Vous aimerez peut-être aussi
- How To Outlive An EMP The Early Pioneer WayDocument66 pagesHow To Outlive An EMP The Early Pioneer WayRod Langley86% (7)
- Dengue Case Presentation Pedia (PCMC)Document59 pagesDengue Case Presentation Pedia (PCMC)Michael Valderrama100% (4)
- Case Study (Diabetes Mellitus)Document24 pagesCase Study (Diabetes Mellitus)Sweetie Star88% (33)
- A Case Study Of: Pulmonary TubercolusisDocument39 pagesA Case Study Of: Pulmonary TubercolusisMASII86% (7)
- Dengue Fever Case StudyDocument24 pagesDengue Fever Case Studymaemaeyee95% (22)
- Dengue Fever Syndrome Case StudyDocument16 pagesDengue Fever Syndrome Case Studylilzette22100% (3)
- Dengue Case StudyDocument20 pagesDengue Case Studyjohn jumborockPas encore d'évaluation
- Case StudyDocument45 pagesCase Studymejul100% (2)
- Case Study On Typhoid FeverDocument33 pagesCase Study On Typhoid Feverjarelle bondoc93% (14)
- Case StudyDocument14 pagesCase StudyJulia NeriPas encore d'évaluation
- Case Study Neonatal SepsisDocument24 pagesCase Study Neonatal Sepsisreiche90% (29)
- Case Study TyphoidDocument10 pagesCase Study TyphoidArchana Sahu100% (3)
- Nursing Case Study LymphomaDocument33 pagesNursing Case Study LymphomaArnie Felipe100% (1)
- Nursing Memory JoggersDocument2 pagesNursing Memory JoggersMarcus, RN96% (24)
- Schools As Centers For Health Educational Initiatives Health Behavior Research and Risk Behavior For DengueDocument20 pagesSchools As Centers For Health Educational Initiatives Health Behavior Research and Risk Behavior For DengueRainforestLeadership MccaPas encore d'évaluation
- Case+Study+Dengue FinalDocument21 pagesCase+Study+Dengue FinalNinz NunezPas encore d'évaluation
- Case Study On PneumoniaDocument31 pagesCase Study On PneumoniaLarah Mae Andog85% (20)
- Bronchopneumonia Case PresentationDocument17 pagesBronchopneumonia Case Presentationgandhialpit100% (1)
- Case Study On Dengue FeverDocument76 pagesCase Study On Dengue FeverMary Rose Silva Gargar0% (1)
- Casestudy DengueDocument57 pagesCasestudy DengueMJ Amarillo93% (14)
- Dengue Fever Case StudyDocument55 pagesDengue Fever Case StudyGlory Holmes67% (6)
- Case Dengue)Document66 pagesCase Dengue)mackmon100% (1)
- Case Study On DengueDocument19 pagesCase Study On DengueOlivia Gianchand100% (2)
- A Case Study On Dengue FeverDocument10 pagesA Case Study On Dengue FeverRinrin de BelenPas encore d'évaluation
- Nursing Case Study Dengue FeverDocument7 pagesNursing Case Study Dengue FeverEdilyn BalicaoPas encore d'évaluation
- Dengue Fever Case StudyDocument5 pagesDengue Fever Case StudyJen Faye Orpilla100% (1)
- Clinical Case Study of DengueDocument64 pagesClinical Case Study of DengueAyiems AiemsPas encore d'évaluation
- Case Study: Rle: Dengue Hemorrhagic FeverDocument7 pagesCase Study: Rle: Dengue Hemorrhagic FeverNikka Moreen Dagdag0% (1)
- Case Presentation DengueDocument3 pagesCase Presentation DengueLindel Assley Turqueza100% (1)
- Case Study DengueDocument10 pagesCase Study DengueKathleen VargasPas encore d'évaluation
- Case Study 5 Dengue Fever CorrectedDocument13 pagesCase Study 5 Dengue Fever CorrectedyounggirldavidPas encore d'évaluation
- A Case Study of Dengue FeverDocument19 pagesA Case Study of Dengue FeverDanny Shrestha100% (1)
- Dengue CaseDocument27 pagesDengue CaseBabyrlene Padilla Añabieza RN100% (4)
- Case Study DengueDocument10 pagesCase Study DengueBasmah A. AdompingPas encore d'évaluation
- Dengue Case StudyDocument8 pagesDengue Case StudysusanausquizaPas encore d'évaluation
- Malaria CASE Presentation by (Harvey) Bingtot21Document52 pagesMalaria CASE Presentation by (Harvey) Bingtot21bingtot21927100% (12)
- Case Study PneumoniaDocument45 pagesCase Study PneumoniaYashoda Satpute83% (6)
- A Case Study On DengueDocument11 pagesA Case Study On DengueYetTamparong100% (1)
- Dengue Case StudyDocument23 pagesDengue Case Studycutie_0023Pas encore d'évaluation
- Case Study On Pneumonia (Real)Document28 pagesCase Study On Pneumonia (Real)Gleevyn Dela Torre86% (7)
- Typhoid FeverDocument23 pagesTyphoid FeverMaden Jayona HaliliPas encore d'évaluation
- Case Study - DengueDocument28 pagesCase Study - DengueAlecs LunganPas encore d'évaluation
- Case Study For Dengue FeverDocument11 pagesCase Study For Dengue FeverPrecious SorianoPas encore d'évaluation
- Case Study Dengue FeverDocument4 pagesCase Study Dengue FeverGerard Guevarra0% (1)
- Case Study - Dengue FeverDocument61 pagesCase Study - Dengue FeverFrancis AdrianPas encore d'évaluation
- Case Study PneumoniaDocument12 pagesCase Study PneumoniaFretzie Mae RamasPas encore d'évaluation
- CcroupDocument53 pagesCcroupOlivia BernadiPas encore d'évaluation
- Case Study-Chronic TonsillitisDocument7 pagesCase Study-Chronic TonsillitisJonalyn TumanguilPas encore d'évaluation
- Case Study On TBDocument3 pagesCase Study On TBJamil Lorca75% (8)
- NURSING CARE PLAN PneumoniaDocument38 pagesNURSING CARE PLAN PneumoniaLuna JadePas encore d'évaluation
- A. Biographical DataDocument6 pagesA. Biographical DataDRAPas encore d'évaluation
- Age - For SubmissionDocument27 pagesAge - For SubmissionAdrian MallarPas encore d'évaluation
- Stab Wound Case StudyDocument33 pagesStab Wound Case StudyAdrian MallarPas encore d'évaluation
- Flail Chest (Tayug)Document25 pagesFlail Chest (Tayug)Adrian MallarPas encore d'évaluation
- Geriatric Assessment ToolDocument5 pagesGeriatric Assessment ToolRoel John Atamosa CasilacPas encore d'évaluation
- Datuin - PediaDocument13 pagesDatuin - PediaMika SaldañaPas encore d'évaluation
- Case 1-Clinical Case StudyDocument4 pagesCase 1-Clinical Case StudyRachel VillanuevaPas encore d'évaluation
- Urinary Tract InfectionDocument18 pagesUrinary Tract InfectionljefarrahPas encore d'évaluation
- A Narrative Report On: Physical AssesmentDocument11 pagesA Narrative Report On: Physical AssesmentchelseyPas encore d'évaluation
- Case Study On Chronic Kidney DiseaseDocument9 pagesCase Study On Chronic Kidney DiseaseHalles Beverlyn Crisostomo GeraldePas encore d'évaluation
- Growth and Development Case Study grp1Document7 pagesGrowth and Development Case Study grp1sleep whatPas encore d'évaluation
- Case Study CholecystitisDocument33 pagesCase Study CholecystitisMelai de GuzmanPas encore d'évaluation
- Identification: Vulnerable Individual (Assessment)Document20 pagesIdentification: Vulnerable Individual (Assessment)Nik Rose ElPas encore d'évaluation
- CA (Angina, Myocardial InfarctionDocument4 pagesCA (Angina, Myocardial InfarctionAdrian MallarPas encore d'évaluation
- Flail Chest (Tayug)Document25 pagesFlail Chest (Tayug)Adrian MallarPas encore d'évaluation
- College of Nursing: Homer D. Elegado BSN 3ADocument12 pagesCollege of Nursing: Homer D. Elegado BSN 3AAdrian MallarPas encore d'évaluation
- Casestudy FractureDocument22 pagesCasestudy FractureAdrian Mallar0% (1)
- HyperkalemiaDocument10 pagesHyperkalemiaAdrian MallarPas encore d'évaluation
- Tuberculosis Grand Case 2.0Document25 pagesTuberculosis Grand Case 2.0Adrian MallarPas encore d'évaluation
- Pathophysiology Siquig EmersonDocument4 pagesPathophysiology Siquig EmersonAdrian Mallar100% (1)
- Risk For Imbalance NutirionDocument2 pagesRisk For Imbalance NutirionAdrian MallarPas encore d'évaluation
- Community Health Nursing p.31-55Document25 pagesCommunity Health Nursing p.31-55Adrian MallarPas encore d'évaluation
- Diabetic RetinopathyDocument2 pagesDiabetic RetinopathyAdrian MallarPas encore d'évaluation
- CA (Angina, Myocardial InfarctionDocument4 pagesCA (Angina, Myocardial InfarctionAdrian MallarPas encore d'évaluation
- Orthopedic Case StudyDocument8 pagesOrthopedic Case StudyAdrian Mallar100% (1)
- Psychiatric NursingDocument15 pagesPsychiatric NursingAdrian MallarPas encore d'évaluation
- NCP Deficient KnowledgeDocument1 pageNCP Deficient KnowledgeAdrian Mallar67% (3)
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarPas encore d'évaluation
- Legg Calve PerthesDocument7 pagesLegg Calve PerthesAdrian Mallar100% (1)
- HyperkalemiaDocument10 pagesHyperkalemiaAdrian MallarPas encore d'évaluation
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarPas encore d'évaluation
- Activity IntoleranceDocument1 pageActivity IntoleranceAdrian MallarPas encore d'évaluation
- Fluid Volume Loss NCP - PediaDocument2 pagesFluid Volume Loss NCP - PediaAdrian MallarPas encore d'évaluation
- Chest Tube ThoracostomyDocument1 pageChest Tube ThoracostomyFritz Regis W. TumaponPas encore d'évaluation
- Activity IntoleranceDocument1 pageActivity IntoleranceAdrian MallarPas encore d'évaluation
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byDocument7 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byAdrian MallarPas encore d'évaluation
- Case Study HerniaDocument7 pagesCase Study HerniaAdrian MallarPas encore d'évaluation
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaAdrian Mallar100% (1)
- Format of Head Nursing Requirement-1Document13 pagesFormat of Head Nursing Requirement-1Adrian MallarPas encore d'évaluation
- Format of Head Nursing Requirement-1Document13 pagesFormat of Head Nursing Requirement-1Adrian MallarPas encore d'évaluation
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarPas encore d'évaluation
- Components of LaborDocument1 pageComponents of LaborAdrian MallarPas encore d'évaluation
- Teaching PlanDocument3 pagesTeaching PlanJaninaPatriciaB100% (2)
- VIRAL Robin Cook ExcerptDocument18 pagesVIRAL Robin Cook ExcerptOtid DellmhalPas encore d'évaluation
- Effective Alternative Mosquito Repellent From Lemongrass As Candle Based FormulationDocument14 pagesEffective Alternative Mosquito Repellent From Lemongrass As Candle Based FormulationFaith LagguiPas encore d'évaluation
- Do Mosquitos Actually Bite Some People More Than Others - Maria Elena de ObaldiaDocument3 pagesDo Mosquitos Actually Bite Some People More Than Others - Maria Elena de Obaldiamc7mqymdj4Pas encore d'évaluation
- Right Form of Verbs Board Question Exercise For SSC Till 2022Document6 pagesRight Form of Verbs Board Question Exercise For SSC Till 2022topuajt0% (1)
- Vector and Pest ControlDocument10 pagesVector and Pest ControlTaufik RizkiandiPas encore d'évaluation
- 2012 Training Manual Malaria EntomologyDocument85 pages2012 Training Manual Malaria EntomologyAntony RajPas encore d'évaluation
- Chapter 2.tapos NaDocument8 pagesChapter 2.tapos NaIza Tom100% (1)
- Chapter 2 Unfinished RRLDocument22 pagesChapter 2 Unfinished RRLGM XylerPas encore d'évaluation
- Class V Evs Question Bank Sa1 SdsdsdsdsdsdssDocument41 pagesClass V Evs Question Bank Sa1 SdsdsdsdsdsdssAshok L Joshi83% (29)
- Kangkong (Ipomoea Aquatica) : A Wriggler Killer: An Investigatory Project Presented ToDocument11 pagesKangkong (Ipomoea Aquatica) : A Wriggler Killer: An Investigatory Project Presented ToAries Palao Austria100% (1)
- Natural Disasters: Archangela Averina Zora Xii Bahasa / 6Document4 pagesNatural Disasters: Archangela Averina Zora Xii Bahasa / 6XII BHS / 6 Archangela Averina ZPas encore d'évaluation
- Typhoid and Dengue PPT by Shefali RanaDocument47 pagesTyphoid and Dengue PPT by Shefali RanariyaPas encore d'évaluation
- Peperiksaan Akhir Tahun Terengganu Tingkatan 4 - Paper 2Document11 pagesPeperiksaan Akhir Tahun Terengganu Tingkatan 4 - Paper 2Alaister Bernard Jampong75% (4)
- Code of ConductDocument8 pagesCode of ConductSabine RoperPas encore d'évaluation
- Sample Proposal 1 - DengueDocument8 pagesSample Proposal 1 - Dengueazliothman100% (1)
- ManufuckingscriptDocument13 pagesManufuckingscript가푸타Pas encore d'évaluation
- Aedes Species in Laboratory"Document3 pagesAedes Species in Laboratory"International Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Schematic Diagram: Predisposing PrecipitatingDocument5 pagesSchematic Diagram: Predisposing PrecipitatingKarl Wesley DillozonPas encore d'évaluation
- Summary of Essential Oils of Cupressus FunebrisDocument4 pagesSummary of Essential Oils of Cupressus Funebrisapi-314966571Pas encore d'évaluation
- B2 English Test International Students - TemplateDocument5 pagesB2 English Test International Students - TemplateScarletRosePas encore d'évaluation
- Life Cycle of A Mosquito TemplateDocument1 pageLife Cycle of A Mosquito TemplateLulu IeqaPas encore d'évaluation
- PHD Research ProposalDocument8 pagesPHD Research ProposalMalik Ijaz Khan100% (1)
- Chapter 8 Water Sanitation and Hygiene in EmergenciesDocument70 pagesChapter 8 Water Sanitation and Hygiene in Emergenciesexponent3100% (1)
- Dengue ReportDocument48 pagesDengue ReportRuthy SegoviaPas encore d'évaluation
- Microorganisms and Its TypesDocument11 pagesMicroorganisms and Its TypesPanav AgarwalPas encore d'évaluation
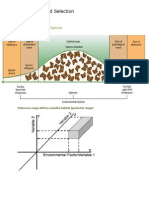
- Habitat Niche and SelectionDocument5 pagesHabitat Niche and SelectionSavannah Simone PetrachenkoPas encore d'évaluation
- AaDocument3 pagesAaDaniel DanaoPas encore d'évaluation