Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Usmle Essential BooksDocument3 pagesUsmle Essential BooksBhavin Choksi33% (3)
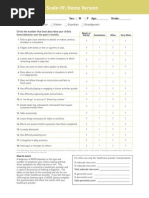
- Screening ADHDDocument2 pagesScreening ADHDPsiholog Alina Mirela CraiuPas encore d'évaluation
- Nutrient Requirements of Egg Laying Chickens: Feed ConsumptionDocument3 pagesNutrient Requirements of Egg Laying Chickens: Feed ConsumptionEzikawa Kirt100% (1)
- Acupuncture (Presentation) by Zheng JiayinDocument15 pagesAcupuncture (Presentation) by Zheng Jiayinpaperbin100% (1)
- Personalized Nutrition For Anxiety Adhd and AutismDocument32 pagesPersonalized Nutrition For Anxiety Adhd and AutismGeanyPas encore d'évaluation
- Tempt WudhuDocument1 pageTempt WudhuGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- Q EFEFDDocument1 pageQ EFEFDGilang IrwansyahPas encore d'évaluation
- SNDocument1 pageSNUddy ArdiaxaPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- PSX ReadmeDocument8 pagesPSX ReadmeohmrspikePas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- FeaaDocument1 pageFeaaGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- 2011 Article 342Document4 pages2011 Article 342Gilang IrwansyahPas encore d'évaluation
- FeaadDocument1 pageFeaadGilang IrwansyahPas encore d'évaluation
- AadDocument1 pageAadGilang IrwansyahPas encore d'évaluation
- ISSN 2073-9990 East Cent. Afr. J. Surg. (Online) : BackgroundDocument6 pagesISSN 2073-9990 East Cent. Afr. J. Surg. (Online) : BackgroundGilang IrwansyahPas encore d'évaluation
- 2010 Article 49Document5 pages2010 Article 49Gilang IrwansyahPas encore d'évaluation
- Predictive Factors For Conversion of Laparoscopic CholecystectomyDocument4 pagesPredictive Factors For Conversion of Laparoscopic CholecystectomyGilang IrwansyahPas encore d'évaluation
- 2010 Article 156vhDocument6 pages2010 Article 156vhGilang IrwansyahPas encore d'évaluation
- Alvarado Scoring in Acute Appendicitis - A Clinicopathological CorrelationDocument4 pagesAlvarado Scoring in Acute Appendicitis - A Clinicopathological CorrelationGilang IrwansyahPas encore d'évaluation
- 2010 Article 33Document5 pages2010 Article 33Gilang IrwansyahPas encore d'évaluation
- AadhDocument1 pageAadhGilang IrwansyahPas encore d'évaluation
- Pertemuan 8Document3 pagesPertemuan 8Furi WigitaPas encore d'évaluation
- Hand Out 2Document2 pagesHand Out 2Christian Fel MoralitaPas encore d'évaluation
- Cataract PTDocument9 pagesCataract PTPreeti SharmaPas encore d'évaluation
- Modified Hemorrhoidal Artery Ligation Malang Procedure As An Alternative Therapy in Management of Haemorrhoid Grade IIIDocument4 pagesModified Hemorrhoidal Artery Ligation Malang Procedure As An Alternative Therapy in Management of Haemorrhoid Grade IIIInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Hormones and The Menstrual Cycle: Discussion GuideDocument11 pagesHormones and The Menstrual Cycle: Discussion GuideJohnryl FranciscoPas encore d'évaluation
- Posttraumatic Stress Disorder Epidemiology, Pathophysiology, Clinical Manifestations, and DiagnosisDocument9 pagesPosttraumatic Stress Disorder Epidemiology, Pathophysiology, Clinical Manifestations, and Diagnosisisa_horejsPas encore d'évaluation
- Reviewer 4th MapehDocument3 pagesReviewer 4th MapehMelanie B. DulfoPas encore d'évaluation
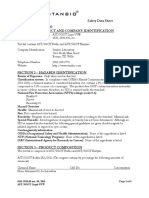
- MSDS - Stanbio SGOTDocument4 pagesMSDS - Stanbio SGOTDoni Eka PrasetiyoPas encore d'évaluation
- DrugStudy CarvedilolCasilaoDocument4 pagesDrugStudy CarvedilolCasilaoArone SebastianPas encore d'évaluation
- 11 Strategies To Fight CancerDocument73 pages11 Strategies To Fight CancerPayal Nandwana100% (1)
- Childhood Glaucoma: by Kelli OrdakowskiDocument16 pagesChildhood Glaucoma: by Kelli OrdakowskikmordakowskiPas encore d'évaluation
- Pubs/behres/bcr4theo - HTML Pada 26 September 2011: Daftar PustakaDocument22 pagesPubs/behres/bcr4theo - HTML Pada 26 September 2011: Daftar PustakareinzhordPas encore d'évaluation
- MCGRW HL S Npte M Dutton BK PDFDocument1 311 pagesMCGRW HL S Npte M Dutton BK PDFJack DowPas encore d'évaluation
- VutaminDocument66 pagesVutamindyla nabillaPas encore d'évaluation
- PHE For AdolescentsDocument26 pagesPHE For AdolescentsSanifa MedPas encore d'évaluation
- Q1 Prenatal CareDocument12 pagesQ1 Prenatal CareTash GuerraPas encore d'évaluation
- NCM 118 - Lesson 3 (Pulmonary Embolism)Document4 pagesNCM 118 - Lesson 3 (Pulmonary Embolism)Bobby Christian DuronPas encore d'évaluation
- Hypertensive Heart DiseasesDocument5 pagesHypertensive Heart DiseasesserubimPas encore d'évaluation
- DMA Ethics GuidelinesDocument51 pagesDMA Ethics GuidelinesTestePas encore d'évaluation
- Tri DoshaDocument7 pagesTri DoshaSKPas encore d'évaluation
- PNM Shaiha KKBB 2023Document15 pagesPNM Shaiha KKBB 2023haslinda84Pas encore d'évaluation
- Physical Fitness TestDocument5 pagesPhysical Fitness TestJhona Nodado RiveraPas encore d'évaluation
- Burning Mouth SyndromeDocument28 pagesBurning Mouth SyndromeMelissa KanggrianiPas encore d'évaluation
- That Sugar Film (2014) Directed by Damon GarneauDocument7 pagesThat Sugar Film (2014) Directed by Damon GarneauBai Fatima LumanggalPas encore d'évaluation
- Activity Completion Report: District of Basey IDocument2 pagesActivity Completion Report: District of Basey IRyan Adona GaddiPas encore d'évaluation