Vous aimerez peut-être aussi
- Lecture 17 - Aging & DiseaseDocument22 pagesLecture 17 - Aging & DiseaseNat FochaPas encore d'évaluation
- P Q S F Q P S F A F: Before Selection Correction For Selection After SelectionDocument1 pageP Q S F Q P S F A F: Before Selection Correction For Selection After SelectionNat FochaPas encore d'évaluation
- Neuroscientist Seeking Career Opportunity at Otsuka America PharmaceuticalDocument1 pageNeuroscientist Seeking Career Opportunity at Otsuka America PharmaceuticalNat FochaPas encore d'évaluation
- Bio112A Sample Lecture Exam S13 With AnswersDocument2 pagesBio112A Sample Lecture Exam S13 With AnswersNat FochaPas encore d'évaluation
- Week 6 HWDocument1 pageWeek 6 HWNat FochaPas encore d'évaluation
- Belluzzi Et Al - Age-Dependent Effects of Nicotine, Locomotor Activity & CPP in RatsDocument7 pagesBelluzzi Et Al - Age-Dependent Effects of Nicotine, Locomotor Activity & CPP in RatsNat FochaPas encore d'évaluation
- PSYCH 118 AGGRESSION NOTES ON PROXIMATE MECHANISMS AND MODELSDocument30 pagesPSYCH 118 AGGRESSION NOTES ON PROXIMATE MECHANISMS AND MODELSNat FochaPas encore d'évaluation
- PSYCH 118 May 30, 2013Document26 pagesPSYCH 118 May 30, 2013Nat FochaPas encore d'évaluation
- Ucla Campus MapDocument2 pagesUcla Campus MapNat FochaPas encore d'évaluation
- MDMA (Ecstasy) - Final PresentationDocument12 pagesMDMA (Ecstasy) - Final PresentationNat Focha100% (1)
- Lecture 8 - Mating SystemsDocument35 pagesLecture 8 - Mating SystemsNat FochaPas encore d'évaluation
- Neurological Diseases - Clinical Correlation 2Document1 pageNeurological Diseases - Clinical Correlation 2Nat FochaPas encore d'évaluation
- Lecture 12 - Antipredator BehaviorDocument34 pagesLecture 12 - Antipredator BehaviorNat FochaPas encore d'évaluation
- Changeux Et Al - Nicotine Receptors & Addiction, Genetically Modified MiceDocument13 pagesChangeux Et Al - Nicotine Receptors & Addiction, Genetically Modified MiceNat FochaPas encore d'évaluation
- Lecture 8 - Mating SystemsDocument35 pagesLecture 8 - Mating SystemsNat FochaPas encore d'évaluation
- Chronic Pain AddictionDocument23 pagesChronic Pain AddictionNat FochaPas encore d'évaluation
- Ucla Campus MapDocument2 pagesUcla Campus MapNat FochaPas encore d'évaluation
- Neurobiology of Social Bonding - Seminar Summary ParagraphDocument1 pageNeurobiology of Social Bonding - Seminar Summary ParagraphNat FochaPas encore d'évaluation
- Aicardi Syndrome - Clinical Correlation 1Document1 pageAicardi Syndrome - Clinical Correlation 1Nat FochaPas encore d'évaluation
- The Veg FruitDocument2 pagesThe Veg FruitNat FochaPas encore d'évaluation
- Week 5 HWDocument1 pageWeek 5 HWNat FochaPas encore d'évaluation
- Psych 137C Midterm Paper - 021413Document2 pagesPsych 137C Midterm Paper - 021413Nat FochaPas encore d'évaluation
- Love Is in The NeurochemicalsDocument1 pageLove Is in The NeurochemicalsNat FochaPas encore d'évaluation
- Event - Female Competition and Dispersal PatternsDocument1 pageEvent - Female Competition and Dispersal PatternsNat FochaPas encore d'évaluation
- Study Worksheet 2Document7 pagesStudy Worksheet 2Nat FochaPas encore d'évaluation
- Belluzzi Et Al - Age-Dependent Effects of Nicotine, Locomotor Activity & CPP in RatsDocument7 pagesBelluzzi Et Al - Age-Dependent Effects of Nicotine, Locomotor Activity & CPP in RatsNat FochaPas encore d'évaluation
- P Q S F Q P S F A F: Before Selection Correction For Selection After SelectionDocument1 pageP Q S F Q P S F A F: Before Selection Correction For Selection After SelectionNat FochaPas encore d'évaluation
- P Q S F Q P S F A F: Before Selection Correction For Selection After SelectionDocument1 pageP Q S F Q P S F A F: Before Selection Correction For Selection After SelectionNat FochaPas encore d'évaluation
- Week 4 HWDocument1 pageWeek 4 HWNat FochaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- T Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentDocument6 pagesT Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentCurcubet OlgaPas encore d'évaluation
- Treatment of Optic NeuritisDocument4 pagesTreatment of Optic NeuritisGufront MustofaPas encore d'évaluation
- 9 Basic Areas of Marriage According To Worthington Jr.Document2 pages9 Basic Areas of Marriage According To Worthington Jr.Lynda A BarnesPas encore d'évaluation
- Understanding Motivation Chapter13Document24 pagesUnderstanding Motivation Chapter13anon-318198Pas encore d'évaluation
- Hydralazine Drug StudyDocument1 pageHydralazine Drug Studymilkv71% (7)
- EFT Tapping Points Chart Explains Emotional Links to Each PointDocument9 pagesEFT Tapping Points Chart Explains Emotional Links to Each PointJodi Johnson100% (2)
- Actinic Cheratosis - A ReviewDocument4 pagesActinic Cheratosis - A ReviewMARIUS-MIRCEA POPESCU-MICLOSANUPas encore d'évaluation
- Traumatic Brain Injury and Cerebral ResuscitationDocument56 pagesTraumatic Brain Injury and Cerebral ResuscitationsyahirPas encore d'évaluation
- Osma y Barlow 2021 PU en SpainDocument15 pagesOsma y Barlow 2021 PU en Spaingerard sansPas encore d'évaluation
- Program Ro-Inmed 2019Document26 pagesProgram Ro-Inmed 2019Adriana FranciscaPas encore d'évaluation
- Journal Bedah Thorax 2Document15 pagesJournal Bedah Thorax 2Novia LarasatiPas encore d'évaluation
- 4.4 Antibiotics IV To Oral Switch Guidelines For Pharmacists Southern HealthDocument5 pages4.4 Antibiotics IV To Oral Switch Guidelines For Pharmacists Southern HealthditaokkyPas encore d'évaluation
- AcetaminophenDocument2 pagesAcetaminophendrugcardref100% (1)
- Occupational Health and SafetyDocument33 pagesOccupational Health and Safetyrajirajesh100% (2)
- Nurse Writing 002 OET Practice Letter by PASS OETDocument3 pagesNurse Writing 002 OET Practice Letter by PASS OETafacean74% (27)
- Pharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CDocument30 pagesPharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CRam NareshPas encore d'évaluation
- History of Counseling Profession DevelopmentDocument8 pagesHistory of Counseling Profession DevelopmentPro Vince SyanoPas encore d'évaluation
- 5 of The Best Essential Oils For HairDocument13 pages5 of The Best Essential Oils For HairJyoti ShindePas encore d'évaluation
- The Gerson Therapy For Those Dying of CancerDocument80 pagesThe Gerson Therapy For Those Dying of CancerElton Luz100% (1)
- Dr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFDocument7 pagesDr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFZACHARIAH MANKIRPas encore d'évaluation
- Blood CollectionDocument25 pagesBlood Collectionطاهرة حربية AlcaldePas encore d'évaluation
- A Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsDocument4 pagesA Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsOrtho OrganizersPas encore d'évaluation
- Modulo 200Document2 pagesModulo 200suso73Pas encore d'évaluation
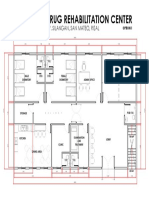
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonPas encore d'évaluation
- COPD, Asthma, and Lung Disease Nursing Assessment QuestionsDocument8 pagesCOPD, Asthma, and Lung Disease Nursing Assessment QuestionsMichael Boado100% (3)
- Psychological First Aid-A Training GuideDocument8 pagesPsychological First Aid-A Training Guidejprewittdiaz100% (1)
- CKD CHCRTDocument28 pagesCKD CHCRTNurhidayati KeriyunPas encore d'évaluation
- Bobath and NeuroDevelopmental Therapy What Is The FutureDocument1 pageBobath and NeuroDevelopmental Therapy What Is The FutureFuncionalidad DiversaPas encore d'évaluation
- Ecmo Basic ConceptsDocument37 pagesEcmo Basic Conceptskhoniker bondhuPas encore d'évaluation
- Thalassemia: BY: Deddy Ramadhan G2A016098Document11 pagesThalassemia: BY: Deddy Ramadhan G2A016098deddy ramadhanPas encore d'évaluation