Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- CH 3.4-3.6 Meiosis Gizmo - StudentDocument11 pagesCH 3.4-3.6 Meiosis Gizmo - StudentKaylia SimmondsPas encore d'évaluation
- NCERT Solutions Class 12th Biology: Chapter 9 - Strategies For Enhancement in Food ProductionDocument7 pagesNCERT Solutions Class 12th Biology: Chapter 9 - Strategies For Enhancement in Food ProductionLavina D'costaPas encore d'évaluation
- Lactobacillus Probiotic Protects Intestinal EpitheliumDocument12 pagesLactobacillus Probiotic Protects Intestinal EpitheliumLavina D'costaPas encore d'évaluation
- Harv Life SC Data SCDocument5 pagesHarv Life SC Data SCLavina D'costaPas encore d'évaluation
- Chapter 7 EvolutionDocument17 pagesChapter 7 EvolutionLavina D'costaPas encore d'évaluation
- Expression of Microbiota, Toll Like Receptors,& Regulators in SmallDocument6 pagesExpression of Microbiota, Toll Like Receptors,& Regulators in SmallLavina D'costaPas encore d'évaluation
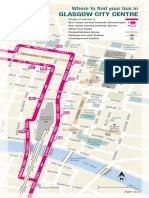
- Glasgow City Centre: Where To Find Your Bus inDocument3 pagesGlasgow City Centre: Where To Find Your Bus inLavina D'costaPas encore d'évaluation
- Cell Cycle M SmegDocument15 pagesCell Cycle M SmegLavina D'costaPas encore d'évaluation
- Chapter 3Document8 pagesChapter 3Lavina D'costaPas encore d'évaluation
- Mitochondrial DNA VariatnDocument6 pagesMitochondrial DNA VariatnLavina D'costaPas encore d'évaluation
- Regulation of Expression, Function, and inDocument9 pagesRegulation of Expression, Function, and inLavina D'costaPas encore d'évaluation
- Immuno PathologyDocument13 pagesImmuno PathologyLavina D'costaPas encore d'évaluation
- Does TLR2 Regulate Intestinal InflammationDocument3 pagesDoes TLR2 Regulate Intestinal InflammationLavina D'costaPas encore d'évaluation
- Transcriptional Profiling of BladderDocument13 pagesTranscriptional Profiling of BladderLavina D'costaPas encore d'évaluation
- B Hler Et Al 1998 Yeast 2Document9 pagesB Hler Et Al 1998 Yeast 2Lavina D'costaPas encore d'évaluation
- Trafficking of Endosomal Toll-LikeDocument10 pagesTrafficking of Endosomal Toll-LikeLavina D'costaPas encore d'évaluation
- Gut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceDocument21 pagesGut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceLavina D'costaPas encore d'évaluation
- Chapter 4: Diagnosis of TB DiseaseDocument34 pagesChapter 4: Diagnosis of TB DiseaseROHITPas encore d'évaluation
- The Toll-Like Receptor Pathway Establishes Commensal Gut ColonizationDocument14 pagesThe Toll-Like Receptor Pathway Establishes Commensal Gut ColonizationLavina D'costaPas encore d'évaluation
- Phylo PDFDocument20 pagesPhylo PDFLavina D'costaPas encore d'évaluation
- 21 24 PDFDocument4 pages21 24 PDFLavina D'costaPas encore d'évaluation
- Microbiology Lab BookDocument83 pagesMicrobiology Lab BookLavina D'costa100% (6)
- Gut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceDocument21 pagesGut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceLavina D'costaPas encore d'évaluation
- Colorazione Ziehl NeelsenDocument4 pagesColorazione Ziehl NeelsenLavina D'costaPas encore d'évaluation
- Phylo PDFDocument20 pagesPhylo PDFLavina D'costaPas encore d'évaluation
- Benefits of Caffeine Citrate - Neurodevelopmental Outcomes of ELBDocument15 pagesBenefits of Caffeine Citrate - Neurodevelopmental Outcomes of ELBLavina D'costaPas encore d'évaluation
- Phylo PDFDocument20 pagesPhylo PDFLavina D'costaPas encore d'évaluation
- GRE Screen Reader InstructionsDocument4 pagesGRE Screen Reader InstructionsWaheed UllahPas encore d'évaluation
- 2009 MMTV Like and Diagnostic Value N Human BR Ca PDFDocument31 pages2009 MMTV Like and Diagnostic Value N Human BR Ca PDFLavina D'costaPas encore d'évaluation
- Medicinal Uses For CorianderDocument2 pagesMedicinal Uses For CorianderLavina D'costaPas encore d'évaluation
- Agglutinin From Arachis Hypogaea: Site-Specific Monoclonal Antibodies Against PeanutDocument10 pagesAgglutinin From Arachis Hypogaea: Site-Specific Monoclonal Antibodies Against PeanutLavina D'costaPas encore d'évaluation
- Learning Outcome.: Terms To Know/keywordsDocument5 pagesLearning Outcome.: Terms To Know/keywordsiknowu250Pas encore d'évaluation
- 12.1, 12.2 Reading GuidesDocument4 pages12.1, 12.2 Reading GuidesShadowPas encore d'évaluation
- Biology Lab 1: Bioinformatic Report AnalysisDocument5 pagesBiology Lab 1: Bioinformatic Report AnalysisKasia DrewniakPas encore d'évaluation
- CH 6Document13 pagesCH 6c00ltimesPas encore d'évaluation
- Anti CD20 Monoclonal Antibodies Reviewing A RevolutionDocument23 pagesAnti CD20 Monoclonal Antibodies Reviewing A RevolutionJugal HarkutPas encore d'évaluation
- Andrew Friedman CVDocument2 pagesAndrew Friedman CVAndrew FriedmanPas encore d'évaluation
- Cam PathwayDocument22 pagesCam PathwayRanu MondalPas encore d'évaluation
- EURO Contraceptive Comp.Document3 pagesEURO Contraceptive Comp.Youssef KaidPas encore d'évaluation
- Tay-Sachs DiseaseDocument6 pagesTay-Sachs Diseaseapi-347043429Pas encore d'évaluation
- Scope of ImmunologyDocument6 pagesScope of ImmunologySulove Koirala100% (2)
- ANKITA.2006796 - Minor Project-1Document23 pagesANKITA.2006796 - Minor Project-1Lalru LalruPas encore d'évaluation
- Earth and Life Science: Quarter 2 - Module 25: Benefits of Genetically Modified OrganismsDocument18 pagesEarth and Life Science: Quarter 2 - Module 25: Benefits of Genetically Modified OrganismsEmer Perez60% (5)
- GENETIC MATERIALS DNA RNA CHROMOSOMESDocument48 pagesGENETIC MATERIALS DNA RNA CHROMOSOMESDam Hapratta Weheb LehaPas encore d'évaluation
- Tissue RepairDocument9 pagesTissue RepairSakidu LegionPas encore d'évaluation
- Topic 3.2 WorksheetDocument2 pagesTopic 3.2 WorksheetYixuan PENGPas encore d'évaluation
- Satyanarayan - BiotechnologyDocument880 pagesSatyanarayan - BiotechnologyDhanya L BolarPas encore d'évaluation
- Electroporation Optimization GuideDocument2 pagesElectroporation Optimization Guidethumita kumiPas encore d'évaluation
- Enzymatic Lysis and Disruption of Microbial CellsDocument5 pagesEnzymatic Lysis and Disruption of Microbial CellsSeptian JauhariansyahPas encore d'évaluation
- Infoaging Guide Theories of Agingfr PDFDocument9 pagesInfoaging Guide Theories of Agingfr PDFIndah Fatma SariPas encore d'évaluation
- Mitochondrial Genome of The Freshwater JellyfishDocument9 pagesMitochondrial Genome of The Freshwater JellyfishyangPas encore d'évaluation
- Cell Growth, Division, and Reproduction: Limits To Cell SizeDocument2 pagesCell Growth, Division, and Reproduction: Limits To Cell SizeZnite100% (1)
- Stuart Schwartz MSGF Presentation7!16!10Document87 pagesStuart Schwartz MSGF Presentation7!16!10cegfracPas encore d'évaluation
- Integrative Assessment Math Sci TLEDocument4 pagesIntegrative Assessment Math Sci TLEJastine LlarinaPas encore d'évaluation
- Yobe State College OF Agriculture, Gujba Public Health DepartmentDocument13 pagesYobe State College OF Agriculture, Gujba Public Health DepartmentYakubu Adamu JajerePas encore d'évaluation
- Transgenic CropsDocument13 pagesTransgenic Cropsrana shahid100% (1)
- Engelke1990 PDFDocument5 pagesEngelke1990 PDFDiego GarzonPas encore d'évaluation
- Phet Natural SelectionDocument6 pagesPhet Natural Selectionapi-315470323Pas encore d'évaluation
- Song 2021Document28 pagesSong 2021Supu VeeturiPas encore d'évaluation
- Virology Assignment Re WriteDocument21 pagesVirology Assignment Re WriteDires AdmasPas encore d'évaluation