Vous aimerez peut-être aussi
- Pathophysiology Chapter 21Document12 pagesPathophysiology Chapter 21Christina100% (6)
- ATI Ebook - Med SurgDocument702 pagesATI Ebook - Med SurgMichelle Villanueva100% (4)
- BloodDocument103 pagesBloodrizwanbas50% (2)
- Urinary SystemDocument99 pagesUrinary SystemHarshika KDGPas encore d'évaluation
- Anatomy and Physiology of The KidneysDocument3 pagesAnatomy and Physiology of The KidneysNeil AlviarPas encore d'évaluation
- Liver and Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Updated TreatmentsD'EverandLiver and Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Updated TreatmentsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Bile Salt & Enterohepatic CirculationDocument27 pagesBile Salt & Enterohepatic Circulationammu 94Pas encore d'évaluation
- Liver, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandLiver, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÉvaluation : 3 sur 5 étoiles3/5 (1)
- RenalSystem Part 1 (Spring2020)Document49 pagesRenalSystem Part 1 (Spring2020)Sahil ParikhPas encore d'évaluation
- PhysioEx Exercise 9 Activity 2Document3 pagesPhysioEx Exercise 9 Activity 2PatriPas encore d'évaluation
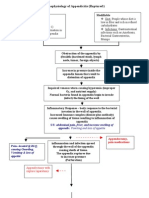
- Pathophysiology of Appendicitis (Ruptured)Document2 pagesPathophysiology of Appendicitis (Ruptured)paul andrew laranjo asuncion100% (2)
- Pathophysiology of Appendicitis (Ruptured)Document2 pagesPathophysiology of Appendicitis (Ruptured)paul andrew laranjo asuncion100% (2)
- Activity 4 Dialysis - Anna Philomena B. FerrerDocument5 pagesActivity 4 Dialysis - Anna Philomena B. FerrerSebs BerebsPas encore d'évaluation
- (Biology) The LiverDocument7 pages(Biology) The LiverNiharikaPas encore d'évaluation
- 1 BloodDocument77 pages1 BloodVisaNathan100% (1)
- Science Stage 9 02 9RP AFP tcm143-639993Document17 pagesScience Stage 9 02 9RP AFP tcm143-639993mal100% (1)
- DLL Science Quarter 2 Week 1-9Document24 pagesDLL Science Quarter 2 Week 1-9Argie PiaPas encore d'évaluation
- Urinalysis and Body Fluids 6th Edition by Susan King Strasinger - Test BankDocument45 pagesUrinalysis and Body Fluids 6th Edition by Susan King Strasinger - Test Bankroseyoung0Pas encore d'évaluation
- Interpretations of Test Results in Routine Urine AnalysisDocument2 pagesInterpretations of Test Results in Routine Urine AnalysisDevaughn Ray PacialPas encore d'évaluation
- Liver: Anatomy & FunctionsDocument18 pagesLiver: Anatomy & FunctionsDR NARENDRAPas encore d'évaluation
- Analysis of UrineDocument22 pagesAnalysis of UrineFaith Domingo100% (1)
- LiverDocument15 pagesLiverNyakie MotlalanePas encore d'évaluation
- Liver, Bile and Pancreatic Physiology PDFDocument78 pagesLiver, Bile and Pancreatic Physiology PDFAdvin BurkePas encore d'évaluation
- Liver & G.bladder55Document41 pagesLiver & G.bladder55Sourin GoswamiPas encore d'évaluation
- Fisiologi Hati Dan Kandung EmpeduDocument37 pagesFisiologi Hati Dan Kandung EmpeduIlham PrayogoPas encore d'évaluation
- IB Biology D.3 Liver NotesDocument7 pagesIB Biology D.3 Liver NotesDilip Pandurang PattilPas encore d'évaluation
- Cpy 531 Lecture Note 1Document20 pagesCpy 531 Lecture Note 1onyibor joshuaPas encore d'évaluation
- Chapter 12 - ExcretionDocument51 pagesChapter 12 - ExcretionKareem DmourPas encore d'évaluation
- Hepatogastroenterologi PK PrintDocument68 pagesHepatogastroenterologi PK Printvita_aprilinaPas encore d'évaluation
- Chapter 84, Physiology of LiverDocument49 pagesChapter 84, Physiology of LiverSangita MPas encore d'évaluation
- Taught To Nursing Students of RmuDocument42 pagesTaught To Nursing Students of RmumunshiPas encore d'évaluation
- LiverDocument18 pagesLiverAbhirami BabuPas encore d'évaluation
- CVS BloodDocument39 pagesCVS BloodMohan GuptaPas encore d'évaluation
- Geb203 AssignmentDocument11 pagesGeb203 AssignmentAysha Siddika MimPas encore d'évaluation
- GruczołyDocument33 pagesGruczołynatalie muyengwaPas encore d'évaluation
- Fisio + Jaundice GabunganDocument52 pagesFisio + Jaundice GabunganMufti DewantaraPas encore d'évaluation
- 1 RENAL Glomerular Nephrotic2016Document45 pages1 RENAL Glomerular Nephrotic2016Crystal Lynn Keener SciariniPas encore d'évaluation
- Department of Kriyasharir: Mahatma Gandhi Ayurved College Hospital & Research Centre Salod (H), WardhaDocument39 pagesDepartment of Kriyasharir: Mahatma Gandhi Ayurved College Hospital & Research Centre Salod (H), WardhaAvanti ShendurjanePas encore d'évaluation
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonPas encore d'évaluation
- Class 10 Biology Chapter 8 Revision NotesDocument5 pagesClass 10 Biology Chapter 8 Revision NotesOm KapoorPas encore d'évaluation
- Option D - Unit 3 - Liver FunctionsDocument26 pagesOption D - Unit 3 - Liver Functionsjanafahmy1211Pas encore d'évaluation
- Gastrointestinal Anatomy and Physiology: Part 4: Liver, Pancreas and Gall BladderDocument38 pagesGastrointestinal Anatomy and Physiology: Part 4: Liver, Pancreas and Gall BladderSar PattsPas encore d'évaluation
- Liver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenDocument79 pagesLiver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenIrish Nicole DCPas encore d'évaluation
- Water-Salt Metabolism in The Body: Intracellular Fluid CompositionDocument6 pagesWater-Salt Metabolism in The Body: Intracellular Fluid CompositionFranklyn Favour FlorencePas encore d'évaluation
- 11 Human Physiology Urinary SystemDocument59 pages11 Human Physiology Urinary SystemsuPas encore d'évaluation
- Blood and Blood ComponentsDocument19 pagesBlood and Blood ComponentsMiljun CatacataPas encore d'évaluation
- Lec5 PDFDocument71 pagesLec5 PDFNaba NabeelPas encore d'évaluation
- Liver and Biliary System: DR Anil Chaudhary Associate Professor PhysiologyDocument31 pagesLiver and Biliary System: DR Anil Chaudhary Associate Professor Physiologylion2chPas encore d'évaluation
- Al Wadi International School Biology Grade 9 13. Excretion in Humans NotesDocument42 pagesAl Wadi International School Biology Grade 9 13. Excretion in Humans NotesMohammed HelmyPas encore d'évaluation
- Excretory SystemDocument61 pagesExcretory Systemalayca cabatanaPas encore d'évaluation
- Kidney SystemDocument21 pagesKidney SystemMuntasirPas encore d'évaluation
- Excretory System-IDocument29 pagesExcretory System-IAkash KumarPas encore d'évaluation
- Chapter 11 - ExcretionDocument46 pagesChapter 11 - Excretionapi-372850875% (4)
- Liver AnaphyDocument4 pagesLiver AnaphyEleazar BelgicaPas encore d'évaluation
- Lecture 4 Excretory SystemDocument18 pagesLecture 4 Excretory Systembabaaijaz01Pas encore d'évaluation
- Function of Liver in Human Body: Liver Physiology, Larry Frolich, Yavapai College, March 10, 2006Document16 pagesFunction of Liver in Human Body: Liver Physiology, Larry Frolich, Yavapai College, March 10, 2006alikhanbalouchPas encore d'évaluation
- Biochemistry: Dr. Dra. Trini Suryowati, MsDocument49 pagesBiochemistry: Dr. Dra. Trini Suryowati, MsDaud ParluhutanPas encore d'évaluation
- Excretory ProductsDocument8 pagesExcretory ProductsmatinPas encore d'évaluation
- Notes Grade: IX Subject: Biology Unit: 12 Topic: Excretion ObjectivesDocument21 pagesNotes Grade: IX Subject: Biology Unit: 12 Topic: Excretion Objectivespraneeth satishPas encore d'évaluation
- Lecture 19-Nutrients Renal Functions-Dr. Dr. Sri Lestari S. R., M.SC (2022)Document38 pagesLecture 19-Nutrients Renal Functions-Dr. Dr. Sri Lestari S. R., M.SC (2022)artha maressaPas encore d'évaluation
- Hepatitis - Case StudyDocument8 pagesHepatitis - Case Studynight24rushPas encore d'évaluation
- 3 Liver Cell AllDocument101 pages3 Liver Cell AllIntanNirmalaPas encore d'évaluation
- Fluid, Electrolytes and Diuretics 2020Document33 pagesFluid, Electrolytes and Diuretics 2020Tasya FakhiraPas encore d'évaluation
- BloodDocument21 pagesBloodRalph Rezin MoorePas encore d'évaluation
- UNIT 10 Excretion in Humans NotesDocument27 pagesUNIT 10 Excretion in Humans NotescyumadripPas encore d'évaluation
- Urinary SystemDocument40 pagesUrinary SystemAlyssa AlferezPas encore d'évaluation
- Normal Liver PhysiologyDocument3 pagesNormal Liver PhysiologymarinelleeslabonPas encore d'évaluation
- Major IntracelularDocument67 pagesMajor Intracelularfarooq shah shabbirPas encore d'évaluation
- Grade 11 Excretion & Homeostasis - Class 1Document33 pagesGrade 11 Excretion & Homeostasis - Class 1Tonique Gordon100% (1)
- Liver, Bile, & Pancreatic Physiology PDFDocument6 pagesLiver, Bile, & Pancreatic Physiology PDFAdvin BurkePas encore d'évaluation
- ProductionDocument2 pagesProductionad-adPas encore d'évaluation
- Pre Labor VsDocument14 pagesPre Labor Vsad-adPas encore d'évaluation
- Please Print AsapDocument22 pagesPlease Print Asapad-adPas encore d'évaluation
- NCP 1Document1 pageNCP 1hsiriaPas encore d'évaluation
- The HemophiliasDocument3 pagesThe HemophiliasVytheeshwaran Vedagiri100% (3)
- NCP 1Document1 pageNCP 1hsiriaPas encore d'évaluation
- Pharmacology IntroductionDocument2 pagesPharmacology Introductionad-adPas encore d'évaluation
- Insertion Nasogastric Tube: Catheterizing The Female & Male Urinary Bladder (Straight & Indwelling)Document4 pagesInsertion Nasogastric Tube: Catheterizing The Female & Male Urinary Bladder (Straight & Indwelling)ad-adPas encore d'évaluation
- DR Arzoo Nephrology ThesesDocument35 pagesDR Arzoo Nephrology ThesesAzam ArzooPas encore d'évaluation
- Costing Ranap Jan-JunDocument32 pagesCosting Ranap Jan-Jungalih wicaksonoPas encore d'évaluation
- Rudaina Alelyani MEV Assignment3.Document15 pagesRudaina Alelyani MEV Assignment3.Rudaina AlelyaniPas encore d'évaluation
- Urology IDocument34 pagesUrology IEbraheam HadiPas encore d'évaluation
- Apogee 5500 Data Sheet V20190301-ADocument18 pagesApogee 5500 Data Sheet V20190301-AIBrahim FayedPas encore d'évaluation
- 0Document2 pages0Dylan WhitePas encore d'évaluation
- Proteinuria and Chronic Kidney DiseaseDocument34 pagesProteinuria and Chronic Kidney DiseaseВалерий ГаврилуцаPas encore d'évaluation
- Chapter 1-4Document11 pagesChapter 1-4Vy ThachPas encore d'évaluation
- Anaplastic Sarcoma of The Kidney With Chromosomal AbnormalityDocument5 pagesAnaplastic Sarcoma of The Kidney With Chromosomal AbnormalityJose Alejandro InciongPas encore d'évaluation
- Summer Vacation Assignment - QuestionsDocument7 pagesSummer Vacation Assignment - QuestionsSidra QueenPas encore d'évaluation
- Anatomi GenitourinariaDocument30 pagesAnatomi Genitourinariamelya susantiPas encore d'évaluation
- Yoshio Terada Takashi Wada Kent Doi Acute Kidney Injury and Regenerative Medicine Springer Singapore Springer 2020Document390 pagesYoshio Terada Takashi Wada Kent Doi Acute Kidney Injury and Regenerative Medicine Springer Singapore Springer 2020XtinePas encore d'évaluation
- UremiaDocument4 pagesUremiaMilnalyn Muammil100% (1)
- Soal Seleksi Impsq Tahap 1Document3 pagesSoal Seleksi Impsq Tahap 1sanjayahalim123Pas encore d'évaluation
- NPNS QuizDocument2 pagesNPNS QuizAshley TañamorPas encore d'évaluation
- Diabetes Related CKD 2Document1 pageDiabetes Related CKD 2Jia-PeiWuPas encore d'évaluation
- Manuscript 3DRFDocument13 pagesManuscript 3DRFMattia TronconePas encore d'évaluation
- Types of Renal Disease in Avian Species: Robert E. Schmidt, DVM, PHD, DabvpDocument10 pagesTypes of Renal Disease in Avian Species: Robert E. Schmidt, DVM, PHD, DabvpjudithPas encore d'évaluation
- Edexcel A-LEVEL BIO5 January 2007 QPDocument20 pagesEdexcel A-LEVEL BIO5 January 2007 QPapi-3726022Pas encore d'évaluation
- Adaptasi Fisiologis Selama PuasaDocument9 pagesAdaptasi Fisiologis Selama PuasaCanva IdPas encore d'évaluation
- Padhle 10th - Life ProcessesDocument74 pagesPadhle 10th - Life ProcessesBhumik HingvePas encore d'évaluation
- Biology 5090 12 Paper 1 Question Paper Mayjue 2013Document16 pagesBiology 5090 12 Paper 1 Question Paper Mayjue 2013Raja Muda Raja NgahPas encore d'évaluation