Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- High Risk Pregnancy (Notes)Document17 pagesHigh Risk Pregnancy (Notes)rhenier_ilado100% (10)
- Maternal & Child Practice Exam 4 - RNpediaDocument21 pagesMaternal & Child Practice Exam 4 - RNpediaLot Rosit100% (1)
- H-Mole Chapter I-VDocument103 pagesH-Mole Chapter I-VJoevence Gazo CuaresmaPas encore d'évaluation
- OB Bingo PDFDocument116 pagesOB Bingo PDFPatricia Ann CagampanPas encore d'évaluation
- Flamm CriteriaDocument1 pageFlamm CriteriaAgli AdhityaPas encore d'évaluation
- TetanusDocument3 pagesTetanusAgli AdhityaPas encore d'évaluation
- Beta HCG TestingDocument2 pagesBeta HCG TestingAgli AdhityaPas encore d'évaluation
- Reading ListDocument3 pagesReading ListAgli AdhityaPas encore d'évaluation
- Urinary Retention 2Document3 pagesUrinary Retention 2Agli AdhityaPas encore d'évaluation
- ArythmiaDocument42 pagesArythmiaAgli AdhityaPas encore d'évaluation
- Patomekanisme Case 1Document1 pagePatomekanisme Case 1Agli AdhityaPas encore d'évaluation
- PANSSDocument2 pagesPANSSAgli AdhityaPas encore d'évaluation
- Chorionic TumorsDocument12 pagesChorionic TumorsAgli AdhityaPas encore d'évaluation
- Medical Management Include Drug Therapy: Hydatidiform MoleDocument2 pagesMedical Management Include Drug Therapy: Hydatidiform MoleMaye ArugayPas encore d'évaluation
- Kompilasi - ICD MM Dan PM - Reference GuideDocument93 pagesKompilasi - ICD MM Dan PM - Reference GuidehijraPas encore d'évaluation
- HMOLEDocument34 pagesHMOLEZuellen Mae Garapan BedañoPas encore d'évaluation
- Hydatidiform MoleDocument15 pagesHydatidiform MoleRegine Mae Morales EncinadaPas encore d'évaluation
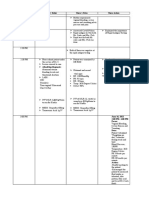
- Date and Time Doctor's Order Nurse's Notes Nurse Action: June 16, 2021 3:00 PM-4:00 PM FocusDocument6 pagesDate and Time Doctor's Order Nurse's Notes Nurse Action: June 16, 2021 3:00 PM-4:00 PM FocusAina De LeonPas encore d'évaluation
- Ectopic Molar Pregnancy A Case ReportDocument4 pagesEctopic Molar Pregnancy A Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- MCN Exam Gestational ConditionsDocument9 pagesMCN Exam Gestational ConditionsEdith Cabrera Cabigas - SabalboroPas encore d'évaluation
- Ultrasound in Obstetrics and Gynaecology: ReviewDocument9 pagesUltrasound in Obstetrics and Gynaecology: ReviewGustina Maryanti MooyPas encore d'évaluation
- OB Intern's Review - Dra LeeDocument214 pagesOB Intern's Review - Dra LeeKathleenZunigaPas encore d'évaluation
- Maternal and Child Health Nursing Practice Quiz #7Document24 pagesMaternal and Child Health Nursing Practice Quiz #7Ayeza DuaPas encore d'évaluation
- Hydatidiform Mole OutlineDocument3 pagesHydatidiform Mole Outlineyxly imperialPas encore d'évaluation
- PBL and NDXDocument15 pagesPBL and NDXJasmin AdoraPas encore d'évaluation
- 1 s2.0 S147264831500156X Main PDFDocument5 pages1 s2.0 S147264831500156X Main PDFMuhammad AzkaPas encore d'évaluation
- HmoleDocument30 pagesHmoleevaPas encore d'évaluation
- Maternal and Child Healthe Nursing MCQ 6Document18 pagesMaternal and Child Healthe Nursing MCQ 6shanika100% (1)
- Ob Pedia CDDocument13 pagesOb Pedia CDNom NomPas encore d'évaluation
- Cmca at RiskDocument11 pagesCmca at RiskAyanami PascuaPas encore d'évaluation
- What Malignancy Must Be Ruled Out in All Postmenopausal Women With Uterine BleedingDocument29 pagesWhat Malignancy Must Be Ruled Out in All Postmenopausal Women With Uterine Bleedingsmian08Pas encore d'évaluation
- NCK Past PapersDocument87 pagesNCK Past PapersjimwaoPas encore d'évaluation
- Obs 1 Bleeding in Early Pregnancy QuestionsDocument9 pagesObs 1 Bleeding in Early Pregnancy QuestionsSalmonella TyphiPas encore d'évaluation
- 1 Products of Conception - Libre PathologyDocument8 pages1 Products of Conception - Libre PathologyfadoPas encore d'évaluation
- Maternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test BankDocument20 pagesMaternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test BankKristinSummersmwyr100% (33)
- DR Khaled Final Exam MCQ 2012 - 2013Document89 pagesDR Khaled Final Exam MCQ 2012 - 2013ﻣﻠﻚ عيسى100% (2)
- 1 PBDocument5 pages1 PBaprajitaguptaPas encore d'évaluation
- Nucama 350Document17 pagesNucama 350BFKHOPas encore d'évaluation
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.Pas encore d'évaluation