Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Benefits of Online EducationDocument26 pagesBenefits of Online EducationJebjeb C. BrañaPas encore d'évaluation
- Introduction To Financial Statement AuditDocument49 pagesIntroduction To Financial Statement Auditgandara koPas encore d'évaluation
- Implementation of Lead Time Reduction in Merchandising Department Using Lean TechniquesDocument10 pagesImplementation of Lead Time Reduction in Merchandising Department Using Lean Techniquessonia joseph100% (1)
- Thesis Data Analysis and InterpretationDocument8 pagesThesis Data Analysis and Interpretationafcnfajtd100% (2)
- Combining Variation Simulation With Welding Simulation For Prediction of Deformation and Variation of A Final AssemblyDocument6 pagesCombining Variation Simulation With Welding Simulation For Prediction of Deformation and Variation of A Final AssemblySaturnus PlutoPas encore d'évaluation
- Organizational Behaviour-SandhyaDocument42 pagesOrganizational Behaviour-SandhyaAshish Gupta0% (1)
- Historical Context of The Emergence of Each DisciplinesDocument43 pagesHistorical Context of The Emergence of Each DisciplinesBloodmier GabrielPas encore d'évaluation
- Advanced Course InCoRP19 ContentsDocument3 pagesAdvanced Course InCoRP19 ContentsSri NPas encore d'évaluation
- Millat Tractor: Auto Mobile Agriculture IndustryDocument27 pagesMillat Tractor: Auto Mobile Agriculture IndustryZaman RanaPas encore d'évaluation
- Child SocialLeadershipQualitiesDocument25 pagesChild SocialLeadershipQualitiesVincent FordPas encore d'évaluation
- 5 CO03 Week 2 Slidesv 2Document37 pages5 CO03 Week 2 Slidesv 2fedaPas encore d'évaluation
- Resource H Approaching The Literature Review PowerpointDocument16 pagesResource H Approaching The Literature Review PowerpointAnonymous XTL7o0tGo9Pas encore d'évaluation
- Understanding The Quality of Life of SeniorsDocument27 pagesUnderstanding The Quality of Life of SeniorsYen NgoPas encore d'évaluation
- Ryan Sudhakaran PposterDocument1 pageRyan Sudhakaran PposterAkihisa YoshiiPas encore d'évaluation
- Artikel Cukilan Contoh ICoTE-1 2017Document6 pagesArtikel Cukilan Contoh ICoTE-1 2017dwitaPas encore d'évaluation
- Production and Active Pharmaceutical Ingredients 5EEC Group 1Document10 pagesProduction and Active Pharmaceutical Ingredients 5EEC Group 1Derrick RamosPas encore d'évaluation
- Innovation Implementation: The Challenge ofDocument27 pagesInnovation Implementation: The Challenge ofMalik Atif ZamanPas encore d'évaluation
- Presentation StrategyDocument40 pagesPresentation StrategyAbdullah ghauriPas encore d'évaluation
- CIK - msl.00166 ReportDocument3 pagesCIK - msl.00166 ReportChristopher Edward Martin FlanaganPas encore d'évaluation
- Assess 2 Module 1Document25 pagesAssess 2 Module 1jezreel arancesPas encore d'évaluation
- MILMAaa InternshipDocument85 pagesMILMAaa InternshipMelvin BabuPas encore d'évaluation
- District Orientation On The Utilization of The Enhanced Teacher Induction Program (Tip) Course Books Learning Action PlanDocument3 pagesDistrict Orientation On The Utilization of The Enhanced Teacher Induction Program (Tip) Course Books Learning Action PlanGabriel Tingson GalleposoPas encore d'évaluation
- Reflections and AnalysisDocument4 pagesReflections and AnalysisAlvin Fruelda FaaPas encore d'évaluation
- The Pfizer Guide To Careers in PharmacyDocument171 pagesThe Pfizer Guide To Careers in Pharmacyakberk8318Pas encore d'évaluation
- Analysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationDocument4 pagesAnalysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationMahavir GemavatPas encore d'évaluation
- Ken Black QA All Odd No Chapter SolutionDocument919 pagesKen Black QA All Odd No Chapter SolutionRushabh Vora83% (6)
- Match Running Performance in UEFA Champions League: Do More Successful Teams Really Run Less?Document5 pagesMatch Running Performance in UEFA Champions League: Do More Successful Teams Really Run Less?Tomislav PranjićPas encore d'évaluation
- All Aboard: Moving Forward Responsibly Online..Document80 pagesAll Aboard: Moving Forward Responsibly Online..Abhijeet PandeyPas encore d'évaluation
- Bender Clincal Nurse ManagerDocument10 pagesBender Clincal Nurse ManagerfairwoodsPas encore d'évaluation
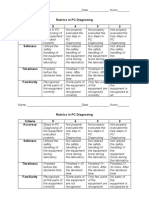
- Rubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - ScoreDocument2 pagesRubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - Scorejhun ecleoPas encore d'évaluation