Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Pharmacology and The Nursing Process - Linda Lane Lilley PDFDocument2 073 pagesPharmacology and The Nursing Process - Linda Lane Lilley PDFChristopher Patch95% (20)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Catapres (Clonidine)Document2 pagesCatapres (Clonidine)Adrianne BazoPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- s37 Cello Syl RCM 2013 Online SecuredDocument102 pagess37 Cello Syl RCM 2013 Online SecuredRobertus Maharyady100% (4)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Test Bank For Basic Pharmacology For Nursing 17th EditionDocument10 pagesTest Bank For Basic Pharmacology For Nursing 17th EditionUsman HaiderPas encore d'évaluation
- Standard Operating Procedure Cold Chain ManagementDocument3 pagesStandard Operating Procedure Cold Chain ManagementDaniel Yves IV Paez100% (1)
- Objection Handling With ConfidenceDocument3 pagesObjection Handling With ConfidenceAnup Soans100% (2)
- Microencapsulation SummaryDocument48 pagesMicroencapsulation SummaryDullah Zungu100% (2)
- Philippines Pharmaceutical Country ProfileDocument347 pagesPhilippines Pharmaceutical Country Profilemrk_rlndPas encore d'évaluation
- Textbook of Forensic PharmacyDocument201 pagesTextbook of Forensic PharmacyAmbika DurgPas encore d'évaluation
- Detailed Drug StudyDocument5 pagesDetailed Drug StudyKarl Vincent SosoPas encore d'évaluation
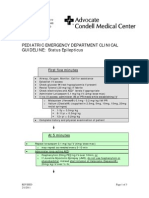
- Condell PedStatusEpilepticusGuildlines 2011Document3 pagesCondell PedStatusEpilepticusGuildlines 2011Robertus MaharyadyPas encore d'évaluation
- Health Professions Act Revised Hypoglycemia Protocol Insulin Subcutaneous Sliding ScaleDocument55 pagesHealth Professions Act Revised Hypoglycemia Protocol Insulin Subcutaneous Sliding ScaleRobertus MaharyadyPas encore d'évaluation
- Morpot TN Jhony TampubolonDocument1 pageMorpot TN Jhony TampubolonRobertus MaharyadyPas encore d'évaluation
- JNC 7 (Klasifikasi Hipertensi) PDFDocument2 pagesJNC 7 (Klasifikasi Hipertensi) PDFAbdur RahmanPas encore d'évaluation
- Cerebral Palsy PDFDocument6 pagesCerebral Palsy PDFRobertus MaharyadyPas encore d'évaluation
- Masalah: Aktif: Pasif:: PH: PP: DPJPDocument2 pagesMasalah: Aktif: Pasif:: PH: PP: DPJPRobertus MaharyadyPas encore d'évaluation
- PropanolDocument8 pagesPropanolStacey CamillePas encore d'évaluation
- Applying For Eligibility To Complete An Overseas Pharmacists Assessment Programme March 2021 3Document28 pagesApplying For Eligibility To Complete An Overseas Pharmacists Assessment Programme March 2021 3DuaaPas encore d'évaluation
- Introduction To Pharmacology by ZebDocument31 pagesIntroduction To Pharmacology by ZebSanam MalikPas encore d'évaluation
- Critical Thinking Essay-Animal Testing: Rough DraftDocument10 pagesCritical Thinking Essay-Animal Testing: Rough Draftjeremygcap2017Pas encore d'évaluation
- Introduction To Microbiology: by T. Topodzi Bpharm (Hons) University of ZimbabweDocument13 pagesIntroduction To Microbiology: by T. Topodzi Bpharm (Hons) University of ZimbabweVon Valentine MhutePas encore d'évaluation
- Dyspepsia in PregnancyDocument1 pageDyspepsia in Pregnancydownload spssPas encore d'évaluation
- Strategy of Pharmacitical IndustryDocument3 pagesStrategy of Pharmacitical IndustrysukeshPas encore d'évaluation
- Ascendant PQP1Document19 pagesAscendant PQP1Raaja VishwaPas encore d'évaluation
- HMR TemplateDocument2 pagesHMR TemplatepharmacisticusPas encore d'évaluation
- Pharma Parenteral Dosage CalculationDocument3 pagesPharma Parenteral Dosage CalculationMaxinne RoseñoPas encore d'évaluation
- CRESTOR Citizen's PetitionDocument14 pagesCRESTOR Citizen's Petitiontuckerd99Pas encore d'évaluation
- JurnalDocument7 pagesJurnalAdy Adha NorsaniePas encore d'évaluation
- Biocon Business EthicsDocument21 pagesBiocon Business EthicsNirjon Dip100% (1)
- Breast Cancer FinaleDocument30 pagesBreast Cancer Finaleخايزورا راهيمPas encore d'évaluation
- Keuntungan Dan Kerugian PastaDocument2 pagesKeuntungan Dan Kerugian PastaMiranda MilePas encore d'évaluation
- Clinical Pharmacist Health Consultant in Pittsburgh PA Resume Michele MosierDocument2 pagesClinical Pharmacist Health Consultant in Pittsburgh PA Resume Michele MosierMicheleMosierPas encore d'évaluation
- Trudell Resume 2Document2 pagesTrudell Resume 2api-323367567Pas encore d'évaluation
- Transition of CareDocument52 pagesTransition of CareAffan PresentationsPas encore d'évaluation
- Intravenous Bolus Administration Part II PDFDocument44 pagesIntravenous Bolus Administration Part II PDFAlaa MansourPas encore d'évaluation
- DR - Saleh SFDA Bioeq IntroductionDocument8 pagesDR - Saleh SFDA Bioeq IntroductionkathreentracyPas encore d'évaluation
- JPM Healthcare Conf HandoutDocument25 pagesJPM Healthcare Conf HandoutkriznanPas encore d'évaluation