Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Phenol - Medical Management Guidelines - Toxic Substance Portal - ATSDR. (N.D.) - Agency ForDocument2 pagesPhenol - Medical Management Guidelines - Toxic Substance Portal - ATSDR. (N.D.) - Agency ForREBEKAH EQUIZPas encore d'évaluation
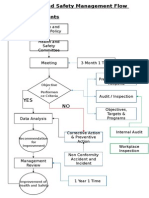
- Health and Safety FlowDocument6 pagesHealth and Safety Flowzaki0304Pas encore d'évaluation
- Challenges Facing People With Disabilities and Possible Solutions in TanzaniaDocument8 pagesChallenges Facing People With Disabilities and Possible Solutions in TanzaniaKo ReaPas encore d'évaluation
- Subdural HematomaDocument20 pagesSubdural HematomaArief Zamir100% (1)
- HESI Comprehensive ReviewDocument4 pagesHESI Comprehensive ReviewJeffrey Viernes50% (2)
- Thesis About Quack DoctorsDocument22 pagesThesis About Quack DoctorsJervyn Guianan100% (3)
- Case Study 2Document12 pagesCase Study 2api-336539272Pas encore d'évaluation
- The Geisha Secret Ancient Dating Rituals Proven To Win A Modern Mans Heart Hanako Z LibraryDocument165 pagesThe Geisha Secret Ancient Dating Rituals Proven To Win A Modern Mans Heart Hanako Z LibraryMarius CristianPas encore d'évaluation
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Thrombotic Disorders Part 2Document7 pagesThrombotic Disorders Part 2KAJAL SINGHPas encore d'évaluation
- Ebook Ebook PDF Personal Stress Management From Surviving To Thriving PDFDocument41 pagesEbook Ebook PDF Personal Stress Management From Surviving To Thriving PDFtina.cousins322100% (37)
- Dunway Test PaperDocument73 pagesDunway Test PaperShivendu Sharma92% (12)
- Fortisian 5 MBDocument44 pagesFortisian 5 MBBadass BitchPas encore d'évaluation
- EWC 661 English For Report Writing: Prepared By: NO Name Student IdDocument7 pagesEWC 661 English For Report Writing: Prepared By: NO Name Student IdAthirah Dinata100% (1)
- Priyanka Sen Final Practice School Internship ReportDocument35 pagesPriyanka Sen Final Practice School Internship ReportThakur Aditya PratapPas encore d'évaluation
- Striano - Can Psychotherapists Hurt You (1988)Document146 pagesStriano - Can Psychotherapists Hurt You (1988)Doron SabariPas encore d'évaluation
- Effect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieDocument7 pagesEffect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieMohammedPas encore d'évaluation
- Thesis About Abortion in The PhilippinesDocument8 pagesThesis About Abortion in The PhilippinesBuyingCollegePapersBatonRouge100% (2)
- Cognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingDocument19 pagesCognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingIsmael RodriguezPas encore d'évaluation
- The Right To Die: Pre-ReadingDocument8 pagesThe Right To Die: Pre-ReadingGiovanni EscobarPas encore d'évaluation
- PSC Advert - 14.9.2021 2Document15 pagesPSC Advert - 14.9.2021 2Derrick Ombura NazleyPas encore d'évaluation
- SDS 80 Fat Unsalted Butter Lactic AcidDocument8 pagesSDS 80 Fat Unsalted Butter Lactic Acidfiyan maulanaPas encore d'évaluation
- Gulayan Sa PaaralanDocument5 pagesGulayan Sa PaaralanLani DolleroPas encore d'évaluation
- Chapter 4. Ergonomics Hazards and Risks ManagementDocument46 pagesChapter 4. Ergonomics Hazards and Risks Managementmich abi100% (1)
- XLL Practice SampleDocument4 pagesXLL Practice SampleAkshita BatraPas encore d'évaluation
- Oxoid WERCSContentDocument9 pagesOxoid WERCSContentAriyanti PrakosaPas encore d'évaluation
- A Client With Cushing's Syndrome: Nursing Care PlanDocument1 pageA Client With Cushing's Syndrome: Nursing Care PlanJulius Caesar ColladoPas encore d'évaluation
- COVID CertificateDocument1 pageCOVID CertificateshibiranPas encore d'évaluation
- Q2 Grade 7 HEALTH DLL Week 1Document10 pagesQ2 Grade 7 HEALTH DLL Week 1Jet Arcangel Laroco LarocoPas encore d'évaluation
- Nursing TherapyDocument121 pagesNursing TherapyIra AarisPas encore d'évaluation