Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Lab 8 - Self Mon3Document48 pagesLab 8 - Self Mon3pinkCherri100% (4)
- Sewage Treatment PlantDocument12 pagesSewage Treatment Plantanuj dhavanPas encore d'évaluation
- Planetary ThreadsDocument2 pagesPlanetary ThreadsViviana PueblaPas encore d'évaluation
- Acupuncture Standards China Baoyan 2009Document50 pagesAcupuncture Standards China Baoyan 2009Marlon RamirezPas encore d'évaluation
- Gas Exchange in HumansDocument9 pagesGas Exchange in HumanscherylrachelPas encore d'évaluation
- Contekan KodeDocument4 pagesContekan KodeTessa Safitri KotoPas encore d'évaluation
- Health Drug Free BrochureDocument2 pagesHealth Drug Free BrochureAlex La RondellePas encore d'évaluation
- Perioperative Nursing 50 ItemsDocument4 pagesPerioperative Nursing 50 ItemsKrestel Saligumba Palanog100% (3)
- Hiv 101Document33 pagesHiv 101Hend Al-RamahiPas encore d'évaluation
- Case Report FinalDocument21 pagesCase Report FinalAyen FornollesPas encore d'évaluation
- Measles (Campak, Rubeola, Gabak, Kerumut)Document20 pagesMeasles (Campak, Rubeola, Gabak, Kerumut)Ami UtamiatiPas encore d'évaluation
- Persian NutritionDocument8 pagesPersian NutritionAndri FerdianPas encore d'évaluation
- Malaprabha Biogas Plant Developed by DR S V MapuskarDocument40 pagesMalaprabha Biogas Plant Developed by DR S V Mapuskarsvmapuskar4914100% (3)
- A 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Document94 pagesA 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Chee Yung NgPas encore d'évaluation
- PL3257 Tutorial 5 Emotion RegulationDocument18 pagesPL3257 Tutorial 5 Emotion RegulationRobin TanPas encore d'évaluation
- Types of Diagnosis:: Problem-Focused Nursing Diagnoses Have Three Components: (1) Nursing DiagnosisDocument4 pagesTypes of Diagnosis:: Problem-Focused Nursing Diagnoses Have Three Components: (1) Nursing DiagnosisDaisy MellaPas encore d'évaluation
- Pranashakty EbrochureDocument6 pagesPranashakty EbrochureMuay KhanPas encore d'évaluation
- Fetal EchocardiographyDocument3 pagesFetal EchocardiographypolygonePas encore d'évaluation
- Collaborative Couple Therapy: Page Pr/gurman3.htm&dir Pp/fac&cart - IdDocument39 pagesCollaborative Couple Therapy: Page Pr/gurman3.htm&dir Pp/fac&cart - IdCarlos InfantePas encore d'évaluation
- JumpSTART Training Presentation Instructor Course 2016 FinalDocument109 pagesJumpSTART Training Presentation Instructor Course 2016 FinalvictorioPas encore d'évaluation
- Lesson 6 Documentation of Pharmacotherapy InterventionsDocument1 pageLesson 6 Documentation of Pharmacotherapy InterventionsVincent Joshua TriboPas encore d'évaluation
- Osteoporosis and Fragility Fractures Surgical PerpspectiveDocument54 pagesOsteoporosis and Fragility Fractures Surgical PerpspectiveSonal DudaniPas encore d'évaluation
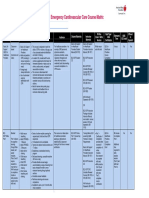
- Emergency Cardiovascular Care Course MatrixDocument15 pagesEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaPas encore d'évaluation
- Informed Consent Form Whole30 2017Document1 pageInformed Consent Form Whole30 2017api-385355641Pas encore d'évaluation
- Holistic VillageDocument5 pagesHolistic VillagemeghadurganPas encore d'évaluation
- Central Auditory PathwaysDocument31 pagesCentral Auditory Pathwayslion2chPas encore d'évaluation
- Insect Bites StingsDocument1 pageInsect Bites StingsnamibadiPas encore d'évaluation
- Imp Questions in PharmacologyDocument5 pagesImp Questions in PharmacologyBeerasandrapalyaRangaiahRavikumar100% (3)
- Filler Rhinoplasty: Evidence, Outcomes, and ComplicationsDocument3 pagesFiller Rhinoplasty: Evidence, Outcomes, and ComplicationsАндрей ПетровPas encore d'évaluation
- LHT 9 Week 5 and 6Document6 pagesLHT 9 Week 5 and 6Aubrey Lynn JoyohoyPas encore d'évaluation