Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Cred PeruDocument2 pagesCred PeruJean Pierre Carrion ArcelaPas encore d'évaluation
- Akafala PrincessDocument1 pageAkafala PrincessJean Pierre Carrion ArcelaPas encore d'évaluation
- What Is The Problem?: Definition and ImpactDocument3 pagesWhat Is The Problem?: Definition and ImpactJean Pierre Carrion ArcelaPas encore d'évaluation
- Diseases of Water Metabolism SEMINARIO PDFDocument22 pagesDiseases of Water Metabolism SEMINARIO PDFAnonymous uVinWXfo4Pas encore d'évaluation
- Artralgias Secundarias A MetimazolDocument1 pageArtralgias Secundarias A MetimazolJean Pierre Carrion ArcelaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- PhenylDocument3 pagesPhenylVince PaelmoPas encore d'évaluation
- Non Ruminant DigestionDocument29 pagesNon Ruminant Digestionshivabt07Pas encore d'évaluation
- Full Feeding Cheat SheetDocument2 pagesFull Feeding Cheat SheethcoplanetPas encore d'évaluation
- NephrolithiasisDocument3 pagesNephrolithiasisVince GagarPas encore d'évaluation
- 2400 Calorie Nutrition Plan for Fat Loss & Muscle GainDocument5 pages2400 Calorie Nutrition Plan for Fat Loss & Muscle GainUtku Cantürk100% (1)
- Catalog Orlandos en HQ CDDocument20 pagesCatalog Orlandos en HQ CDGeorge PreoteasaPas encore d'évaluation
- Week 15 NutritionDocument33 pagesWeek 15 Nutritionrichard respetoPas encore d'évaluation
- Anthropometry 130824161551 Phpapp02Document48 pagesAnthropometry 130824161551 Phpapp02cuckoo1234Pas encore d'évaluation
- Manual 3Document17 pagesManual 3milagros vergaraPas encore d'évaluation
- Analisa Kandungan Gizi Dan Daya Terima Crackers Dengan Pemanfaatan Tepung Daun Kelor Dan Tepung Ikan LeleDocument8 pagesAnalisa Kandungan Gizi Dan Daya Terima Crackers Dengan Pemanfaatan Tepung Daun Kelor Dan Tepung Ikan LeleLupi PurniasihPas encore d'évaluation
- Buhler 2003-Vademecum For Vitamin FormulationsDocument144 pagesBuhler 2003-Vademecum For Vitamin FormulationsRok Kopinč100% (1)
- ADIME Note: Hypertension: AssessmentDocument2 pagesADIME Note: Hypertension: AssessmentJasperl Niña Malabuyoc100% (1)
- Gobbly Glook ReportDocument4 pagesGobbly Glook ReportTrang NguyenPas encore d'évaluation
- EV916 - E916 User Manual - EnglishDocument41 pagesEV916 - E916 User Manual - EnglishJeremyPas encore d'évaluation
- Glândulas Supra-Renais ou Adrenais: Função e RegulaçãoDocument37 pagesGlândulas Supra-Renais ou Adrenais: Função e RegulaçãoFilipe SilvaPas encore d'évaluation
- Causes, Symptoms and Tests for High Vitamin D LevelsDocument3 pagesCauses, Symptoms and Tests for High Vitamin D LevelsbhatambarekarPas encore d'évaluation
- The Keys to Progressive Resistance TrainingDocument8 pagesThe Keys to Progressive Resistance TrainingTomrules100% (1)
- Rda PDFDocument3 pagesRda PDFAnjali ReddyPas encore d'évaluation
- Management of Renal DiseasesDocument57 pagesManagement of Renal DiseasesAyana KeikoPas encore d'évaluation
- Nursing Care Plan (Bowel Elemination)Document8 pagesNursing Care Plan (Bowel Elemination)Rijane Tabonoc Omlang100% (1)
- Moribasa Ice Cream 1Document10 pagesMoribasa Ice Cream 1Glecy KimPas encore d'évaluation
- Analysis of Fruit and Vegetable JuicesDocument15 pagesAnalysis of Fruit and Vegetable JuicesTimothy DevaprasadPas encore d'évaluation
- Clearing Histamine - Ray Peat ForumDocument11 pagesClearing Histamine - Ray Peat ForumDarci HallPas encore d'évaluation
- The Transformation TenDocument28 pagesThe Transformation TenRob AtkinPas encore d'évaluation
- Fundamentals of NutritionDocument55 pagesFundamentals of NutritionIhsan BadshaPas encore d'évaluation
- Latent Autoimmune Diabetes in Adults (LADA)Document5 pagesLatent Autoimmune Diabetes in Adults (LADA)Fina Ahmad FitrianaPas encore d'évaluation
- Baseline Survey On Fruit and Vegetables Consumption Among SchoolDocument13 pagesBaseline Survey On Fruit and Vegetables Consumption Among Schoolmujuni brianmjuPas encore d'évaluation
- Final Project of MarketingDocument18 pagesFinal Project of MarketingshoaibmanglaPas encore d'évaluation
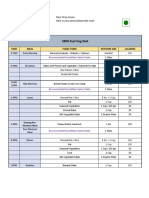
- 2800 Kcal Veg Diet: Time Meal Food Items Portion Size CaloriesDocument2 pages2800 Kcal Veg Diet: Time Meal Food Items Portion Size CaloriesSiraj AnsariPas encore d'évaluation
- Specific Test For Folate Deficiency AnemiaDocument5 pagesSpecific Test For Folate Deficiency AnemiaPremaKurniaPas encore d'évaluation