Vous aimerez peut-être aussi
- Is psoriasis linked to gut health? Study finds bile acids and plant compounds may treat skin conditionDocument32 pagesIs psoriasis linked to gut health? Study finds bile acids and plant compounds may treat skin conditionMACPANAMERAPas encore d'évaluation
- Major Functions of Boron in PlantsDocument3 pagesMajor Functions of Boron in PlantsQasim aliPas encore d'évaluation
- Dietary Changes To Prevent Calcium Oxalate Stones - tcm75-194243Document2 pagesDietary Changes To Prevent Calcium Oxalate Stones - tcm75-194243mecoyiPas encore d'évaluation
- Some Pediatrics Medicine Followed by The Tradisional MedicineDocument9 pagesSome Pediatrics Medicine Followed by The Tradisional Medicinedrrajalakshmi100% (3)
- Endocrine Effects of Prenatal Exposure PCBS, Dioxins, and Other Xenobiotics: Implications For Policy and Future ResearchDocument4 pagesEndocrine Effects of Prenatal Exposure PCBS, Dioxins, and Other Xenobiotics: Implications For Policy and Future ResearchAgent Orange LegacyPas encore d'évaluation
- Bar Soap vs. Liquid SoapDocument3 pagesBar Soap vs. Liquid SoapEdmar De Guzman JanePas encore d'évaluation
- Eating Pattern Questionnaire by American Medical AssociationDocument1 pageEating Pattern Questionnaire by American Medical AssociationNurSyuhadaAhmad100% (1)
- AloeliciousDocument25 pagesAloeliciousAlex Miguel GarciaPas encore d'évaluation
- Christine Schaffner Energy Hygiene EGuideDocument17 pagesChristine Schaffner Energy Hygiene EGuidevaleriabostanPas encore d'évaluation
- Cure All Types Of Headache Naturally Fast With AyurvedaDocument4 pagesCure All Types Of Headache Naturally Fast With AyurvedaSN WijesinhePas encore d'évaluation
- Endocrine DisruptorsDocument50 pagesEndocrine DisruptorsSnowangeleyes AngelPas encore d'évaluation
- Unesco - Eolss Sample Chapter: Plants As A Source of Anti-Cancer AgentsDocument15 pagesUnesco - Eolss Sample Chapter: Plants As A Source of Anti-Cancer AgentsSundararajan Jeyaraman100% (1)
- The Molecular Biology of How Dietary Supplements Support Optimal Human HealthDocument15 pagesThe Molecular Biology of How Dietary Supplements Support Optimal Human HealthKarlos Lds NvPas encore d'évaluation
- Lugol and GraveDocument6 pagesLugol and GraveSeptiandry Ade Putra100% (1)
- Phytotherapy 9Document8 pagesPhytotherapy 9Rahul PatilPas encore d'évaluation
- Is It Time To Fire Your DoctorDocument21 pagesIs It Time To Fire Your DoctorAshiraChayil100% (1)
- CancerDocument5 pagesCancerapi-3771269Pas encore d'évaluation
- Oligotherapy History MeaningDocument2 pagesOligotherapy History MeaningLuiz AlmeidaPas encore d'évaluation
- The Brain and BotanicalsDocument28 pagesThe Brain and BotanicalsbonziebodyPas encore d'évaluation
- "Herbal Antibiotics: A Research Review: A Project Report ofDocument25 pages"Herbal Antibiotics: A Research Review: A Project Report ofnawazPas encore d'évaluation
- Phthalates SummaryDocument25 pagesPhthalates SummarysunildutttripathiPas encore d'évaluation
- Advances in Integrative Medicine: Book ReviewDocument2 pagesAdvances in Integrative Medicine: Book ReviewVictor Raul JuramaPas encore d'évaluation
- Unik Aloe Vera PP PresentationDocument77 pagesUnik Aloe Vera PP PresentationTAMBAKI EDMOND100% (3)
- Scientific evidence for clinical use of horsetailDocument23 pagesScientific evidence for clinical use of horsetailDanilo Maciel Carneiro100% (1)
- Opuntia Ficus IndicaDocument8 pagesOpuntia Ficus IndicajpetinarakisPas encore d'évaluation
- Kundalini Reiki 1Document12 pagesKundalini Reiki 1anivallPas encore d'évaluation
- Cancer Treatment - TurkeyDocument16 pagesCancer Treatment - TurkeySaadet DagistanliPas encore d'évaluation
- 119th KSW Transcript EN Draft v1Document53 pages119th KSW Transcript EN Draft v1Miguel VegaPas encore d'évaluation
- Mechanism of the Anticancer Effect of PhytochemicalsD'EverandMechanism of the Anticancer Effect of PhytochemicalsPas encore d'évaluation
- CCWS™ Candida Cell Wall Suppressor Study ReviewDocument16 pagesCCWS™ Candida Cell Wall Suppressor Study ReviewCCWS Candida Cleanser Treatment Protocol100% (1)
- The Natural Cure To Your MigraineDocument97 pagesThe Natural Cure To Your Migraine---Pas encore d'évaluation
- Aging Glutathione and CysteineDocument5 pagesAging Glutathione and CysteineRandy GroverPas encore d'évaluation
- List of Genetically Transmitted DiseasesDocument3 pagesList of Genetically Transmitted DiseasesKara Mae Pagcanlungan Sugui100% (1)
- Bacteria Causing PulpitisDocument8 pagesBacteria Causing PulpitisMardiyah PratiwiPas encore d'évaluation
- Suzie BiofeedbackSDCRIDocument3 pagesSuzie BiofeedbackSDCRIocortezlariosPas encore d'évaluation
- Radionics AgriDocument4 pagesRadionics AgriNisha JoshiPas encore d'évaluation
- Tomato Products May Benefit Prostate HealthDocument4 pagesTomato Products May Benefit Prostate HealthSyahira AlmunPas encore d'évaluation
- How To Protect Against Radiation ExposureDocument7 pagesHow To Protect Against Radiation Exposurerichardck61100% (1)
- Vibration Training 2010Document2 pagesVibration Training 2010jithhtijPas encore d'évaluation
- 64 Positively Healing EssencesDocument32 pages64 Positively Healing EssenceskapiltondonPas encore d'évaluation
- In Vitro Culture of Orchids: The Roles of Class-1 Knox Gene in Shoot DevelopmentDocument10 pagesIn Vitro Culture of Orchids: The Roles of Class-1 Knox Gene in Shoot DevelopmentjammesPas encore d'évaluation
- Effects of Boron Deficiency and Excess On PlantsDocument13 pagesEffects of Boron Deficiency and Excess On PlantsSolve Et Coagula100% (1)
- EM WaveDocument13 pagesEM Wavekay100% (1)
- Cause of DiseaseDocument7 pagesCause of Diseaseparacelsus5Pas encore d'évaluation
- Safety Issues Affecting Herbs - Pyrrolizidine AlkaloidsDocument11 pagesSafety Issues Affecting Herbs - Pyrrolizidine AlkaloidsleyendosinpararPas encore d'évaluation
- Dr. Stevens's System of Medical ElectricityDocument20 pagesDr. Stevens's System of Medical Electricityaryaa2020Pas encore d'évaluation
- Blueprint for Free Plasma EnergyDocument18 pagesBlueprint for Free Plasma EnergyAnonymous Kti5jq5EJIPas encore d'évaluation
- Spirulina: The Benefit ofDocument5 pagesSpirulina: The Benefit ofRahmatin Lia100% (1)
- Raising Resilient Bees: Elevating A Hobby Into A CraftDocument3 pagesRaising Resilient Bees: Elevating A Hobby Into A CraftChelsea Green PublishingPas encore d'évaluation
- Preventive HealthDocument380 pagesPreventive HealthmurappanadPas encore d'évaluation
- Chakra Rotation and LayersDocument2 pagesChakra Rotation and LayerskatburnerPas encore d'évaluation
- Psoriasis Treatment by AnogenDocument27 pagesPsoriasis Treatment by AnogenAnogenPas encore d'évaluation
- Herbal ActionsDocument11 pagesHerbal ActionsG AnshuPas encore d'évaluation
- Keto Vegans Cookbook for Beginners: Take Pleasure and Become HealthierD'EverandKeto Vegans Cookbook for Beginners: Take Pleasure and Become HealthierPas encore d'évaluation
- Cell and Tissue Destruction: Mechanisms, Protection, DisordersD'EverandCell and Tissue Destruction: Mechanisms, Protection, DisordersPas encore d'évaluation
- A Slacker's Guide to Genetics: A Beginner's Guide to GeneticsD'EverandA Slacker's Guide to Genetics: A Beginner's Guide to GeneticsPas encore d'évaluation
- Fentanyl Inhibisi Kelenjar AdrenalDocument3 pagesFentanyl Inhibisi Kelenjar AdrenalGede Eka Putra NugrahaPas encore d'évaluation
- Fentanyl GlukosaDocument7 pagesFentanyl GlukosaGede Eka Putra NugrahaPas encore d'évaluation
- Evans SyndromeDocument13 pagesEvans SyndromerizeviPas encore d'évaluation
- Whipple Procedure: (Pancreaticoduodenectomy)Document13 pagesWhipple Procedure: (Pancreaticoduodenectomy)gamaPas encore d'évaluation
- Hazards of Endotracheal AnaesthesiaDocument12 pagesHazards of Endotracheal AnaesthesiaGede Eka Putra NugrahaPas encore d'évaluation
- 6 - Manajemen Perioperatif PD HipertensiDocument10 pages6 - Manajemen Perioperatif PD HipertensiOlief ShoppersPas encore d'évaluation
- Intraoperative Recruitment Manoeuvres: Protective Ventilation in The ORDocument7 pagesIntraoperative Recruitment Manoeuvres: Protective Ventilation in The ORGede Eka Putra NugrahaPas encore d'évaluation
- Child-Pugh Score: Patient Name: - DateDocument3 pagesChild-Pugh Score: Patient Name: - DateGede Eka Putra NugrahaPas encore d'évaluation
- Delirium (PM)Document9 pagesDelirium (PM)Dini Fajriah OmariPas encore d'évaluation
- Update On The Management of LaryngospasmDocument6 pagesUpdate On The Management of LaryngospasmGede Eka Putra NugrahaPas encore d'évaluation
- LN Class IV Fauci 2008Document1 pageLN Class IV Fauci 2008Gede Eka Putra NugrahaPas encore d'évaluation
- Ambulance OperationDocument11 pagesAmbulance OperationGede Eka Putra NugrahaPas encore d'évaluation
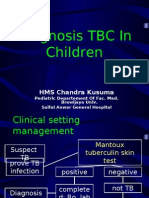
- Diagnosis TBDocument44 pagesDiagnosis TBGede Eka Putra NugrahaPas encore d'évaluation
- Diagnosis TBDocument44 pagesDiagnosis TBGede Eka Putra NugrahaPas encore d'évaluation
- Kesehatan Anak Slide Acute Renal FailureDocument21 pagesKesehatan Anak Slide Acute Renal FailureBasory Ok OkPas encore d'évaluation
- Levenson Am JPsychiat 85Document9 pagesLevenson Am JPsychiat 85Gede Eka Putra NugrahaPas encore d'évaluation
- Pathogenesis TBDocument39 pagesPathogenesis TBGede Eka Putra NugrahaPas encore d'évaluation
- Treatment TBDocument43 pagesTreatment TBGede Eka Putra NugrahaPas encore d'évaluation
- Soil Mechanics (Richard Brachman)Document158 pagesSoil Mechanics (Richard Brachman)api-3763023100% (3)
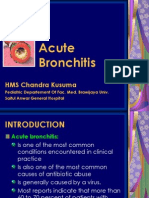
- Acute Bronchitis: HMS Chandra KusumaDocument16 pagesAcute Bronchitis: HMS Chandra KusumaGede Eka Putra NugrahaPas encore d'évaluation
- Case Summary 1Document75 pagesCase Summary 1Faryad HussainPas encore d'évaluation
- Icar JRFDocument12 pagesIcar JRFᗬᗴᐻ ᔤᗩᕼᕢᖆᘍ80% (5)
- Ibn SinaDocument2 pagesIbn SinaWaris Husain0% (1)
- Enoxaparin FDADocument40 pagesEnoxaparin FDAImam Nur Alif Khusnudin100% (2)
- Head and Neck TumorsDocument14 pagesHead and Neck TumorsBarda GulanPas encore d'évaluation
- EMP Env. Law in NepalDocument43 pagesEMP Env. Law in NepalSeba Videla GPas encore d'évaluation
- Cast, Brace, Traction CompilationDocument13 pagesCast, Brace, Traction CompilationMar Ordanza100% (1)
- DSM-5 Changes to Psychotic and Mood Disorder CriteriaDocument9 pagesDSM-5 Changes to Psychotic and Mood Disorder CriteriaMonika LangngagPas encore d'évaluation
- Giving Advice:: Should/Shouldn'tDocument3 pagesGiving Advice:: Should/Shouldn'tPATRICIA APARECIDA DA SILVAPas encore d'évaluation
- Mh-Somatic Symptom Disorders - 2Document9 pagesMh-Somatic Symptom Disorders - 2martinPas encore d'évaluation
- A Review On Phytochemical and Pharmacological Properties of Holy 2018 PDFDocument16 pagesA Review On Phytochemical and Pharmacological Properties of Holy 2018 PDFCDB 1st Semester 2077Pas encore d'évaluation
- BP PGD CausticDocument36 pagesBP PGD Causticasni_rahayu9020Pas encore d'évaluation
- Genetic Disorder Brochure ProjectDocument1 pageGenetic Disorder Brochure ProjectErika ContrerasPas encore d'évaluation
- Philippine Health Care LawsDocument5 pagesPhilippine Health Care LawstonytorrejonPas encore d'évaluation
- MitochondriaDocument6 pagesMitochondriakevin smithPas encore d'évaluation
- November 2009 Final EditionDocument45 pagesNovember 2009 Final Editionaajo136Pas encore d'évaluation
- Maternal Serum Alpha-Fetoprotein (MSAFP)Document2 pagesMaternal Serum Alpha-Fetoprotein (MSAFP)Shaells JoshiPas encore d'évaluation
- 1 MSN UNIT 1introductionDocument57 pages1 MSN UNIT 1introductionVikash PrajapatiPas encore d'évaluation
- Circular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاDocument2 pagesCircular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاErin JohnsonPas encore d'évaluation
- Victus Brochure 2011 WEBDocument45 pagesVictus Brochure 2011 WEBArunkumar RamasamyPas encore d'évaluation
- Microbiology IntroductionDocument2 pagesMicrobiology IntroductionAnonymous XuiUo2ThPas encore d'évaluation
- Paket 4Document6 pagesPaket 4Lovis ShalahuddinPas encore d'évaluation
- The Rules of The Cancer Patient Diet and Dr. Hammer GNMDocument71 pagesThe Rules of The Cancer Patient Diet and Dr. Hammer GNMshivapuja100% (1)
- How Do We Take Care of Our Endocrine SystemDocument7 pagesHow Do We Take Care of Our Endocrine SystemAndrei CunananPas encore d'évaluation
- Nefropatía Por Cilindros Biliares Asociada A Disfunción Hepática Severa Causada Por Esteroides AnabolizantesDocument3 pagesNefropatía Por Cilindros Biliares Asociada A Disfunción Hepática Severa Causada Por Esteroides AnabolizantesKarla JazminPas encore d'évaluation
- ENGLISHDocument22 pagesENGLISHears bonifacioPas encore d'évaluation
- Porcelain Fused To Metal (PFM) Crowns and Caries in Adjacent TeetDocument5 pagesPorcelain Fused To Metal (PFM) Crowns and Caries in Adjacent Teetbaiq rengganis dewiPas encore d'évaluation
- I. Answer The Following Questions Based On The Audio atDocument4 pagesI. Answer The Following Questions Based On The Audio atlalaPas encore d'évaluation
- Pro-Lab: Salmonella AntiseraDocument2 pagesPro-Lab: Salmonella Antiseraapi-3742158Pas encore d'évaluation
- Tryptic Soy Agar - Trypticase Soy Agar (Soybean-Casein Digest Agar)Document4 pagesTryptic Soy Agar - Trypticase Soy Agar (Soybean-Casein Digest Agar)Fred GreenPas encore d'évaluation