Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Drug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaiseDocument3 pagesDrug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaisekristel_nicole18yahoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
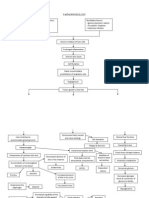
- Diagram I Pathogenesis of Insulin Dependent DM (Type 1) : DiagramsDocument2 pagesDiagram I Pathogenesis of Insulin Dependent DM (Type 1) : Diagramskristel_nicole18yahoPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Middle Adulthood (40 To 65 Years)Document1 pageMiddle Adulthood (40 To 65 Years)kristel_nicole18yahoPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Monday, Tuesday, Thursday & Friday: St. Pio of Pietrelcina ChapelDocument2 pagesMonday, Tuesday, Thursday & Friday: St. Pio of Pietrelcina Chapelkristel_nicole18yahoPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Chemistry Date: 04/29/14: Developed or Changed The Ranges From Her Chemistry LabDocument1 pageChemistry Date: 04/29/14: Developed or Changed The Ranges From Her Chemistry Labkristel_nicole18yahoPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Nursing Care Process: University of The East Ramon MagsaysayDocument5 pagesNursing Care Process: University of The East Ramon Magsaysaykristel_nicole18yahoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Assessment Diagnosis Rationale Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Implementation Rationale Evaluationkristel_nicole18yahoPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- 3rd NCP Risk For ConstipationDocument2 pages3rd NCP Risk For Constipationkristel_nicole18yaho100% (3)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hinds & Gattuso, 1999Document1 pageHinds & Gattuso, 1999kristel_nicole18yahoPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Clinical Teaching Behavior Student'S Learning Response: Conceptual FrameworkDocument5 pagesClinical Teaching Behavior Student'S Learning Response: Conceptual Frameworkkristel_nicole18yahoPas encore d'évaluation
- Pathophysiology of Spinal Cord Injury 1Document1 pagePathophysiology of Spinal Cord Injury 1kristel_nicole18yaho60% (5)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Assessment Diagnosis Rationale Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Implementation Rationale Evaluationkristel_nicole18yahoPas encore d'évaluation
- Predisposing Factors Precipitating FactorsDocument1 pagePredisposing Factors Precipitating Factorskristel_nicole18yahoPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Past Health History Medward3Document1 pagePast Health History Medward3kristel_nicole18yahoPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Evidence-Based Practice: Acute Upper Gastrointestinal Bleeding: ManagementDocument3 pagesEvidence-Based Practice: Acute Upper Gastrointestinal Bleeding: Managementkristel_nicole18yahoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Family Nursing Care Plan. 1st and 2nd Level AssessmentDocument7 pagesFamily Nursing Care Plan. 1st and 2nd Level Assessmentkristel_nicole18yaho100% (1)
- Childlessness Is Defined As The Condition of Being Without ChildrenDocument2 pagesChildlessness Is Defined As The Condition of Being Without Childrenkristel_nicole18yahoPas encore d'évaluation
- Case Study: Post-Cesarian Section: University of The EastDocument3 pagesCase Study: Post-Cesarian Section: University of The Eastkristel_nicole18yahoPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- PathophysiologyDocument2 pagesPathophysiologykristel_nicole18yahoPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Mobile Health Clinic InitiativeDocument47 pagesMobile Health Clinic InitiativededdyPas encore d'évaluation
- h2s Hand BookDocument34 pagesh2s Hand BookJorge Eliecer Ferro Cotes100% (4)
- Material Safety Data Sheet: Liquefied Petroleum GasDocument1 pageMaterial Safety Data Sheet: Liquefied Petroleum GasardhanhendroPas encore d'évaluation
- Activity 1: Write Your Answer On The Space ProvidedDocument4 pagesActivity 1: Write Your Answer On The Space ProvidedEki OmallaoPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Nov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Document79 pagesNov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Jean Gwyneth GatchalianPas encore d'évaluation
- Jurnal ParuDocument31 pagesJurnal Parudr. syah sembung wasisoPas encore d'évaluation
- Qand ADocument5 pagesQand AJoshua PascasioPas encore d'évaluation
- Araldite - GT7074Document2 pagesAraldite - GT7074maz234Pas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- 7 Contoh Analytical Exposition Pendek Bahasa InggrisDocument6 pages7 Contoh Analytical Exposition Pendek Bahasa InggrisDarsi YujiwatiPas encore d'évaluation
- Medicine Supplies & First Aid Treatment LogsheetDocument4 pagesMedicine Supplies & First Aid Treatment LogsheetMark BuendiaPas encore d'évaluation
- Final Stock ReportDocument63 pagesFinal Stock ReportKarthik SunnyPas encore d'évaluation
- Adoption LawsDocument10 pagesAdoption LawsAneesh PandeyPas encore d'évaluation
- Definition of Physical EducationDocument7 pagesDefinition of Physical EducationRose Jane BangisPas encore d'évaluation
- Synopsis - Anu Varghese and Dr. M H Salim, 2015 - Handloom Industry in Kerala A Study of The Problems and ChallengesDocument8 pagesSynopsis - Anu Varghese and Dr. M H Salim, 2015 - Handloom Industry in Kerala A Study of The Problems and ChallengesNandhini IshvariyaPas encore d'évaluation
- PNF 8th EditionDocument7 pagesPNF 8th EditionDanisaWajePas encore d'évaluation
- MSDS Phthalic AnhydrideDocument6 pagesMSDS Phthalic AnhydrideBansi TumbadiaPas encore d'évaluation
- SAFed Tests PDFDocument88 pagesSAFed Tests PDFDanPas encore d'évaluation
- Rules Related Statutes All CodesDocument150 pagesRules Related Statutes All CodesRod SatrePas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Sex Should Be Taught in Schools: Shafira Anindya Maharani X IPS 1 /29Document11 pagesSex Should Be Taught in Schools: Shafira Anindya Maharani X IPS 1 /29Shafira Anindya MaharaniPas encore d'évaluation
- MSDS Baybl T65 901510Document8 pagesMSDS Baybl T65 901510gnavarroPas encore d'évaluation
- A Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125Document9 pagesA Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125PREJA PATELPas encore d'évaluation
- HEALTH-TEACHING-PLAN sUGATON EVALDocument9 pagesHEALTH-TEACHING-PLAN sUGATON EVALPrincess Faniega SugatonPas encore d'évaluation
- 04fc75de986c12 Pharmaceutics-I AROMATIC WATERSDocument14 pages04fc75de986c12 Pharmaceutics-I AROMATIC WATERSsultanPas encore d'évaluation
- Vieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMDocument17 pagesVieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMFranciscoPas encore d'évaluation
- Activity 2: General Biology 2 (Quarter IV-Week 3)Document4 pagesActivity 2: General Biology 2 (Quarter IV-Week 3)KatsumiJ AkiPas encore d'évaluation
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127Pas encore d'évaluation
- Body GuideDocument46 pagesBody GuideBárbara Leite95% (22)
- Corpus Alienum PneumothoraxDocument3 pagesCorpus Alienum PneumothoraxPratita Jati PermatasariPas encore d'évaluation
- Pelvic Fracture Case StudyDocument48 pagesPelvic Fracture Case StudyYves BasanPas encore d'évaluation
- Tsoukaki 2012Document8 pagesTsoukaki 2012Marina JoelPas encore d'évaluation
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)D'EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Évaluation : 3 sur 5 étoiles3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 4.5 sur 5 étoiles4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (32)