Vous aimerez peut-être aussi
- Encycl in Neuro PsyDocument2 813 pagesEncycl in Neuro PsyAnonymous haOGKg8JUV100% (2)
- Cervical PainDocument15 pagesCervical Painsteffiecruz06Pas encore d'évaluation
- Sue Falsone Bridging The Gap Chapter One Excerpt1 PDFDocument14 pagesSue Falsone Bridging The Gap Chapter One Excerpt1 PDFAléssio Novais100% (2)
- Bubble Inclinometer Measurement Chart PDFDocument2 pagesBubble Inclinometer Measurement Chart PDFsyedqutub16Pas encore d'évaluation
- Kamars RadiologyDocument135 pagesKamars RadiologyNayantara Nair100% (1)
- Cervical DisordersDocument89 pagesCervical DisordersAbdallah Samir Mostafa٢٠١٩٠٢١٥٩Pas encore d'évaluation
- Assessment of Back Pain-BMJDocument30 pagesAssessment of Back Pain-BMJMarco Paulo Reyes NaoePas encore d'évaluation
- Physiotherapy MOPDocument20 pagesPhysiotherapy MOPHbk RajneeshPas encore d'évaluation
- The Challenge of Managing Mid-Foot Pain: BackgroundDocument6 pagesThe Challenge of Managing Mid-Foot Pain: BackgroundIsha WuPas encore d'évaluation
- Design of A Hand OrthosisDocument251 pagesDesign of A Hand OrthosisIsrael BlancoPas encore d'évaluation
- Rehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryDocument11 pagesRehab Plans and Exercises Minor Rotator Cuff Repair Protocol For Physiotherapy Following SurgeryTech How AssamPas encore d'évaluation
- Lumbar Spine AssesmentDocument8 pagesLumbar Spine AssesmentPavithra SivanathanPas encore d'évaluation
- Examination of v. SystemDocument64 pagesExamination of v. SystemYibeltalPas encore d'évaluation
- Shoulder Pain and Disability Index (SPADI)Document2 pagesShoulder Pain and Disability Index (SPADI)M Ilham ArifiansyahPas encore d'évaluation
- Red Flag: MSK Services Pathway - Shoulder PathologyDocument11 pagesRed Flag: MSK Services Pathway - Shoulder PathologyMuhammed ElgasimPas encore d'évaluation
- Wound Care MangementDocument17 pagesWound Care Mangementdian lukman hakimPas encore d'évaluation
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementD'EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementPas encore d'évaluation
- Home Exercise ProgramDocument6 pagesHome Exercise ProgramRavin NarwalPas encore d'évaluation
- Orthopediatric LWWDocument398 pagesOrthopediatric LWWかちえ ちょうPas encore d'évaluation
- SCI Acute Care and Rehabilitation PT 2009Document265 pagesSCI Acute Care and Rehabilitation PT 2009api-3822828Pas encore d'évaluation
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÉvaluation : 4 sur 5 étoiles4/5 (2)
- Clinical Signs - NamedDocument9 pagesClinical Signs - NamedsprapurPas encore d'évaluation
- Health and Wellness GuideDocument16 pagesHealth and Wellness GuideLara LovePas encore d'évaluation
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Manual TherapyDocument16 pagesManual TherapylecturioPas encore d'évaluation
- The OT Role in Rehabilitation For The Person With An Upper-Limb AmputationDocument2 pagesThe OT Role in Rehabilitation For The Person With An Upper-Limb AmputationThe American Occupational Therapy AssociationPas encore d'évaluation
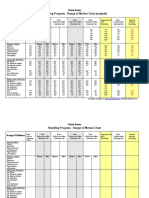
- Standing Program - Range of Motion Chart (Sample) : Client NameDocument2 pagesStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezPas encore d'évaluation
- Orthosisofhandppt 181202162551Document65 pagesOrthosisofhandppt 181202162551Khageswar SamalPas encore d'évaluation
- Upper Body Thera Band Exercise Program - BasicDocument7 pagesUpper Body Thera Band Exercise Program - Basicakheel ahammed100% (1)
- Pain Measurement PDFDocument13 pagesPain Measurement PDFDragos GarofilPas encore d'évaluation
- Upper Extremity AmputationDocument24 pagesUpper Extremity AmputationvirginiaPas encore d'évaluation
- Marshall 2015Document13 pagesMarshall 2015MalikinNadalPas encore d'évaluation
- Malignant Spinal Cord Compression - Dealing The Most Common - MetsDocument60 pagesMalignant Spinal Cord Compression - Dealing The Most Common - MetsDr Sasikumar Sambasivam100% (2)
- Shoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFDocument31 pagesShoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFRulyPas encore d'évaluation
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryPas encore d'évaluation
- Fracture Colles Wrist Exercise-AfterDocument4 pagesFracture Colles Wrist Exercise-Afterfaprilisa100% (1)
- INTRODUCTION MSC 1t Yr Nursing EducationDocument19 pagesINTRODUCTION MSC 1t Yr Nursing EducationPooja Vishwakarma78% (9)
- Joint ROMDocument2 pagesJoint ROMdr_gentel19Pas encore d'évaluation
- Foam Roller TherapyDocument8 pagesFoam Roller TherapyLucia Constantinescu75% (4)
- TRX PDFDocument38 pagesTRX PDFAllPas encore d'évaluation
- Norkin, C. C., & White, D. J. (2009) - Measurement of Joint Motion: A Guide To Goniometry. Philadelphia: F.A. Davis. jdcptrp2019Document12 pagesNorkin, C. C., & White, D. J. (2009) - Measurement of Joint Motion: A Guide To Goniometry. Philadelphia: F.A. Davis. jdcptrp2019Anne SerneoPas encore d'évaluation
- Shoulder Knee WristDocument110 pagesShoulder Knee Wriststevebravo81100% (1)
- AAPMR - What Makes The Practice of Physiatry MultidisciplinaryDocument3 pagesAAPMR - What Makes The Practice of Physiatry MultidisciplinaryJared CoganPas encore d'évaluation
- Cervical Spondylosis and Neck PainDocument5 pagesCervical Spondylosis and Neck PainIsaac AlemanPas encore d'évaluation
- AOTA New Guidelines For Functional Reassessments Ad Documentation in Home HealthDocument4 pagesAOTA New Guidelines For Functional Reassessments Ad Documentation in Home HealthIris De La CalzadaPas encore d'évaluation
- Department of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017Document24 pagesDepartment of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017aritrisnawatiPas encore d'évaluation
- ABOS Sports Acceptable CPT CodesDocument13 pagesABOS Sports Acceptable CPT CodesFrank CookPas encore d'évaluation
- Overview of Tool and Key Points: Section A: HistoryDocument4 pagesOverview of Tool and Key Points: Section A: HistoryM Naeem ArhamPas encore d'évaluation
- Rehab - NotesDocument8 pagesRehab - Noteschris blacPas encore d'évaluation
- Low Back Pain Presentation IMPDocument114 pagesLow Back Pain Presentation IMPrapannika100% (3)
- Development Chart For BookletDocument13 pagesDevelopment Chart For BookletzapelPas encore d'évaluation
- GWS Total Hip ReplacementDocument17 pagesGWS Total Hip ReplacementRadu MoglanPas encore d'évaluation
- App1 Pain Rating ScalesDocument4 pagesApp1 Pain Rating Scalesthilaga88Pas encore d'évaluation
- De Quervain SyndromeDocument5 pagesDe Quervain Syndromebangla018Pas encore d'évaluation
- About PRPDocument5 pagesAbout PRPAllanSalardaAdemPas encore d'évaluation
- Sci Bladder ProtocolDocument45 pagesSci Bladder ProtocolAbbas JafarzadehabbasPas encore d'évaluation
- Hemiarthroplasty Hip - Apr20Document10 pagesHemiarthroplasty Hip - Apr20Shalu OjhaPas encore d'évaluation
- Dyspnea Best PracticesDocument23 pagesDyspnea Best PracticesShivaniPas encore d'évaluation
- Manual Therapy For Musculoskeletal Pain Syndromes, 1st EditionDocument16 pagesManual Therapy For Musculoskeletal Pain Syndromes, 1st EditionMaansi GuptaPas encore d'évaluation
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarPas encore d'évaluation
- Sci RehabDocument45 pagesSci RehabkaushikawebPas encore d'évaluation
- Elbow Instability Anatomy BiomechanicsDocument9 pagesElbow Instability Anatomy BiomechanicsSPerOrtPas encore d'évaluation
- Hip Spica Nursing CareDocument10 pagesHip Spica Nursing CareItstineePas encore d'évaluation
- Gluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDocument13 pagesGluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDaniela Villablanca100% (1)
- Intravenous TherapyDocument48 pagesIntravenous TherapyFrancr ToledanoPas encore d'évaluation
- Elbow Injuires and SportDocument12 pagesElbow Injuires and SportSurgicalgownPas encore d'évaluation
- Phys Ther 2010 Weppler 438 49Document15 pagesPhys Ther 2010 Weppler 438 49Gaman IulianPas encore d'évaluation
- Rotator CuffDocument5 pagesRotator CufflizardbeePas encore d'évaluation
- Fulk 2011 Stroke Gait SpeedDocument8 pagesFulk 2011 Stroke Gait SpeedlizardbeePas encore d'évaluation
- Pyramida SpecDocument2 pagesPyramida SpeclizardbeePas encore d'évaluation
- Lim 2011 Pilates Exs and LBPDocument11 pagesLim 2011 Pilates Exs and LBPlizardbeePas encore d'évaluation
- ADDENDUM - Addendum To Advt - No.P&A.II-10-JSSC-SCTIMST-2022, Dated 23.02.2022Document2 pagesADDENDUM - Addendum To Advt - No.P&A.II-10-JSSC-SCTIMST-2022, Dated 23.02.2022monishaPas encore d'évaluation
- Yataco2019.Early Progressive Mobilization of Patients With EVD. Safety An FeasibilityDocument7 pagesYataco2019.Early Progressive Mobilization of Patients With EVD. Safety An FeasibilityEviPas encore d'évaluation
- Timms Carus - Lit Review On Mirror Therapy To Alleviate Phantom Limb PainDocument12 pagesTimms Carus - Lit Review On Mirror Therapy To Alleviate Phantom Limb Painapi-435636207Pas encore d'évaluation
- Day 3 Principles of Rehabilitation in Elderly The NewestDocument43 pagesDay 3 Principles of Rehabilitation in Elderly The NewestaniendyawijayaPas encore d'évaluation
- Listening Is Therapy: Patient Interviewing From A Pain Science PerspectiveDocument12 pagesListening Is Therapy: Patient Interviewing From A Pain Science PerspectiveGilbert ThierryPas encore d'évaluation
- Reimbursement of Medical Claims2Document5 pagesReimbursement of Medical Claims2Doctor 07Pas encore d'évaluation
- DISABILITYDocument8 pagesDISABILITYahmedPas encore d'évaluation
- Equipment CatalogueDocument18 pagesEquipment CatalogueSylvia LoongPas encore d'évaluation
- Physical Therapy Exe SheetDocument232 pagesPhysical Therapy Exe SheetShahzad AliPas encore d'évaluation
- SAFEMOB Final18673Document2 pagesSAFEMOB Final18673Muhammad FarisPas encore d'évaluation
- History, Evolution & Classification of HospitalsDocument10 pagesHistory, Evolution & Classification of HospitalsAnonymous ibmeej9100% (1)
- Test Bank For Therapeutic Exercise Foundations and Techniques 6th Edition by KisnerDocument31 pagesTest Bank For Therapeutic Exercise Foundations and Techniques 6th Edition by Kisnerpachyunmuzzleimshbk100% (28)
- Inspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialDocument8 pagesInspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialMuhammad AbdullahPas encore d'évaluation
- A CBT-based Approach To Medically Unexplained Symptoms: ArticleDocument7 pagesA CBT-based Approach To Medically Unexplained Symptoms: Articleaastha jainPas encore d'évaluation
- Lesson 7 Rehabilitation Program Lesson 8 Bureau of Corrections Rehabilitation ProgramDocument22 pagesLesson 7 Rehabilitation Program Lesson 8 Bureau of Corrections Rehabilitation ProgramDaks GameplayPas encore d'évaluation
- 1076 PDFDocument157 pages1076 PDFSri Charan ReddyPas encore d'évaluation
- Clinical - Bulletin - Physical Therapy in MS RehabilitationDocument17 pagesClinical - Bulletin - Physical Therapy in MS RehabilitationSoom RamadanPas encore d'évaluation
- AHM Black White Boost FlexiDocument10 pagesAHM Black White Boost FlexiDani Kirky Ylagan100% (1)
- Concept Sheet Specialized Health and Medical Rehabilitation CenterDocument3 pagesConcept Sheet Specialized Health and Medical Rehabilitation CenterAine OdalerPas encore d'évaluation
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051Document8 pagesA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051sebafigueroa94Pas encore d'évaluation
- Article 10Document8 pagesArticle 10Hamza DibPas encore d'évaluation
- Woman's HealthDocument3 pagesWoman's HealthMahmoud Abo AlfaPas encore d'évaluation