Vous aimerez peut-être aussi
- RCFT ManualDocument131 pagesRCFT ManualFernanda Gallo100% (20)
- Revised Comprehensive Norms For An Expanded Halstead-Reitan Battery PDFDocument645 pagesRevised Comprehensive Norms For An Expanded Halstead-Reitan Battery PDFnihao_ching100% (7)
- WCST Manual PDFDocument234 pagesWCST Manual PDFKarina Hechenleitner100% (4)
- Manual CCTT I y II PDFDocument77 pagesManual CCTT I y II PDFJosé LuccaPas encore d'évaluation
- Tower of London ManualDocument100 pagesTower of London ManualLucyRainPas encore d'évaluation
- Trail Making TestDocument5 pagesTrail Making TestRahmah Fitri Utami71% (7)
- Scoring Rey Complex Figure Test and Recognition TrialDocument11 pagesScoring Rey Complex Figure Test and Recognition TrialAnonymous mIBVSE100% (4)
- Boston Naming Test: Harold Goodglass and Edith KaplanDocument61 pagesBoston Naming Test: Harold Goodglass and Edith Kaplancaroline100% (1)
- Stroop Color and Word TestDocument3 pagesStroop Color and Word TestVíctor MJ0% (1)
- Trail Making Test Manual PDFDocument37 pagesTrail Making Test Manual PDFubunturider50% (2)
- Halstead Reitan BatteryDocument8 pagesHalstead Reitan Batteryren1322100% (3)
- Adult Norms For The Rey-Osterrieth Complex Figure ExtendedDocument19 pagesAdult Norms For The Rey-Osterrieth Complex Figure ExtendedIcaro100% (1)
- Hooper Visual Organization Test PsychometricDocument10 pagesHooper Visual Organization Test PsychometricJosiane AlmeidaPas encore d'évaluation
- FBI (Frontal Behabioral InventoryDocument2 pagesFBI (Frontal Behabioral InventoryBegoña Martinez100% (1)
- BVMTDocument5 pagesBVMTyadiiiiii0% (1)
- Children With ProblemsDocument97 pagesChildren With ProblemsbobbysingersyahooPas encore d'évaluation
- Nursing Performance Appraisal ExamplesDocument6 pagesNursing Performance Appraisal ExamplesSophia Kara50% (6)
- The Hopkins Verbal Learning TestDocument7 pagesThe Hopkins Verbal Learning TestRocío G Izq50% (4)
- RBANSDocument10 pagesRBANSFanel PutraPas encore d'évaluation
- Normative Symbol Digit Modalities Test..Document7 pagesNormative Symbol Digit Modalities Test..baobhPas encore d'évaluation
- Wms-Iv Presentation PDFDocument32 pagesWms-Iv Presentation PDFraghu kumaarPas encore d'évaluation
- Ravlt 2010 PDFDocument7 pagesRavlt 2010 PDFPriscila KleinPas encore d'évaluation
- WISC-IV Subtest DescriptionsDocument2 pagesWISC-IV Subtest DescriptionsPUÑOYLETRAPas encore d'évaluation
- Benton VRTDocument134 pagesBenton VRTRadu Andrei100% (34)
- Trail Making TestDocument4 pagesTrail Making TestElizabeth Gajardo BustosPas encore d'évaluation
- Clinical Interpretation of the WAIS-III and WMS-IIID'EverandClinical Interpretation of the WAIS-III and WMS-IIIÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- PQ Procedure Focusing QDocument6 pagesPQ Procedure Focusing Qagnes windram100% (1)
- 10 Mental Health Tips For Teachers During The COVIDDocument4 pages10 Mental Health Tips For Teachers During The COVIDBey Bi NingPas encore d'évaluation
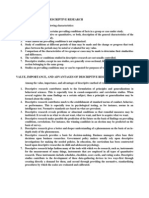
- Characteristics of Descriptive ResearchDocument1 pageCharacteristics of Descriptive ResearchJohn Mark Manganip Edades93% (15)
- Norms For The Visual Object and Space Perception Battery-AbbreviatedDocument16 pagesNorms For The Visual Object and Space Perception Battery-Abbreviatedlaura4dap100% (1)
- Benton Judgment of Line Orientation PDFDocument16 pagesBenton Judgment of Line Orientation PDFIrina DespaPas encore d'évaluation
- Finger Tapping Test AveragesDocument10 pagesFinger Tapping Test AveragesLuis ReyesPas encore d'évaluation
- Detection of Malingering during Head Injury LitigationD'EverandDetection of Malingering during Head Injury LitigationArthur MacNeill Horton, Jr.Pas encore d'évaluation
- Norms For The Stroop Color-Word Interference Test and The TowerDocument17 pagesNorms For The Stroop Color-Word Interference Test and The Towerlaura4dapPas encore d'évaluation
- BVRT PDFDocument8 pagesBVRT PDFAleena Zaidi100% (1)
- Norms For The Rey-Osterrieth Complex FigureDocument23 pagesNorms For The Rey-Osterrieth Complex Figurelaura4dap100% (2)
- D-KEFS Validity - An Update (Pearson Clinical UK, 2008)Document9 pagesD-KEFS Validity - An Update (Pearson Clinical UK, 2008)Anonymous tFZP10dVRUPas encore d'évaluation
- Dementia and Effort Test PerformanceDocument21 pagesDementia and Effort Test PerformanceIcaroPas encore d'évaluation
- HVLTDocument19 pagesHVLTVicente Cáceres100% (3)
- Trail MakingDocument6 pagesTrail MakingYolanda Carreño100% (1)
- Trail Making Test A and B Normative DataDocument12 pagesTrail Making Test A and B Normative DataVivi Patarroyo MPas encore d'évaluation
- M WCSTDocument7 pagesM WCSTMarcela Pretto100% (1)
- WMS IvDocument12 pagesWMS IvAnaaaerobiosPas encore d'évaluation
- MOANS - Trail-Making Test, Stroop, and COWATDocument50 pagesMOANS - Trail-Making Test, Stroop, and COWATGeorge BialkowskiPas encore d'évaluation
- Estimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciaDocument14 pagesEstimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciathebeholderPas encore d'évaluation
- WMS IvDocument12 pagesWMS IvAnaaaerobios100% (1)
- Fas InglesDocument54 pagesFas Inglescgalain100% (1)
- Color Trail TestDocument13 pagesColor Trail Testallexa726083100% (4)
- Norm TMT PDFDocument12 pagesNorm TMT PDFGustavoPas encore d'évaluation
- WAIS in Traumatic Brain Injury Wais CercDocument14 pagesWAIS in Traumatic Brain Injury Wais CercBeeHoofPas encore d'évaluation
- Trail Making Test (TMT) : (Prikaz Instrumenta)Document6 pagesTrail Making Test (TMT) : (Prikaz Instrumenta)lidijaperovic880% (1)
- Understanding Design Uency: Motor and Executive ContributionsDocument13 pagesUnderstanding Design Uency: Motor and Executive ContributionsTurfa AhmedPas encore d'évaluation
- Interference Score Stroop Test-MainDocument13 pagesInterference Score Stroop Test-MainNur Indah FebriyantiPas encore d'évaluation
- Wisconsin Card Sorting TestDocument2 pagesWisconsin Card Sorting TestzeljkamandicPas encore d'évaluation
- Trail Making TestDocument12 pagesTrail Making TestSónia Mendes100% (1)
- PASAT Manual PDFDocument8 pagesPASAT Manual PDFFélix ÁguilaPas encore d'évaluation
- BRIEF2 Self PiC Interpretive Sample ReportDocument45 pagesBRIEF2 Self PiC Interpretive Sample ReportirinaPas encore d'évaluation
- Children's Color TrailsDocument14 pagesChildren's Color TrailsLuis Venegas B100% (1)
- NBSE Evidence-Based Review Test Summary TablesDocument82 pagesNBSE Evidence-Based Review Test Summary TablesIcaroPas encore d'évaluation
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)jovicacona5598Pas encore d'évaluation
- Case Report Original Article: Utilization Pa! Ern of Psychiatric Consultation ServicesDocument7 pagesCase Report Original Article: Utilization Pa! Ern of Psychiatric Consultation ServicesbobbysingersyahooPas encore d'évaluation
- CNSP FileDocument3 pagesCNSP FilebobbysingersyahooPas encore d'évaluation
- DSWDDocument61 pagesDSWDGorby Resuello89% (9)
- Special Laws On Children - 8353 9262 9231 7877 7610 920-130608212650Document95 pagesSpecial Laws On Children - 8353 9262 9231 7877 7610 920-130608212650bobbysingersyahooPas encore d'évaluation
- Glossary of Important Terms For Evaluation and Assessment As A Precursor To Solicitation of GrantsDocument8 pagesGlossary of Important Terms For Evaluation and Assessment As A Precursor To Solicitation of GrantsbobbysingersyahooPas encore d'évaluation
- CSC Form 41 - Medical CertifcateDocument1 pageCSC Form 41 - Medical CertifcateRizal LeonardoPas encore d'évaluation
- Investigation Formats2Document45 pagesInvestigation Formats2Lhine Kiwalan100% (1)
- TODA JR vs. Court of Appeals DigestDocument2 pagesTODA JR vs. Court of Appeals Digestproject_zi50% (2)
- What Is Night Shift Differential PayDocument14 pagesWhat Is Night Shift Differential PaybobbysingersyahooPas encore d'évaluation
- Mens Rea Table - NewDocument4 pagesMens Rea Table - NewbobbysingersyahooPas encore d'évaluation
- 111 The Law ChicDocument14 pages111 The Law ChicbobbysingersyahooPas encore d'évaluation
- Bill of Rights - Section6-12Document23 pagesBill of Rights - Section6-12sydfrey75% (4)
- Exponential EquationDocument77 pagesExponential EquationbobbysingersyahooPas encore d'évaluation
- Cases On Wills and SuccessionDocument4 pagesCases On Wills and SuccessionDeb BagaporoPas encore d'évaluation
- Firo - B: Will SchutzDocument10 pagesFiro - B: Will SchutzAshokPas encore d'évaluation
- Counselor S Check List of Rights and ResponsibilitiesDocument3 pagesCounselor S Check List of Rights and ResponsibilitiesbobbysingersyahooPas encore d'évaluation
- JC2013-1 AnnexbDocument20 pagesJC2013-1 AnnexbJeremiah TrinidadPas encore d'évaluation
- JC2013-1 Annex A.1Document1 pageJC2013-1 Annex A.1bobbysingersyahooPas encore d'évaluation
- The Attorney General's Guidelines For Domestic Fbi OperationsDocument46 pagesThe Attorney General's Guidelines For Domestic Fbi Operationsmary engPas encore d'évaluation
- Children's Personality QuestionnaireDocument138 pagesChildren's Personality QuestionnairebobbysingersyahooPas encore d'évaluation
- Firo-B PowrpointDocument34 pagesFiro-B PowrpointbobbysingersyahooPas encore d'évaluation
- FIRODocument4 pagesFIROsheerinfathimaPas encore d'évaluation
- AphasiaDocument2 pagesAphasiaVanessa AntoinePas encore d'évaluation
- Important Decisions Thirty Year Cut OffDocument45 pagesImportant Decisions Thirty Year Cut OffbobbysingersyahooPas encore d'évaluation
- FIRODocument1 pageFIROTamanna SarkarPas encore d'évaluation
- Lions Digests IIDocument16 pagesLions Digests IIbobbysingersyahooPas encore d'évaluation
- Mens Rea Table PDFDocument2 pagesMens Rea Table PDFbobbysingersyahooPas encore d'évaluation
- Feb 28proceedings Notes FinalDocument102 pagesFeb 28proceedings Notes FinalbobbysingersyahooPas encore d'évaluation
- Psychometric Tests For Recuitment and Selection ProjectDocument75 pagesPsychometric Tests For Recuitment and Selection Projectbobbysingersyahoo100% (1)
- SubjectivismDocument8 pagesSubjectivismBack upPas encore d'évaluation
- Psychology & Criminal BehaviorDocument4 pagesPsychology & Criminal Behaviorelisha oketchPas encore d'évaluation
- COMFORT From The Koran Translated by N.J. DawoodDocument20 pagesCOMFORT From The Koran Translated by N.J. DawoodChrisneliane Macahilas100% (2)
- Project 2 SociologyDocument11 pagesProject 2 SociologyDavid DuongPas encore d'évaluation
- MGBBTOOSE: Orientation For Success in Higher Education in Business and Tourism ManagementDocument6 pagesMGBBTOOSE: Orientation For Success in Higher Education in Business and Tourism Managementmadam iqraPas encore d'évaluation
- Lesson Plan 2Document4 pagesLesson Plan 2api-253371909Pas encore d'évaluation
- Diagnostic ResearchDocument6 pagesDiagnostic ResearchKyle Collene Macaloyos BardajePas encore d'évaluation
- History and Evolution of Dynamic Psychiatry: A Timeless ClassicDocument11 pagesHistory and Evolution of Dynamic Psychiatry: A Timeless ClassicCatalin TudoriuPas encore d'évaluation
- OpenStax Psychology2e LN01Document5 pagesOpenStax Psychology2e LN01Shehib GulaimidPas encore d'évaluation
- Acceptance Vs Forgiveness 1-3 FromDocument3 pagesAcceptance Vs Forgiveness 1-3 Fromdiya gautamPas encore d'évaluation
- Bipolar - Related Disorders and Its Etiology 1 25092023 124646pmDocument38 pagesBipolar - Related Disorders and Its Etiology 1 25092023 124646pmashraffatima875Pas encore d'évaluation
- Argumentative EssayDocument2 pagesArgumentative EssayKarolGamingPas encore d'évaluation
- PsychologyDocument6 pagesPsychologyJerlyn Marie MelicadoPas encore d'évaluation
- Data CollectionDocument28 pagesData CollectionJohn Jordan Calebag100% (5)
- Keywords:-Internet, Social Networking, PsychologicalDocument8 pagesKeywords:-Internet, Social Networking, PsychologicalInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Michael Rees ResumeDocument1 pageMichael Rees Resumeapi-438184228Pas encore d'évaluation
- Dbda Introductiondoc PDF FreeDocument5 pagesDbda Introductiondoc PDF FreeJomyJosePas encore d'évaluation
- Sample Test Questions Special EducationDocument5 pagesSample Test Questions Special EducationRobert Samonte100% (1)
- Test Anxiety Causes University Students To Underperform in Their ExaminationsDocument3 pagesTest Anxiety Causes University Students To Underperform in Their ExaminationsnurfarahPas encore d'évaluation
- Detailed Lesson Plan in Humanities and Social ScienceDocument4 pagesDetailed Lesson Plan in Humanities and Social ScienceIrish LorestoPas encore d'évaluation
- Assignment 1Document2 pagesAssignment 1Ayessa GomezPas encore d'évaluation
- CBFS-Module 5 - Performance Appraisals, FeedbackDocument6 pagesCBFS-Module 5 - Performance Appraisals, FeedbackIrish Claire BaquiranPas encore d'évaluation
- Business Ethics Note 2Document18 pagesBusiness Ethics Note 2Jebin JamesPas encore d'évaluation
- Work Review and FeedbackDocument28 pagesWork Review and FeedbackKoral VermaPas encore d'évaluation
- DR KizlikDocument5 pagesDR KizlikAli Yahya100% (1)
- CRCJ1000B W13 Syllabus VFDocument6 pagesCRCJ1000B W13 Syllabus VFJose Li ToPas encore d'évaluation