Vous aimerez peut-être aussi
- 7 Day Diet AnalysisDocument5 pages7 Day Diet AnalysislipakevinPas encore d'évaluation
- NSCA Sports Nutrition 2008 PDFDocument20 pagesNSCA Sports Nutrition 2008 PDFSergio Mc DowellsPas encore d'évaluation
- The Neonatal Intensive Care Unit-2Document28 pagesThe Neonatal Intensive Care Unit-2api-457873289Pas encore d'évaluation
- Nutrilite Product HandbookDocument33 pagesNutrilite Product HandbookNikhil JainPas encore d'évaluation
- Nutrition in Etentulous PatientsDocument23 pagesNutrition in Etentulous PatientsKartik R. MorjariaPas encore d'évaluation
- Let's Celebrate National Brush Day! by SlidesgoDocument25 pagesLet's Celebrate National Brush Day! by SlidesgoALFEARA YUNIARPas encore d'évaluation
- Nutrition For Geriatric Complete Denture Wearing Patients 888Document20 pagesNutrition For Geriatric Complete Denture Wearing Patients 888Dhanu DhanushreePas encore d'évaluation
- International Journal of Health Sciences and Research: Caries Prevention: Vitamin Way - A Novel ApproachDocument5 pagesInternational Journal of Health Sciences and Research: Caries Prevention: Vitamin Way - A Novel Approachmaryam.saadPas encore d'évaluation
- Nutrition and Oral Health - (Review) : L. Leelavathi, Santa Thoudam and M. AnithaDocument5 pagesNutrition and Oral Health - (Review) : L. Leelavathi, Santa Thoudam and M. AnithaKhalisahatma BklPas encore d'évaluation
- Folic Acid and Periodontal Disease PDFDocument8 pagesFolic Acid and Periodontal Disease PDFAnonymous 8raPGW1tLPas encore d'évaluation
- 1nutrition and Oral Health 5th YearDocument11 pages1nutrition and Oral Health 5th Yeardr_masamaraPas encore d'évaluation
- P Muhammed Raheesh 1 Year PGDocument72 pagesP Muhammed Raheesh 1 Year PGneelima cPas encore d'évaluation
- محاضرة 9Document11 pagesمحاضرة 9mkomyu088Pas encore d'évaluation
- 120 Vitamin C Power Point Sophia Gomes Fe2 1Document17 pages120 Vitamin C Power Point Sophia Gomes Fe2 1api-720120569Pas encore d'évaluation
- Etiology of Dental CariesDocument35 pagesEtiology of Dental Cariesayshil mary sajiPas encore d'évaluation
- 8.diet, Nutrition, and Sugar SubstitutesDocument29 pages8.diet, Nutrition, and Sugar Substituteskhush sidhuPas encore d'évaluation
- By Dr. Smitha B K Post Graduate Student Department of Preventive and Community DentistryDocument58 pagesBy Dr. Smitha B K Post Graduate Student Department of Preventive and Community DentistryAnnupriya KhannaPas encore d'évaluation
- Nutritional Status and Its Effect On Dental HealthDocument5 pagesNutritional Status and Its Effect On Dental HealthMemex papPas encore d'évaluation
- 7 Oral Health of Geriatric People Modified Copy or ReferenceDocument15 pages7 Oral Health of Geriatric People Modified Copy or ReferenceNitya KrishnaPas encore d'évaluation
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيPas encore d'évaluation
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيPas encore d'évaluation
- Epidemiology of Periodontal DiseaseDocument24 pagesEpidemiology of Periodontal DiseaseAsad Khan5556Pas encore d'évaluation
- Nutritional Defi Ciencies: Vitamin DeficienciesDocument3 pagesNutritional Defi Ciencies: Vitamin DeficienciesdeenmPas encore d'évaluation
- 55 Diagnosis, Prevention and Management of Dental ErosionDocument29 pages55 Diagnosis, Prevention and Management of Dental Erosionraed ibrahimPas encore d'évaluation
- Ijpi 3 2 75 79Document5 pagesIjpi 3 2 75 79Rabiatul AdawiyahPas encore d'évaluation
- Ilovepdf MergedDocument7 pagesIlovepdf MergedNoval BalancePas encore d'évaluation
- Calcium-Vitamin D-Thyroid DisordersDocument4 pagesCalcium-Vitamin D-Thyroid DisorderssimranPas encore d'évaluation
- Atrophic GlossitisDocument7 pagesAtrophic Glossitisbima prabuPas encore d'évaluation
- Gerodontology BaruDocument53 pagesGerodontology BaruHappy Septianto S100% (1)
- Oral Manifestations of Nuritional Diseases in Children1Document5 pagesOral Manifestations of Nuritional Diseases in Children1andrada67Pas encore d'évaluation
- Francis Rossitano Case Objectives Days 4-5: Anatomy/Histology/Physiology (DBCS)Document7 pagesFrancis Rossitano Case Objectives Days 4-5: Anatomy/Histology/Physiology (DBCS)Phil BobPas encore d'évaluation
- Oral Medicine Journal Reading (Complete)Document29 pagesOral Medicine Journal Reading (Complete)Gabriel LowPas encore d'évaluation
- Biofilm Pertama Kali Dikenalkan Oleh Carlson Dan Criitenden Pada Tahun 1990 MeliputiDocument10 pagesBiofilm Pertama Kali Dikenalkan Oleh Carlson Dan Criitenden Pada Tahun 1990 MeliputiCindikya Saftiari DewiPas encore d'évaluation
- Diagnosis, Prevention and Management of Dental ErosionDocument29 pagesDiagnosis, Prevention and Management of Dental ErosionDr.Mandeep RallanPas encore d'évaluation
- Nutrition and Craniofacial Growth: P Muhammed Raheesh 1 Year PGDocument18 pagesNutrition and Craniofacial Growth: P Muhammed Raheesh 1 Year PGneelima cPas encore d'évaluation
- Geriatric Oral HealthDocument12 pagesGeriatric Oral HealthCeza CezaaPas encore d'évaluation
- Diet, Nutrition, and Prevention of Dental DiseaseDocument26 pagesDiet, Nutrition, and Prevention of Dental DiseaseMuhammad Benny SetiyadiPas encore d'évaluation
- 01 Metabolic Diseases CADocument47 pages01 Metabolic Diseases CAMi PatelPas encore d'évaluation
- Diet CounsellingDocument11 pagesDiet CounsellingDrBhawna AroraPas encore d'évaluation
- Fat Soluble Vitamin RevisedDocument80 pagesFat Soluble Vitamin RevisedsumitPas encore d'évaluation
- Causes of Periodontal Disease: BiofilmDocument3 pagesCauses of Periodontal Disease: BiofilmCristinaPas encore d'évaluation
- Orh Fact SheetDocument2 pagesOrh Fact SheetAliantz MosesPas encore d'évaluation
- Oral Deasease and Dental HealthDocument2 pagesOral Deasease and Dental HealthAgam KgPas encore d'évaluation
- Vitamin C Research PaperDocument6 pagesVitamin C Research Paperapi-720120569Pas encore d'évaluation
- DR Prakash Mungli Vitamin Questions With Short Case Stems Along With PicturesDocument12 pagesDR Prakash Mungli Vitamin Questions With Short Case Stems Along With PicturesomarPas encore d'évaluation
- Ncbi Ascorbic AcidDocument7 pagesNcbi Ascorbic AcidOsunlola GabrielPas encore d'évaluation
- Topic 161: Changes in The Mucous Membrane of Oral Cavity in Hypovitaminosis and Avitaminosis A, C. Tactics of Dentists. Questions For Control of KnowledgeDocument9 pagesTopic 161: Changes in The Mucous Membrane of Oral Cavity in Hypovitaminosis and Avitaminosis A, C. Tactics of Dentists. Questions For Control of KnowledgeAbdullah SaleemPas encore d'évaluation
- POMDocument3 pagesPOMYzsa Geal InalPas encore d'évaluation
- Nutrition and Oral HealthDocument71 pagesNutrition and Oral HealthVinay PanchalPas encore d'évaluation
- ScccvyDocument7 pagesScccvyDavy JonesPas encore d'évaluation
- Scurvy in Pediatric Age Group E A Disease Often Forgotten?: SciencedirectDocument7 pagesScurvy in Pediatric Age Group E A Disease Often Forgotten?: SciencedirectDavy JonesPas encore d'évaluation
- Manifestasi Oral Nutritional Disorders (Journal)Document12 pagesManifestasi Oral Nutritional Disorders (Journal)yolasrikandiPas encore d'évaluation
- 2012 33 339 Bryon Lauer and Nancy Spector: Pediatrics in ReviewDocument16 pages2012 33 339 Bryon Lauer and Nancy Spector: Pediatrics in ReviewFernanda SierraPas encore d'évaluation
- Jurnal InternasionalDocument8 pagesJurnal InternasionalBrivita PopyPas encore d'évaluation
- Prevention of Periodontal Disease HandoutDocument13 pagesPrevention of Periodontal Disease HandoutShady AnwarPas encore d'évaluation
- Preven Lec27Document6 pagesPreven Lec27Sura Abdel JabbarPas encore d'évaluation
- Final Editing AssignmentDocument5 pagesFinal Editing Assignmentbarsha subediPas encore d'évaluation
- Kwashiorkor: Signs and SymptomsDocument5 pagesKwashiorkor: Signs and SymptomsJohn MaynardPas encore d'évaluation
- Prevention of Dental CariesDocument6 pagesPrevention of Dental CariesRadhwan Hameed AsadPas encore d'évaluation
- Molecules: Development and Characterization of An Orodispersible Film For Vitamin D3 SupplementationDocument14 pagesMolecules: Development and Characterization of An Orodispersible Film For Vitamin D3 Supplementationheristiana pratiwiPas encore d'évaluation
- How To Prevent And Reverse Tooth Decay In ChildrenD'EverandHow To Prevent And Reverse Tooth Decay In ChildrenPas encore d'évaluation
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsD'EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsPas encore d'évaluation
- Alert Protein DrinksDocument4 pagesAlert Protein DrinksnospamokPas encore d'évaluation
- Intervention Module - For NutritionDocument13 pagesIntervention Module - For NutritionRadhaKrishna BallaPas encore d'évaluation
- Amway Products and BrandsDocument8 pagesAmway Products and BrandsSundar Shanmuga100% (1)
- Dave DetoxDocument2 pagesDave DetoxIulian Mihai100% (1)
- Soluvit N CMIDocument2 pagesSoluvit N CMIIka KusumaPas encore d'évaluation
- Case StudyDocument33 pagesCase StudySarah GatuzPas encore d'évaluation
- Spirulina Cultivation General InformationDocument94 pagesSpirulina Cultivation General InformationGanesh SelvarajPas encore d'évaluation
- Biology F3 Supp Exercise - AnswersDocument2 pagesBiology F3 Supp Exercise - AnswersJacky Choi0% (1)
- Production of Solanum Lycopersicum (Tomato) Extract As VinegarDocument28 pagesProduction of Solanum Lycopersicum (Tomato) Extract As VinegarAngel100% (1)
- SeleniumDocument16 pagesSeleniumAmalia RizkyPas encore d'évaluation
- Ingestion of Wheat Protein Increases in Vivo Muscle Protein Synthesis Rates in Healthy Older Men in A Randomized TrialDocument16 pagesIngestion of Wheat Protein Increases in Vivo Muscle Protein Synthesis Rates in Healthy Older Men in A Randomized TrialliaPas encore d'évaluation
- THE STARCH SOLUTION: The Low Fat Whole Foods Plant Based DietDocument2 pagesTHE STARCH SOLUTION: The Low Fat Whole Foods Plant Based DietSalman khanPas encore d'évaluation
- Full Hand Feeding of Sheep QuantitiesDocument8 pagesFull Hand Feeding of Sheep QuantitiesfrankyPas encore d'évaluation
- Flavored Milk - A Brief ResearchDocument12 pagesFlavored Milk - A Brief ResearchKaren NoronhaPas encore d'évaluation
- Health Malnut. and Micronut. DLPDocument3 pagesHealth Malnut. and Micronut. DLPMary Ann PaladPas encore d'évaluation
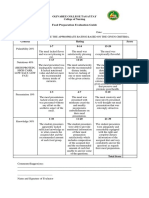
- Food Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingDocument2 pagesFood Preparation Evaluation Guide: Olivarez College Tagaytay College of NursingRaquel M. MendozaPas encore d'évaluation
- Associate Price ListDocument2 pagesAssociate Price ListRustom RemorozaPas encore d'évaluation
- 5 - Aratiles-WHOLE PAPER PDFDocument22 pages5 - Aratiles-WHOLE PAPER PDFCindy MarquezPas encore d'évaluation
- Case Study 11Document28 pagesCase Study 11api-301883277Pas encore d'évaluation
- Impact of Different Treatments On Vitamin - C Content of AmlaDocument2 pagesImpact of Different Treatments On Vitamin - C Content of AmlaProfessor.Krishan Bir SinghPas encore d'évaluation
- 8a Food Digestion Science QuizDocument42 pages8a Food Digestion Science QuizahmerjamilPas encore d'évaluation
- Latihan SoalDocument8 pagesLatihan SoalNisaun Najwa ShalihahPas encore d'évaluation
- Moringa BookDocument9 pagesMoringa BookRodney McCrary GrayPas encore d'évaluation
- SALUYOT1Document38 pagesSALUYOT1rosemarie nachorPas encore d'évaluation
- Ben Greenfield Fitness Daily Routines PDFDocument29 pagesBen Greenfield Fitness Daily Routines PDFAlan80% (10)
- Puso NG Saging EmbutidoDocument4 pagesPuso NG Saging EmbutidoRiel Sevilla100% (1)