClinical Case Aki Presentation Eportfolioapi-463444835Pas encore d'évaluation
- Reviewer NCM 109 LaboratoryDocument5 pagesReviewer NCM 109 Laboratorysiopili EpitychiaPas encore d'évaluation
- LPRDocument40 pagesLPRChristopher AdhisasmitaPas encore d'évaluation
- Cough: Cold:: BronchoconstrictionDocument7 pagesCough: Cold:: BronchoconstrictionAbdul MajeedPas encore d'évaluation
- Appendix and Cecum!Document13 pagesAppendix and Cecum!SilvanaPutriPas encore d'évaluation
- Daftar Obat High Alert Dan High Risk InsDocument2 pagesDaftar Obat High Alert Dan High Risk InsdindaPas encore d'évaluation
- Plan of DissertationDocument27 pagesPlan of DissertationPriya PuriPas encore d'évaluation
- Mhealth Project Proposal: Imci: Global Health Informatics To Improve Quality of CareDocument2 pagesMhealth Project Proposal: Imci: Global Health Informatics To Improve Quality of CareMito CisneroPas encore d'évaluation
- 1644 CV Europass Daniel MatosDocument2 pages1644 CV Europass Daniel MatosDaniel MatosPas encore d'évaluation
- Gus156 Slide Ginjal Dan Saluran KemihDocument128 pagesGus156 Slide Ginjal Dan Saluran KemihRina ChairunnisaPas encore d'évaluation
- Comparison of The Recovery Rate of Otomycosis Using Betadine and Clotrimazole Topical TreatmentDocument6 pagesComparison of The Recovery Rate of Otomycosis Using Betadine and Clotrimazole Topical TreatmentHendra SusantoPas encore d'évaluation
- Edkt 2030-Graded DiscussionDocument2 pagesEdkt 2030-Graded Discussionapi-271964727Pas encore d'évaluation