Vous aimerez peut-être aussi
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913D'EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Pas encore d'évaluation
- TRABECULECTOMY Complications FinalDocument31 pagesTRABECULECTOMY Complications FinalalfarizyjefryPas encore d'évaluation
- Chapter 11 Eye & Vision DisordersDocument72 pagesChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSAPas encore d'évaluation
- Diseases of Lacrimal ApparatusDocument46 pagesDiseases of Lacrimal Apparatusসপ্নে ছোয়া মন100% (1)
- Optic NeuritisDocument32 pagesOptic NeuritisNajaf Ali Khan100% (1)
- Week 4 - Development of The EyeDocument5 pagesWeek 4 - Development of The EyeAleia GoPas encore d'évaluation
- Embryology of Eye - 1Document12 pagesEmbryology of Eye - 1Maitha AlwhshiPas encore d'évaluation
- Ocular Manifestations of Thyroid DiseaseDocument20 pagesOcular Manifestations of Thyroid Diseasevivekrajbhilai5850Pas encore d'évaluation
- Lecture Three Convergence and Accommodation (AC/A) : Mr. Natnael L. (Lecturer) April/2017Document33 pagesLecture Three Convergence and Accommodation (AC/A) : Mr. Natnael L. (Lecturer) April/2017henok birukPas encore d'évaluation
- Introduction To The EyeDocument18 pagesIntroduction To The EyeJúnior Alves100% (1)
- Lacrimal System and Disorders: DR Asad FrazDocument30 pagesLacrimal System and Disorders: DR Asad FrazAsad Fraz0% (1)
- Mechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthDocument7 pagesMechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthQomariah RiaPas encore d'évaluation
- Colour Vision AnomaliesDocument27 pagesColour Vision AnomaliesGershon HayfordPas encore d'évaluation
- Clinical Orthoptics 2019Document97 pagesClinical Orthoptics 2019Joseph IsraelPas encore d'évaluation
- Nungki-Esodeviations & ExodeviationsDocument36 pagesNungki-Esodeviations & ExodeviationsNia RoosdhantiaPas encore d'évaluation
- Basic Eye ExamDocument8 pagesBasic Eye ExamLisa AguilarPas encore d'évaluation
- Share Myopia Mcqs'sDocument4 pagesShare Myopia Mcqs'sshumaila khan50% (2)
- Orientation, History Taking and ExaminationDocument77 pagesOrientation, History Taking and ExaminationMuhammad AwaisPas encore d'évaluation
- Retinoscopy: Moderator:-Dr. Jyoti PuriDocument33 pagesRetinoscopy: Moderator:-Dr. Jyoti PuriSafa Abdualrahaman Ali HamadPas encore d'évaluation
- Strabismus Quick GuideDocument4 pagesStrabismus Quick Guideghitza80100% (1)
- Blood Supply, Nerve Supply and Lymphatics of The OrbitDocument28 pagesBlood Supply, Nerve Supply and Lymphatics of The OrbitPallavi Uday NaikPas encore d'évaluation
- Degenerative MyopiaDocument53 pagesDegenerative MyopiaNiloy BasakPas encore d'évaluation
- OculomotorDocument41 pagesOculomotorcmirceaPas encore d'évaluation
- Frame SelectionDocument21 pagesFrame Selectionhenok birukPas encore d'évaluation
- OPTICS Revised + Extra QsDocument75 pagesOPTICS Revised + Extra Qsdoaa naieemPas encore d'évaluation
- RGP Lens MeasurementDocument5 pagesRGP Lens MeasurementSumon SarkarPas encore d'évaluation
- Incomitant SquintDocument41 pagesIncomitant Squintshreeja maheshwari100% (3)
- UveaDocument83 pagesUveaShewit TeklehaymanotPas encore d'évaluation
- CLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationDocument26 pagesCLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationRhendy 172019022Pas encore d'évaluation
- Blurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocDocument15 pagesBlurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocRea Dominique CabanillaPas encore d'évaluation
- Smith Test, Goniolens, Shadow TestDocument3 pagesSmith Test, Goniolens, Shadow TestJLo100% (1)
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Cornea-Anatomy and PhysiologyDocument10 pagesCornea-Anatomy and PhysiologyMido KimoPas encore d'évaluation
- Opticalprescriptions2010 1938 1938Document60 pagesOpticalprescriptions2010 1938 1938PRANEET MISHRA100% (1)
- Artificial TearsDocument36 pagesArtificial TearsFahmi Rizal100% (1)
- Anatomy of Uvea: Dr. Binu AsharafDocument48 pagesAnatomy of Uvea: Dr. Binu AsharafBinu AshrafPas encore d'évaluation
- Optometry PresDocument31 pagesOptometry Pressafna saleemPas encore d'évaluation
- Paediatric Contact LenseDocument63 pagesPaediatric Contact LenseGurria NaheedPas encore d'évaluation
- CPG 19Document78 pagesCPG 19anon-24970100% (1)
- Diseases of LensDocument42 pagesDiseases of LensAmmad ShahidPas encore d'évaluation
- Investigation in OptometryDocument10 pagesInvestigation in Optometryrapid73Pas encore d'évaluation
- Concomitant SquintDocument21 pagesConcomitant SquintShivani NairPas encore d'évaluation
- Investigative Techniques & Ocular Examination - Sandip DoshiDocument161 pagesInvestigative Techniques & Ocular Examination - Sandip DoshiShifan Abdul MajeedPas encore d'évaluation
- Development of Binocular Vision: University of Gondar Department of Optometry by Nebiyat FelekeDocument35 pagesDevelopment of Binocular Vision: University of Gondar Department of Optometry by Nebiyat Felekehenok birukPas encore d'évaluation
- Refractive Errors: Dr. Leow Thye YngDocument55 pagesRefractive Errors: Dr. Leow Thye YngRaissaPas encore d'évaluation
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamPas encore d'évaluation
- Direct OphthalmoscopeDocument16 pagesDirect OphthalmoscopeMuhammed AbdulmajeedPas encore d'évaluation
- Episkleritis Dan SkleritisDocument41 pagesEpiskleritis Dan SkleritisSuryana AdityaPas encore d'évaluation
- Case ReportDocument29 pagesCase ReportRaisa AriesthaPas encore d'évaluation
- Surgical Procedures That Change Refracting Ability of Eye:: Different Types of Refractive SurgeryDocument12 pagesSurgical Procedures That Change Refracting Ability of Eye:: Different Types of Refractive Surgeryblack00swanPas encore d'évaluation
- What Is Retinoscopy?: Myopia HyperopiaDocument4 pagesWhat Is Retinoscopy?: Myopia HyperopiababyswitPas encore d'évaluation
- Prescribing Lenses - Troubleshooting .Document65 pagesPrescribing Lenses - Troubleshooting .KhairunnisaPas encore d'évaluation
- Pediatric Eye Examination: Seia MahananiDocument35 pagesPediatric Eye Examination: Seia MahananiRaissaPas encore d'évaluation
- RefraksiDocument84 pagesRefraksinaroetocapkutilPas encore d'évaluation
- Dispensing 204 Tutorial 201-1Document2 pagesDispensing 204 Tutorial 201-1Basildon MukorombindoPas encore d'évaluation
- Visual Field InterpretationsDocument35 pagesVisual Field InterpretationsAhmadhassan RanaPas encore d'évaluation
- Introduction To Spherical Lenses2Document6 pagesIntroduction To Spherical Lenses2Nuon HudaPas encore d'évaluation
- Optics - Contact Lens Related - MMSDocument38 pagesOptics - Contact Lens Related - MMSManmohan ShahPas encore d'évaluation
- Periorbital and Orbital CellulitisDocument51 pagesPeriorbital and Orbital CellulitisJoanne BlancoPas encore d'évaluation
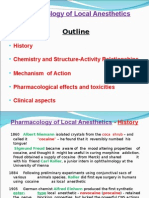
- Pharmacology of Local AnestheticsDocument32 pagesPharmacology of Local AnestheticsJk FloresPas encore d'évaluation
- ARTHRITISDocument4 pagesARTHRITISJk FloresPas encore d'évaluation
- Metabolic Bone DiseasesDocument55 pagesMetabolic Bone DiseasesJk FloresPas encore d'évaluation
- Anatomy Mcqs With AnswersDocument8 pagesAnatomy Mcqs With AnswersJk Flores67% (6)
- Glaucoma and CataractDocument30 pagesGlaucoma and CataractJayselle ArviePas encore d'évaluation
- GLAUCOMA (Class 7) : Faculty Name Institute NameDocument32 pagesGLAUCOMA (Class 7) : Faculty Name Institute NamePranshu Prajyot 67Pas encore d'évaluation
- Approach To The Adult With Acute Persistent Visual Loss - UpToDateDocument2 pagesApproach To The Adult With Acute Persistent Visual Loss - UpToDateCalvin LooPas encore d'évaluation
- Visual DisordersDocument21 pagesVisual DisordersJobelle Acena100% (1)
- Anatomical & Physiological Changes With AgingDocument9 pagesAnatomical & Physiological Changes With AgingIqra AzizPas encore d'évaluation
- Ophthalmology: Cataract Surgery in Eyes With Pseudoexfoliation (PEX) SyndromeDocument5 pagesOphthalmology: Cataract Surgery in Eyes With Pseudoexfoliation (PEX) SyndromeCahya AlfalizaPas encore d'évaluation
- CEI Training Manual 2014 PDFDocument43 pagesCEI Training Manual 2014 PDFswasahmedPas encore d'évaluation
- E-Book Ophthalmology Referral Guide For GPsDocument11 pagesE-Book Ophthalmology Referral Guide For GPsnaravichandran3662Pas encore d'évaluation
- Vasan Eye CareDocument13 pagesVasan Eye CareGokul BalajiPas encore d'évaluation
- Dwnload Full The Ophthalmic Assistant e Book A Text For Allied and Associated Ophthalmic Personnel PDFDocument51 pagesDwnload Full The Ophthalmic Assistant e Book A Text For Allied and Associated Ophthalmic Personnel PDFebony.blanchard21195% (22)
- Trabeculectomy-Induced Hypotony: When and How To Intervene: Clinical UpdateDocument3 pagesTrabeculectomy-Induced Hypotony: When and How To Intervene: Clinical UpdateROMOPas encore d'évaluation
- Cover Sarpus 1 GREDocument7 pagesCover Sarpus 1 GREGracia HarahapPas encore d'évaluation
- 002 Block 2 SDocument56 pages002 Block 2 SAlan DaaboulPas encore d'évaluation
- NCPDocument3 pagesNCPLornz E. Cantos100% (1)
- Trauma OcularDocument10 pagesTrauma OcularEmigdioPas encore d'évaluation
- Chapter 50 Vision and HearingDocument7 pagesChapter 50 Vision and HearingAlmer OstreaPas encore d'évaluation
- Glaucoma in Dog A Case Report-Dr. Jibachha SahDocument8 pagesGlaucoma in Dog A Case Report-Dr. Jibachha SahDr.Jibachha Sah,Vet.physician,author, & motivatorPas encore d'évaluation
- GlaucomaDocument31 pagesGlaucomaJake Albert MiguelPas encore d'évaluation
- Weinreb 2014Document11 pagesWeinreb 2014José Adrian Espejel GuzmánPas encore d'évaluation
- 17) Efocus Phase 2 A Randomised Crossover Trial of Smartphone & Direct Fundoscopy For Medical StudentsDocument16 pages17) Efocus Phase 2 A Randomised Crossover Trial of Smartphone & Direct Fundoscopy For Medical StudentshasdiniPas encore d'évaluation
- Suturas Liberables Ejo.5000718Document8 pagesSuturas Liberables Ejo.5000718Emile NumberPas encore d'évaluation
- PIIS000293942200407XDocument13 pagesPIIS000293942200407XAnca Florina GaceaPas encore d'évaluation
- Disease Entity: Edit SourceDocument18 pagesDisease Entity: Edit SourceResya IntannabilaPas encore d'évaluation
- gt0912 F4 LarocheDocument3 pagesgt0912 F4 LarocheMichael CranePas encore d'évaluation
- Medical Management of GlaucomaDocument43 pagesMedical Management of Glaucomahemnath rajendran100% (1)
- Cataract Case PresentationDocument7 pagesCataract Case PresentationShahbaz AAnsariPas encore d'évaluation
- Oxidative Stress and Antioxidants - Their Role in Human Disease-Nova Biomedical Books (2009)Document374 pagesOxidative Stress and Antioxidants - Their Role in Human Disease-Nova Biomedical Books (2009)io montoya v100% (1)
- Myopic Optic Disc Changes and Its Role in GlaucomaDocument8 pagesMyopic Optic Disc Changes and Its Role in GlaucomaValentina Gracia ReyPas encore d'évaluation
- Application of Marketing Strategies To Re - Launch The ProductDocument39 pagesApplication of Marketing Strategies To Re - Launch The ProductChintan ManekPas encore d'évaluation
- Glaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorDocument22 pagesGlaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorWulandari EmyPas encore d'évaluation
- Secrets of the Millionaire Mind: Mastering the Inner Game of WealthD'EverandSecrets of the Millionaire Mind: Mastering the Inner Game of WealthÉvaluation : 4.5 sur 5 étoiles4.5/5 (197)
- Proof of Heaven: A Neurosurgeon's Journey into the AfterlifeD'EverandProof of Heaven: A Neurosurgeon's Journey into the AfterlifeÉvaluation : 3.5 sur 5 étoiles3.5/5 (165)
- The Game: Penetrating the Secret Society of Pickup ArtistsD'EverandThe Game: Penetrating the Secret Society of Pickup ArtistsÉvaluation : 4 sur 5 étoiles4/5 (131)
- New Zealand Adventure Travel GuideD'EverandNew Zealand Adventure Travel GuideÉvaluation : 4.5 sur 5 étoiles4.5/5 (14)
- Geneva, Lausanne, Fribourg & Western Switzerland Travel AdventuresD'EverandGeneva, Lausanne, Fribourg & Western Switzerland Travel AdventuresPas encore d'évaluation
- Coastal Alaska & the Inside Passage Adventure Travel GuideD'EverandCoastal Alaska & the Inside Passage Adventure Travel GuidePas encore d'évaluation
- Maui, Lanai & Molokai Adventure Travel GuideD'EverandMaui, Lanai & Molokai Adventure Travel GuideÉvaluation : 4 sur 5 étoiles4/5 (1)
- Jamaica: A Guide to the Food & RestaurantsD'EverandJamaica: A Guide to the Food & RestaurantsÉvaluation : 4 sur 5 étoiles4/5 (1)
- Hollywood & the Best of Los Angeles Travel GuideD'EverandHollywood & the Best of Los Angeles Travel GuideÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)