Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Development Through The Lifespan: Cognitive Development in Infancy and ToddlerhoodDocument48 pagesDevelopment Through The Lifespan: Cognitive Development in Infancy and Toddlerhoodmonster40lbsPas encore d'évaluation
- Motivation and EmotionDocument56 pagesMotivation and Emotionmonster40lbsPas encore d'évaluation
- Psych 327 #15807 Sec 01 SchlussmanDocument6 pagesPsych 327 #15807 Sec 01 Schlussmanmonster40lbsPas encore d'évaluation
- Dishwasher: 24 Hours A Day, 7 Days A Week For LG Customer ServiceDocument48 pagesDishwasher: 24 Hours A Day, 7 Days A Week For LG Customer Servicemonster40lbsPas encore d'évaluation
- Psych 327 #11955 Sec 02 Schnieder - 0001Document8 pagesPsych 327 #11955 Sec 02 Schnieder - 0001monster40lbsPas encore d'évaluation
- Development, Maturation, Aging, and Death: Lecture Presentation by Suzanne Long, Monroe Community CollegeDocument62 pagesDevelopment, Maturation, Aging, and Death: Lecture Presentation by Suzanne Long, Monroe Community Collegemonster40lbsPas encore d'évaluation
- Chapter 07-IntelligenceDocument91 pagesChapter 07-Intelligencemonster40lbsPas encore d'évaluation
- Chapter 5 Powerpoint With Extra SlidesDocument111 pagesChapter 5 Powerpoint With Extra Slidesmonster40lbsPas encore d'évaluation
- 10 Memory: Reconstructing The Past The Biology of MemoryDocument60 pages10 Memory: Reconstructing The Past The Biology of Memorymonster40lbsPas encore d'évaluation
- Depression: WWW - Bradfordvts.co - UkDocument28 pagesDepression: WWW - Bradfordvts.co - Ukmonster40lbsPas encore d'évaluation
- Cook Handout AppendixDocument22 pagesCook Handout Appendixmonster40lbsPas encore d'évaluation
- Neurotransmitter ChartDocument1 pageNeurotransmitter Chartmonster40lbs100% (2)
- Schizophrenia PowerpointDocument53 pagesSchizophrenia Powerpointmonster40lbsPas encore d'évaluation
- 9.00 Exam 3 Notes: Please Pardon Any Spelling Errors or Typos!Document9 pages9.00 Exam 3 Notes: Please Pardon Any Spelling Errors or Typos!monster40lbsPas encore d'évaluation
- By: Margaret Wise Brown Adapted By: Jessie Moreau, M.Ed., NBCTDocument18 pagesBy: Margaret Wise Brown Adapted By: Jessie Moreau, M.Ed., NBCTmonster40lbsPas encore d'évaluation
- Module3 - Psychology PowerpointDocument12 pagesModule3 - Psychology Powerpointmonster40lbsPas encore d'évaluation
- Understanding Psychology: The Biological Basis of BehaviorDocument79 pagesUnderstanding Psychology: The Biological Basis of Behaviormonster40lbsPas encore d'évaluation
- Cognition and Emotion: November 13-20, 2008Document90 pagesCognition and Emotion: November 13-20, 2008monster40lbsPas encore d'évaluation
- Learning Worksheet For 9 - 27Document2 pagesLearning Worksheet For 9 - 27monster40lbsPas encore d'évaluation
- Physiological Mechanism of RegulationDocument11 pagesPhysiological Mechanism of Regulationmonster40lbsPas encore d'évaluation
- Emotion RegulationDocument53 pagesEmotion Regulationmonster40lbs100% (1)
- Lecture 9 - Inductive and Deductive ReasoningDocument50 pagesLecture 9 - Inductive and Deductive Reasoningmonster40lbs0% (1)
- A Bitter EndingDocument15 pagesA Bitter Endingmonster40lbsPas encore d'évaluation
- Visual Attention PartDocument3 pagesVisual Attention Partmonster40lbsPas encore d'évaluation
- L Basic Neuroscience Lecture 13Document17 pagesL Basic Neuroscience Lecture 13monster40lbsPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Choral SpeakingDocument17 pagesChoral SpeakingAnithsia F. Kapitan100% (1)
- Bachelor Express Vs CA DigestDocument2 pagesBachelor Express Vs CA DigestKryzel V. LaurenaPas encore d'évaluation
- Regular Verbs - Vocabulary Word ListDocument6 pagesRegular Verbs - Vocabulary Word ListCeyhun Güler ☾☆Pas encore d'évaluation
- Risk Asessment For Coke DrumDocument17 pagesRisk Asessment For Coke DrumthawdarPas encore d'évaluation
- Chemical AwarenessDocument59 pagesChemical Awarenessbilo1984Pas encore d'évaluation
- Read The Situation Below and Fill in The Form That Follows.: Activity 2 (Accident/Incident Report)Document2 pagesRead The Situation Below and Fill in The Form That Follows.: Activity 2 (Accident/Incident Report)Husna IzzatiPas encore d'évaluation
- Design and Experimental Analysis of An Impact AttenuatorDocument5 pagesDesign and Experimental Analysis of An Impact AttenuatorSuryo HadiwibowoPas encore d'évaluation
- Psychiatric Injury Question 8 of 2019 Zone-B (Zone-A-N/A)Document4 pagesPsychiatric Injury Question 8 of 2019 Zone-B (Zone-A-N/A)Saydul ImranPas encore d'évaluation
- ISTAR Facilities (5e) (8887105)Document12 pagesISTAR Facilities (5e) (8887105)kerredaiPas encore d'évaluation
- Board Probles: Exercise - IiDocument4 pagesBoard Probles: Exercise - IithinkiitPas encore d'évaluation
- Achevara V RamosDocument6 pagesAchevara V RamosSecret SecretPas encore d'évaluation
- DGCA CAR On Cockpit Voice Recorders - D2I-I6 - SERIES 'I' PART VI-ISSUE II, 14th November 2012Document11 pagesDGCA CAR On Cockpit Voice Recorders - D2I-I6 - SERIES 'I' PART VI-ISSUE II, 14th November 2012james_008Pas encore d'évaluation
- Major Accidents Involving ContractorsDocument6 pagesMajor Accidents Involving ContractorsSt_LairPas encore d'évaluation
- Alits-6 Xii Apt 3 - Set-DDocument13 pagesAlits-6 Xii Apt 3 - Set-DYogesh GoyalPas encore d'évaluation
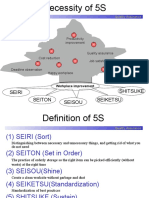
- Seiri Seiton Seiketsu Seisou ShitsukeDocument25 pagesSeiri Seiton Seiketsu Seisou ShitsukeSAmyPas encore d'évaluation
- Spec Pub 18-94 Improving Safety at Small Underground MinesDocument179 pagesSpec Pub 18-94 Improving Safety at Small Underground MinesRussell HartillPas encore d'évaluation
- 10.1.1.476.5960-Fsa Cruise ShipsDocument17 pages10.1.1.476.5960-Fsa Cruise ShipsJay Jay0% (1)
- Road Safety 2013 BergDocument45 pagesRoad Safety 2013 BergjoebriffaPas encore d'évaluation
- President Uhuru Kenyatta's Speech During The St. John Ambulance Priory Inauguration Ceremony at All Saints Cathedral, NairobiDocument3 pagesPresident Uhuru Kenyatta's Speech During The St. John Ambulance Priory Inauguration Ceremony at All Saints Cathedral, NairobiState House KenyaPas encore d'évaluation
- Alcock and BrownDocument9 pagesAlcock and BrownRowan Pritchard0% (1)
- Terminal Aerodrome Forecasts (Tafs) : Reading AssignmentDocument3 pagesTerminal Aerodrome Forecasts (Tafs) : Reading Assignmentintern_mike0% (1)
- Radiation PressureDocument19 pagesRadiation PressurebhishanPas encore d'évaluation
- Summary Tristram ShandyDocument2 pagesSummary Tristram ShandylsacnoattPas encore d'évaluation
- 04-Chapter 2 PDFDocument41 pages04-Chapter 2 PDFhymerchmidt100% (1)
- The Implications of The Accident at Three Mile Island - The New YorkerDocument3 pagesThe Implications of The Accident at Three Mile Island - The New YorkerEdmondsonPas encore d'évaluation
- Volvo 242 244 245 Owners Manual 1979Document120 pagesVolvo 242 244 245 Owners Manual 1979sander_kartPas encore d'évaluation
- Annonuevo Vs CADocument3 pagesAnnonuevo Vs CAClaudine BancifraPas encore d'évaluation
- WSH Awards 2018 Briefing (Auditors)Document58 pagesWSH Awards 2018 Briefing (Auditors)OnaFajardoPas encore d'évaluation
- Longford ExplosionDocument2 pagesLongford ExplosionZalu PrasetyoPas encore d'évaluation
- Present Perfect, Past and Past PerfectDocument4 pagesPresent Perfect, Past and Past PerfectBlanka MazuchPas encore d'évaluation