Vous aimerez peut-être aussi
- Critical Incidence Reporting & Learning PDFDocument7 pagesCritical Incidence Reporting & Learning PDFNenny Puji LestariPas encore d'évaluation
- Patient Safety Officer 2009 Annual ReportDocument36 pagesPatient Safety Officer 2009 Annual ReportRyan McNeillPas encore d'évaluation
- Slips, Trips and Falls in Hospital: WWW - Npsa.nhs - UkDocument72 pagesSlips, Trips and Falls in Hospital: WWW - Npsa.nhs - Ukjojimathew03Pas encore d'évaluation
- NRLSDocument16 pagesNRLSDounia MarbouhPas encore d'évaluation
- Making Health Care Safer.2Document9 pagesMaking Health Care Safer.2YANPas encore d'évaluation
- Effectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsDocument8 pagesEffectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsNurul AidaPas encore d'évaluation
- Ontario Health Technology Assessment SeriesDocument73 pagesOntario Health Technology Assessment SeriesCassie AbernathPas encore d'évaluation
- 9pscssicurrentDocument41 pages9pscssicurrentDavid Mayo FigueroaPas encore d'évaluation
- Quality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonDocument8 pagesQuality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonMulyawan Safwandy NugrahaPas encore d'évaluation
- Literature Review Infections Associated With Peripheral Venous Access deDocument100 pagesLiterature Review Infections Associated With Peripheral Venous Access deIswenti NoveraPas encore d'évaluation
- Managing Patient Access and Flow in The Emergency Department To Improve Patient SafetyDocument13 pagesManaging Patient Access and Flow in The Emergency Department To Improve Patient SafetyAli ErenPas encore d'évaluation
- Early Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsDocument28 pagesEarly Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsRosmira Agreda CabreraPas encore d'évaluation
- Measure To Know: An Approach To Improve Surgical Outcomes in A Surgical DepartmentDocument23 pagesMeasure To Know: An Approach To Improve Surgical Outcomes in A Surgical DepartmentlgrandePas encore d'évaluation
- Paula Grace EduvaneDocument80 pagesPaula Grace EduvaneDennisIgoyDacanayPas encore d'évaluation
- 9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEDocument12 pages9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEmiftakhul jannahPas encore d'évaluation
- Zhan2008 Article CardiacDeviceImplantationInTheDocument7 pagesZhan2008 Article CardiacDeviceImplantationInTheBeto RamirezPas encore d'évaluation
- Clinical Risk ManagementDocument6 pagesClinical Risk ManagementJaparaj PeterPas encore d'évaluation
- R F I R: Edesigning The ALL Ncident EportDocument9 pagesR F I R: Edesigning The ALL Ncident EportShePas encore d'évaluation
- Data Collection ProtocolDocument2 pagesData Collection ProtocolSinung BawonoPas encore d'évaluation
- Roils PaperDocument4 pagesRoils Paperapi-575843507Pas encore d'évaluation
- Linking Lean Healthcare To Six Sigma: An Emergency Department Case StudyDocument14 pagesLinking Lean Healthcare To Six Sigma: An Emergency Department Case StudyEduardo Castillo AlvaradoPas encore d'évaluation
- Pcsmanual CurrentDocument408 pagesPcsmanual CurrentQMMC NursingPas encore d'évaluation
- Pcsmanual Current PDFDocument355 pagesPcsmanual Current PDFArgadia YuniriyadiPas encore d'évaluation
- Patient Safety - 2019 PDFDocument355 pagesPatient Safety - 2019 PDFnisaPas encore d'évaluation
- Serious Reportable Adverse Events in Health Care: Kenneth W. Kizer, Melissa B. StegunDocument14 pagesSerious Reportable Adverse Events in Health Care: Kenneth W. Kizer, Melissa B. StegunThanh Doan ThiPas encore d'évaluation
- Point of Care DiagnosticsDocument109 pagesPoint of Care Diagnosticschhatra0% (1)
- Malaysian Patient Safety Goals Technical SpecsDocument18 pagesMalaysian Patient Safety Goals Technical Specsprisma1Pas encore d'évaluation
- RCA Sentinel EventsDocument4 pagesRCA Sentinel EventsGabriela FrederickPas encore d'évaluation
- Health informatics: Improving patient careD'EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITÉvaluation : 3 sur 5 étoiles3/5 (1)
- CDC Surgical Site Infection GuideDocument39 pagesCDC Surgical Site Infection GuideNor KongPas encore d'évaluation
- Writing TaskDocument2 pagesWriting TaskAnggi Satria SiburianPas encore d'évaluation
- Monitoring Preventable Adverse Events and Near.9Document6 pagesMonitoring Preventable Adverse Events and Near.9danny widjajaPas encore d'évaluation
- 680 FullDocument9 pages680 FullRye CalderonPas encore d'évaluation
- Performance Indicators For Hospital Emergency Departments ManagementDocument12 pagesPerformance Indicators For Hospital Emergency Departments ManagementNehal KhalafPas encore d'évaluation
- JournalDocument5 pagesJournalCris TanPas encore d'évaluation
- Needlestick InjuryDocument24 pagesNeedlestick InjuryAli AlisonPas encore d'évaluation
- NHSN Manual OverviewDocument445 pagesNHSN Manual OverviewDayana RodriguezPas encore d'évaluation
- BMC Health Services ResearchDocument7 pagesBMC Health Services Researchuei_enyd2004Pas encore d'évaluation
- "Virtual" Trials: Case Control Experiments Utilizing Health Services Research WorkstationDocument5 pages"Virtual" Trials: Case Control Experiments Utilizing Health Services Research WorkstationKang Opik TaufikPas encore d'évaluation
- Patient Safety 1, 2Document98 pagesPatient Safety 1, 2salah salem100% (1)
- Care Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WereDocument10 pagesCare Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WerenanikPas encore d'évaluation
- Surgical Site Infection Event (SSI) : January 2022Document39 pagesSurgical Site Infection Event (SSI) : January 2022Amanuel TamiruPas encore d'évaluation
- Classifying Healthcare Innovations ActivityDocument3 pagesClassifying Healthcare Innovations ActivityAlejandro CardonaPas encore d'évaluation
- Department of Health and Human Services: Payments ForDocument32 pagesDepartment of Health and Human Services: Payments Formarkv93Pas encore d'évaluation
- Key Terms of EHRs and Examples in Various Types of Care SettingsDocument10 pagesKey Terms of EHRs and Examples in Various Types of Care SettingsDariaZhuravlevaPas encore d'évaluation
- AQI Is The Definition of QualityDocument3 pagesAQI Is The Definition of QualityeryxspPas encore d'évaluation
- Surveillance SystemDocument49 pagesSurveillance Systemjeevan ghimirePas encore d'évaluation
- Coursematerial 214Document16 pagesCoursematerial 214Francisco Reyes IslaPas encore d'évaluation
- CDC Surveilance 2018Document321 pagesCDC Surveilance 2018spiderPas encore d'évaluation
- MSQH Performance Indicators - 6th Edition (Complete Set of Performance Indicators)Document274 pagesMSQH Performance Indicators - 6th Edition (Complete Set of Performance Indicators)Nabila Huda100% (1)
- Week2 Submitter PaperDocument3 pagesWeek2 Submitter Paperapi-299189797Pas encore d'évaluation
- Applying Simulation and Six Sigma to Improve ED ProcessDocument0 pageApplying Simulation and Six Sigma to Improve ED ProcessdeepakjothivelPas encore d'évaluation
- A Practical Guide To Healthcare DataDocument20 pagesA Practical Guide To Healthcare DataGeorge Tanaruno100% (1)
- Patient Safety Thesis PDFDocument6 pagesPatient Safety Thesis PDFasiagroverprovo100% (2)
- Guide Lines in Surgical Quality ServiceDocument23 pagesGuide Lines in Surgical Quality ServiceAddis YeshitlaPas encore d'évaluation
- A Checklist To Improve Patient Safety in Interventional RadiologyDocument8 pagesA Checklist To Improve Patient Safety in Interventional Radiologyaegysabetterway100% (1)
- A Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayDocument7 pagesA Review of Medical Errors in Laboratory Diagnostics and Where We Are TodayRobert MaynardPas encore d'évaluation
- Journal of Continuing Education in Nursing. 40 (5) :221-7, 2009 MayDocument10 pagesJournal of Continuing Education in Nursing. 40 (5) :221-7, 2009 MayJessica GabejanPas encore d'évaluation
- Patient Information Systems in The LiteratureDocument6 pagesPatient Information Systems in The LiteratureJohn MunaonyediPas encore d'évaluation
- SensorssorDocument52 pagesSensorssorDeepak BujahiPas encore d'évaluation
- File Related Commands:: Cat Command: This Command Is Used To Create A File. Syntax: $cat FilenameDocument12 pagesFile Related Commands:: Cat Command: This Command Is Used To Create A File. Syntax: $cat FilenameDeepak BujahiPas encore d'évaluation
- 59-Tending Pets 2Document2 pages59-Tending Pets 2Deepak BujahiPas encore d'évaluation
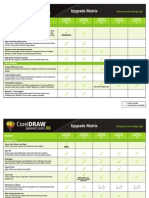
- CorelDraw X6 Version ComparisonDocument11 pagesCorelDraw X6 Version ComparisonFrans van BeersPas encore d'évaluation
- Law Colleges in KarnatakaDocument5 pagesLaw Colleges in KarnatakaDeepak BujahiPas encore d'évaluation
- GRAPHICS Lab ReportDocument70 pagesGRAPHICS Lab ReportFahad AhmadPas encore d'évaluation
- Citizenn Interface ModuleDocument4 pagesCitizenn Interface ModuleDeepak BujahiPas encore d'évaluation
- Directory Related Commands:: Mkdir Command: This Command Is Used To Create A Directory. Syntax: $mkdir File NameDocument4 pagesDirectory Related Commands:: Mkdir Command: This Command Is Used To Create A Directory. Syntax: $mkdir File NameDeepak BujahiPas encore d'évaluation
- (WWW - Entrance-Exam - Net) - PTU MCA 3rd Semester Sample Paper 4Document2 pages(WWW - Entrance-Exam - Net) - PTU MCA 3rd Semester Sample Paper 4Mangesh MalvankarPas encore d'évaluation
- Seearch ModuleDocument7 pagesSeearch ModuleDeepak BujahiPas encore d'évaluation
- Set2 - Transport & NetworkDocument155 pagesSet2 - Transport & NetworkRashmi GandhiPas encore d'évaluation
- Gauss JordanDocument3 pagesGauss JordanDeepak BujahiPas encore d'évaluation
- IELTS Essay Topics (Task 1)Document96 pagesIELTS Essay Topics (Task 1)Si Le100% (6)
- Unit1 JWFILESDocument41 pagesUnit1 JWFILESRajashekar ReddyPas encore d'évaluation
- Ielts Task 2 6 Sample EssaysDocument7 pagesIelts Task 2 6 Sample EssaysSungjin ParkPas encore d'évaluation
- 21 Ways To Have A High Scoring IELTS ExamDocument7 pages21 Ways To Have A High Scoring IELTS ExamDeepak BujahiPas encore d'évaluation
- 3 2212Document1 page3 2212Deepak BujahiPas encore d'évaluation
- IELTS Essay: The Rubbish ProblemDocument5 pagesIELTS Essay: The Rubbish ProblemDomingo2611Pas encore d'évaluation
- Ielts EssayDocument34 pagesIelts EssayTinu Anna GeorgePas encore d'évaluation
- Step by Step Guide To Install Microsoft Windows XP ProfessionalDocument68 pagesStep by Step Guide To Install Microsoft Windows XP ProfessionalRambo IIIPas encore d'évaluation
- Art History 1993Document5 pagesArt History 1993Deepak BujahiPas encore d'évaluation
- Atonement 6Document5 pagesAtonement 6Deepak BujahiPas encore d'évaluation
- Arianism 6Document8 pagesArianism 6Deepak BujahiPas encore d'évaluation
- Art in The BibleDocument2 pagesArt in The BibleDeepak BujahiPas encore d'évaluation
- ArianismDocument8 pagesArianismDeepak BujahiPas encore d'évaluation
- Anglo Saxon Belief in Fate and ChristianityDocument2 pagesAnglo Saxon Belief in Fate and ChristianityDeepak BujahiPas encore d'évaluation
- Art in The Bible 6Document2 pagesArt in The Bible 6Deepak BujahiPas encore d'évaluation
- ApocalypseDocument7 pagesApocalypseDeepak BujahiPas encore d'évaluation
- Apocalypse 6Document7 pagesApocalypse 6Deepak BujahiPas encore d'évaluation
- Bio Medical Engineer On Contract BasisDocument3 pagesBio Medical Engineer On Contract BasisSreedhar RajaPas encore d'évaluation
- Margin Elevation Technique PDFDocument6 pagesMargin Elevation Technique PDFUsman SanaPas encore d'évaluation
- Prasugrel and RosuvastatinDocument7 pagesPrasugrel and RosuvastatinMohammad Shahbaz AlamPas encore d'évaluation
- Changes in Central Corneal Thickness in Healthy Pregnant Women-A Clinical StudyDocument3 pagesChanges in Central Corneal Thickness in Healthy Pregnant Women-A Clinical StudyIJAR JOURNALPas encore d'évaluation
- Goals and principles of community health nursingDocument4 pagesGoals and principles of community health nursingNoemiPas encore d'évaluation
- Taking Medical HistoryDocument2 pagesTaking Medical HistoryDiana KulsumPas encore d'évaluation
- Labor Pain ManagementDocument1 pageLabor Pain ManagementKenneth Sy100% (5)
- Assessment 7Document5 pagesAssessment 7api-525782290Pas encore d'évaluation
- Case StudyDocument6 pagesCase StudyMattPas encore d'évaluation
- Lincomycin: Drug Information: ALERT: US Boxed WarningDocument12 pagesLincomycin: Drug Information: ALERT: US Boxed WarningsadiaPas encore d'évaluation
- The Encyclopedia of Sexually Transmitted DiseasesDocument353 pagesThe Encyclopedia of Sexually Transmitted DiseasesLaura ZabiskyFlorestaPas encore d'évaluation
- Restraints Assignment on Definitions, Types, Indications and Nurses RoleDocument8 pagesRestraints Assignment on Definitions, Types, Indications and Nurses RolemacmohitPas encore d'évaluation
- Cutaneous MelanomaDocument226 pagesCutaneous MelanomaGriskalia ChristinePas encore d'évaluation
- NEET UG Biology Human Health and DiseasesDocument18 pagesNEET UG Biology Human Health and DiseasesMansoor MalikPas encore d'évaluation
- Fact Sheet 1 - Addiction OverviewDocument5 pagesFact Sheet 1 - Addiction Overviewgoldbergleah100% (1)
- Methods For The Euthanasia of Dogs and Cats - EnglishDocument28 pagesMethods For The Euthanasia of Dogs and Cats - Englishapi-266985430Pas encore d'évaluation
- Geriatric Medicine Certification Examination Blueprint - ABIMDocument7 pagesGeriatric Medicine Certification Examination Blueprint - ABIMabimorgPas encore d'évaluation
- Aiims Hospital Disaster PlanDocument6 pagesAiims Hospital Disaster PlanSujatha J JayabalPas encore d'évaluation
- Classification of FracturesDocument26 pagesClassification of FracturesHoney May Rollan VicentePas encore d'évaluation
- تجميعات باثولوجيDocument3 pagesتجميعات باثولوجيTurky TurkyPas encore d'évaluation
- Guía OxigenoterapiaDocument39 pagesGuía OxigenoterapiaSMIBA MedicinaPas encore d'évaluation
- U.S. clinical observerships help IMGs gain experienceDocument8 pagesU.S. clinical observerships help IMGs gain experienceAkshit ChitkaraPas encore d'évaluation
- Standards of Medical Care in Diabetes-2022Document10 pagesStandards of Medical Care in Diabetes-2022Adina SimionPas encore d'évaluation
- Differences in Housemen Performance from CUCMS and Other Medical SchoolsDocument10 pagesDifferences in Housemen Performance from CUCMS and Other Medical SchoolsAfif AizatPas encore d'évaluation
- AssociationBetweenBRAFV600EMutationand MortalityDocument9 pagesAssociationBetweenBRAFV600EMutationand MortalityMade RusmanaPas encore d'évaluation
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On PsychiatryMing Wang50% (6)
- German Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchDocument8 pagesGerman Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchKarla VegaPas encore d'évaluation
- Ibuprofen - Pharmacology, Therapeutics and Side Effects. 2012Document260 pagesIbuprofen - Pharmacology, Therapeutics and Side Effects. 2012VuqarPas encore d'évaluation
- Performance Review NPDocument11 pagesPerformance Review NPtmlePas encore d'évaluation
- Apollo Hospitals: Porters Generic FrameworkDocument6 pagesApollo Hospitals: Porters Generic FrameworkVaibhav AroraPas encore d'évaluation