Vous aimerez peut-être aussi
- Liver Function in Early Lyme PDFDocument6 pagesLiver Function in Early Lyme PDFiri_balPas encore d'évaluation
- Lyme Combat IVDocument51 pagesLyme Combat IViri_balPas encore d'évaluation
- ULDN Inverse Titration Protocol FINALDocument50 pagesULDN Inverse Titration Protocol FINALiri_bal100% (2)
- Naltrexone and Autoimmune Disease - Grandpa's Cmpding RXDocument6 pagesNaltrexone and Autoimmune Disease - Grandpa's Cmpding RXiri_balPas encore d'évaluation
- Brain Wave VibrationDocument6 pagesBrain Wave Vibrationiri_bal100% (2)
- Alternative DietDocument31 pagesAlternative Dietiri_balPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Impaired Urinary EliminationDocument5 pagesImpaired Urinary Eliminationapi-279878989Pas encore d'évaluation
- UNIT 16 Spa Treatments Syllabus V2Document7 pagesUNIT 16 Spa Treatments Syllabus V2Jowie SooPas encore d'évaluation
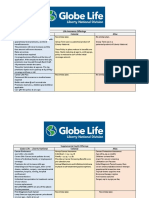
- Life Insurance Offerings Globe Life - Liberty National Colonial AflacDocument3 pagesLife Insurance Offerings Globe Life - Liberty National Colonial AflacTina Hughes0% (1)
- Lec - 4 - Risk AnalysisDocument22 pagesLec - 4 - Risk Analysisحسن خالد وسوPas encore d'évaluation
- Sarcoma Surveillance A Review of Current Evidence.2Document12 pagesSarcoma Surveillance A Review of Current Evidence.2Fernanda Lorena AcevesPas encore d'évaluation
- Miracle MineralsDocument32 pagesMiracle MineralsTURGIS100% (13)
- Immunotherapy For Lung CancerDocument3 pagesImmunotherapy For Lung CancerPongwirat ChantasoontornPas encore d'évaluation
- Grabovoi NumbersDocument17 pagesGrabovoi Numbershealthy57Pas encore d'évaluation
- It's Official! Vegetarian Centenarians Are Happier Healthier Than Aging Meat-eaters - Mrs. Nasib Kaur Surpasses 100 Years Old Eating Plant-based Diet and Loving It - Majid Ali, Nir Barzilai - Non-LowCarb Non-Paleo Longevity DietDocument3 pagesIt's Official! Vegetarian Centenarians Are Happier Healthier Than Aging Meat-eaters - Mrs. Nasib Kaur Surpasses 100 Years Old Eating Plant-based Diet and Loving It - Majid Ali, Nir Barzilai - Non-LowCarb Non-Paleo Longevity DietPaleoCentenarianDietPas encore d'évaluation
- Journal ReadingDocument29 pagesJournal ReadingAchmad YasinPas encore d'évaluation
- New GOLD Guideline 2011Document25 pagesNew GOLD Guideline 2011ebramnainggolanPas encore d'évaluation
- The Timber News! - November 2010Document20 pagesThe Timber News! - November 2010TheTimberNewsPas encore d'évaluation
- BBBBBXXDocument5 pagesBBBBBXXodi jayaPas encore d'évaluation
- Nuclear Medicine - Radioactivity For Diagnosis and TherapyDocument217 pagesNuclear Medicine - Radioactivity For Diagnosis and TherapyPriscila FloresPas encore d'évaluation
- Exam 1 PracticumDocument9 pagesExam 1 Practicumapi-310181843Pas encore d'évaluation
- Congress Program September 2022 Anglisht 1 1Document17 pagesCongress Program September 2022 Anglisht 1 1ediPas encore d'évaluation
- Leeward Microbiology 130 DR - Kae Final ExamDocument164 pagesLeeward Microbiology 130 DR - Kae Final Examraymond theardPas encore d'évaluation
- Buccal Mucosa CancerDocument9 pagesBuccal Mucosa Cancermuhammad_ariefPas encore d'évaluation
- MRCPCH - Important Skin DiseasesDocument42 pagesMRCPCH - Important Skin DiseasesarjumandPas encore d'évaluation
- Xiaoming Zhu China's Technology Innovators Selected Cases On Creating and Staying Ahead of Business TrendsDocument193 pagesXiaoming Zhu China's Technology Innovators Selected Cases On Creating and Staying Ahead of Business TrendsrezasattariPas encore d'évaluation
- Kontrasepsi: Brahmantyo Danang GuntoroDocument22 pagesKontrasepsi: Brahmantyo Danang GuntoroAzuma Asma Azizah100% (1)
- Saudi Counsel Exams For LabDocument30 pagesSaudi Counsel Exams For Labasif86% (14)
- Bio Energetic TherapyDocument19 pagesBio Energetic TherapyVishnu Moorthy Raja Singam100% (2)
- Head and Neck Laryngeal Tumors An OverviewDocument7 pagesHead and Neck Laryngeal Tumors An OverviewpupuayuwandiraPas encore d'évaluation
- Chapter 22 - The Respiratory SystemDocument15 pagesChapter 22 - The Respiratory SystemTony Snearly100% (1)
- Psa Testing A Critical Look at Current RecommendationsDocument4 pagesPsa Testing A Critical Look at Current Recommendationsapi-306915317Pas encore d'évaluation
- The Cellular Basis of Disease: Cell Injury 3 Apoptosis and Necrosis Cellular AgingDocument49 pagesThe Cellular Basis of Disease: Cell Injury 3 Apoptosis and Necrosis Cellular AgingZabella SilvianaPas encore d'évaluation
- 2 - Cell Culture LectureDocument45 pages2 - Cell Culture LectureSathvik PalakurtyPas encore d'évaluation
- Skippers United Pacific, Inc. vs. Lagne DigestDocument4 pagesSkippers United Pacific, Inc. vs. Lagne DigestEmir MendozaPas encore d'évaluation
- BRVO PPT by Dr. Chinmay KharadeDocument31 pagesBRVO PPT by Dr. Chinmay KharadeChinmay KharadePas encore d'évaluation