Article
Arq Neuropsiquiatr 2010;68(2):242-245
Temperature variation in the 24 hours before the initial symptoms of stroke
Fernando Morgadinho Santos Coelho1, Bento Fortunato Cardoso dos Santos1, Miguel Cendoroglo Neto1, Luis Fernando Lisboa1, Adriana Serra Cypriano1, Tania Oliveira Lopes1, Marina Jorge de Miranda2, Ana Maria H. vila2, Jonas Bordin Alonso2, Hilton Siqueira Pinto2
Abstract A few studies have performed to evaluate the temperature variation influences over on the stroke rates in Brazil. Method: 176 medical records of inpatients were analyzed after having had a stroke between 2004 and 2006 at Hospital Israelita Albert Einstein. The temperature preceding the occurrence of the symptoms was recorded, as well as the temperature 6, 12 and 24 hours before the symptoms in 6 different weather substations, closest to their houses in So Paulo. Results: Strokes occurred more frequently after a variation of 3C between 6 and 24 hours before the symptoms. There were most hospitalizations between 23-24C. Conclusion: Incidence of stroke on these patients was increased after a variation of 3 Celsius within 24 hours before the ictus. The temperature variations could be an important factor in the occurrence of strokes in this population. Key words: stroke, temperature, cardiovascular risk, seasonal. Variao da temperatura nas 24 horas anteriores aos sintomas iniciais do acidente vascular cerebral Resumo Poucos trabalhos tm estudado a variao sazonal e de temperatura em acidente vascular cerebral (AVC) no Brasil. Mtodo: Foram analisados 176 registros de pacientes com AVC no Hospital Israelita Albert Einstein entre 2004 e 2006. Foram anotadas as temperaturas ambientes do incio dos sintomas, bem como as temperaturas de 6, 12 e 24 horas antes dos sintomas, em 6 diferentes subestaes metereolgicas mais prximas da casa do paciente em So Paulo. Resultados: Houve aumento da incidncia do AVC com a variao de 3C entre 6 e 24 horas antes do incio dos sintomas. Houve um pico de internao entre 2324C. Concluso: A variao de temperatura de 3C nas 24 horas que antecederam o incio dos sintomas pode ter sido um fator importante na ocorrncia do AVC. Palavras-chave: acidente vascular cerebral, temperatura, risco cardiovascular, sazonal. The correlation between strokes and seasonal variations have been studied in various places1-8. Some studies around the world have reported an increase of incidence, mortality, and stroke hospitalization during the coldest months of winter. The authors suggest that the temperature variations may trigger responses of vasoconstriction with increase in cardiovascular events. However, the understanding
1
Correspondence Fernando Morgadinho Santos Coelho Avenida Albert Einstein 677 1 SS - Prtica Mdica 05651-901 So Paulo SP - Brasil E-mail: fernandomorgadinho@hotmail.com or fmscoelho@einstein.br Received 1 August 2009 Received in final form 22 October 2009 Accepted 3 November 2009 242
of the relation between changes of weather and cardiovascular events is limited9-13. The variation of temperatures before the occurrence of ictus has not been frequently observed. The change in temperature before a stroke could has play a more important role than the season it self. Authors show that the incidence of hemorrhagic stroke (HS) was higher on those days during which the temperature varied significantly12.
Hospital Israelita Albert Einstein, So Paulo SP, Brazil; 2UNICAMP, Campinas SP, Brazil.
Arq Neuropsiquiatr 2010;68(2)
Stroke temperature variations Coelho et al.
A few studies have been performed to evaluate seasonal and temperature variation in the Southern Hemisphere13,14. Since Brazil is a tropical country, we believe that the seasons have less influence on the incidence of cerebral vascular disease than thermal changes. It is known that the seasons in tropical countries are not as distinctive as in the temperate climate countries. Therefore, it becomes difficult to compare the influence of the environmental aspects on different parts of the world14. The effects of the temperature variation on risk factors in stroke incidence have not been easily shown. Especially in a great metropolitan area as Sao Paulo, there is a substantial heterogeneity of temperature depending on the part of the city. This piece information stresses the importance of checking the local temperatures depending on which part of the city each patient lives or works. The goal of this study is to describe the temperature variation during the 24 hours before the occurrence of the stroke such the measurement was recorded by weather substations in the city, depending on their proximity to the patients location. The purpose of this study is to analyze the temperature variation during the 24 hours before the beginning of symptoms of stroke on the inpatients at Hospital Albert Einstein between August 2004 and December 2006. Method This is a retrospective study that has used data from the medical records of inpatients with stroke, admitted to the Hospital Israelita Albert Einstein. All patients were monitored by the stroke protocol between August 2004 and December 2006. The study was approved by Hospitals Ethics Committee under number 411-08.
Since July 2004 Hospital Israelita Albert Einstein has haven a stroke team. (Joint Commission Certificated Stroke Center 2007 May). A total of 176 medical records of inpatients have been reviewed with cerebral vascular disease. The patients were separated into groups according to the aetiology of the ischemic stroke (149 patients) or hemorrhagic stroke (27 patients). Patients with ischemic strokes were subdivided in thrombotic stroke (101 patients) and embolic stroke (48 patients) according to TOAST criteria. Inclusion criteria All patients between 50 and 80 years old who had acute stroke confirmed. Exclusion criteria: All patients younger than 50 years old and older than 80 years old and whose symptoms began while sleeping. The temperature at the beginning of the symptoms on the date of hospitalisation was noted, as well as the temperature 6, 12 and 24 hours before the initial symptoms in 6 different weather substations in the city, depending on their proximity to the patients address by team of CEPAGRI (Centre for Weather and Climate Research). Continuous variable data were expressed as number of hospitalizations (n) mean value, standard deviation (STD Dev) median, lower quartile (Q1), upper quartile (Q3), minimum and maximum values. Categorical variables were expressed as frequency. The number of inpatients was presented after applying the Poisson random variables, where each hospitalisation was assumed to be a function of temperature, year and month. The Generalized Additive Model (GAM) was used to fit both a reduced categorical model and a nonparametric spline model.
Table. Number of hospitalizations of patients with stroke. Thrombotic Month Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 3 6 3 13 3 48 40 5 1 11 11 3 8 1 6 10 1 3 2004 2005 1 5 7 6 6 2006 6 3 5 2 6 3 6 4 3 2 2 3 1 2 2 2 3 2 1 1 3 1 1 1 1 16 24 2 3 1 4 1 4 2004 Haemorrhagic 2005 2006 2004 Embolic 2005 3 1 1 3 2006 2 2 9 4 2 2 1 Total 12 11 29 17 18 8 17 18 14 14 7 11 176
243
Stroke temperature variations Coelho et al.
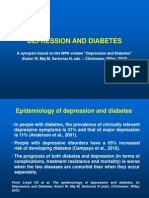
25 20 15 10 5 0
Arq Neuropsiquiatr 2010;68(2)
n 144.00 Mean 22.527 StD 4.446
12.5
15
17.5
20
22.5
25
27.5
30
32.5
Temperature at the beginning of the symptoms (BOS) - Celsius Degree
Figure. Histogram of temperature at the beginning of symptoms before the beginning of symptoms.
Results There were no differences in the numbers of hospitalisations among types of stroke after analysis of the seasonal factors. There was an increase of stroke inpatients in March (Summer-Autumn) (Table). The numbers of hospitalisations were low bellow the temperature of 20C, increasing until it reached a maximum between 23-24C, and decreasing again. The hospitalisations after ischemic and haemorrhagic strokes were more frequent at an average temperature that is more prevalent temperature at So Paulo (22.524.44C) (Figure). Discussion The highest prevalence of cerebral vascular disease hospitalisations occurred in March, a period that corresponds to the end of Summer in Brazil. This data differs from other studies that show a higher predominance of cerebral vascular disease during the Winter. Our study demonstrates that the variation of 3C, measured close to the patients address, during 24 hours before the occurrence of a stroke was an important factor for these patients in So Paulo. There was an increase in the hospitalization of patients with stroke between 23-24C, which is the range most common temperature of the city. However, the differences between environmental and room temperature exposition could be a bias for our study. On the other hand, the association among daily variation of temperature in the environment, pollution and cardiovascular mortality has been demonstrated in epidemiological studies15-18. An interesting study found out some factors that have increased the cardiovascular risk, such as the variation of environmental temperature, drier air, upper respiratory infections, grass pollen, SO2, and particulate air pollution19. It is known that the variation of temperature plays an
244
important role in risk factors of cardiovascular diseases, such as respiratory infections, concentration of particulate air and agglomeration of people with a high possibility of having had contact with the influenza virus, for example. Likewise, another interesting study has shown that a decrease in air temperature over a few days is associated with an increase among C-reactive protein, interleukin-6, and fibrinogen with increased cardiovascular risk20. Previous studies carried out in England have analyzed the variation of temperature before the occurrence of a stroke and it noted five days between the decreased in temperature and the incidence of the stroke21-23. The new and interesting finding of our study is that almost all of our patients started to show the symptoms during a comfortable range of temperature (23-24C) after a variation of 3C. In this way, a new study has reported that the daily average of HS for the group aged <65 increased by 15% and 12% for a 1C increase in daily maximum temperature and minimum temperature in the Summer and that the daily average of IS for the group aged 65 decreased by 3% for a 1C increase in daily maximum temperature in the Winter, after the adjustment of confounding factors13. Such study has not analyzed in detail the 24 hours prior to the event and the authors didnt use the temperature that was closest to the patients location. Unfortunately, the general analysis of the temperature variation can contain mistakes. The bottom line is that temperature variations were an important factor for the occurrence of Stroke and that the events were more frequent after the normalization of the local temperature during the 24 hours before it occurred.
acknowledgments We thank the patients and staff members
Percent
Reynaldo Brandt, Eliova Zukerman, Pedro Paulo Porto, Paulo Hlio Monzillo, Pedro Camilo de Almeida Pimentel, Roberto Naun Morgulis and Alexandre Pieri for neurological support.
1. Wang Y, Levi CR, Attia JR, et al. Seasonal variation in stroke in the Hunter Region. Australia A 5-year hospital-based study, 1995-2000. Stroke 2003;34: 1144-1150. 2. Laaidi K, Minier D,Osseby GV, et al. Seasonal variation in strokes incidence and the influence of the meteorological conditions. Rev Neurol 2004;160:321-330. 3. Anlar O, Tombul T, Unal O, Kayan M. Seasonal and environmental temperature variation in the occurrence of ischemic strokes and intracerebral hemorrhages in a Turkish adult population. Int J Neurosci 2002;112:959-963. 4. Shinkawa A, Ueda K, Hasuo Y, Kiyohara Y, Fujishima M. Seasonal variation in stroke incidence in Hisayama, Japan. Stroke 1990;21:1262-1267. 5. Sobel E, Zhang ZX, Alter M, et al. Stroke in the Lehigh Valley: seasonal variation in incidence rates. Stroke 1987;18:38-42. 6. Piver WT, Ando M, Ye F, Portier CJ. Temperature and air pollution as risk factors for heat stroke in Tokyo, July and August 1980-1995. Environ Health Perspect 1999;107:11-16. 7. Oberg AL, Ferguson JA, McIntyre LM, Horner RD. Incidence of stroke and season of the year: evidence of an association. Am J Epidemiol 2000;152:558-564. 8. Field TS, Green TL, Roy K, Pedersen J, Hill MD. Trends in hospital admission for stroke in Calgary. Can J Neurol Sci 2004;31:387-393.
References
Arq Neuropsiquiatr 2010;68(2)
9. Khan IA, Joy KP. Seasonal and daily variations in hypothalamic monoamine levels and monoamine oxidase activity in the Teleost Channa Punctatus (Bloch). Chronobiol Int 1988;5:311-316. 10. Baumgartl H,Heinrich U,Lubbers DW. Oxygen supply of the blood-free perfused guinea-pig brain in normo- and hypothermia measured by the local distribution of oxygen pressure. Pflugers Arch 1989;414:228-234. 11. Leppaluoto J, Paakkonen T, Korhonen I,Hassi J. Pituitary and autonomic responses to cold exposures in man. Acta Physiol Scand 2005;184:255-264. 12. Ohwaki K, Yano E, Murakami H, Nagashima H, Nakagomi T. Meteorological factors and the onset of hypertensive intracerebral hemorrhage. Int J Biometeorol 2004;49:86-90. 13. Wang XY, Barnett AG, Hu W, Tong S. Temperature variation and emergency hospital admiss for stroke in Brisbane, Australia, 1996-2005. Int J Biometeorol 2009 [Epub ahead of print]. 14. Alonso WJ, Viboud C, Simonsen L, et al. Seasonality of Influenza in Brazil: a traveling wave from the Amazon to the Subtropics. Am J Epidemiol 2007;165:1434-1442. 15. Ostro B, Chestnut L, Vichit-Vadakan N, Laixuthai A. The impact of particulate matter on daily mortality in Bangkok, Thailand. J Air Waste Manag Assoc 1999;49:100-107. 16. Samet JM, Dominici F, Curriero FC, Coursac I, Zeger SL. Fine particulate air pollution and mortality in 20 US cities, 1987-1994. N Engl J Med 2000;343:1742-1749.
Stroke temperature variations Coelho et al.
17. Katsouyanni K, Touloumi G, Samoli E, et al. Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology 2001; 12:521-531. 18. Pope A. Epidemiology of fine particulate air pollution and human health: biologic mechanisms and whos at risk? Environ Health Erspect 2000; 108(Suppl 4): S713-S724. 19. Low RB, Bielory L, Qureshi AI, et al. The relation of stroke admissions to recent weather, airborne allergens, air pollution, seasons, upper respiratory infections, and asthma incidence, September 11, 2001, and Day of the Week. Stroke 2006;37:951-957. 20. Schneider A, Panagiotakos D, Picciotto S, et al AIRGENE Study Group. Air temperature and inflammatory responses in myocardial infarction survivors. Epidemiology 2008;19:391-400. 21. Donaldson GC, Keatinge WR. Mortality related to cold weather in elderly people in southeast England, 1979-94. BMJ 1997;315:1055-1056. 22. Kyobutungi C, Grau A, Stieglbauer G, Becher H. Absolute temperature, temperature changes and stroke risk: a case-crossover study. Eur J Epidemiol 2005;20:693-698. 23. Yun-Chul H, Joung-Ho R, Jong-Tae L, Eun-Hee H, Ho-Jang K, Ho K. Ischemic stroke associated with decrease in temperature. Epidemiology 2003;14: 473-478.
245
Vous aimerez peut-être aussi
- 44 1019eDocument7 pages44 1019ePrya ChairullahPas encore d'évaluation
- Pass 12345Document1 pagePass 12345Prya ChairullahPas encore d'évaluation
- Pengantar Ebm KKDocument17 pagesPengantar Ebm KKPrya ChairullahPas encore d'évaluation
- Buku Bedah UmumDocument126 pagesBuku Bedah UmumSilvia Kamal100% (7)
- Front PsychiatryDocument4 pagesFront PsychiatryPrya ChairullahPas encore d'évaluation
- Buku Bedah UmumDocument7 pagesBuku Bedah UmumPrya ChairullahPas encore d'évaluation
- Schizophrenia: From Neurophysiological Abnormalities To Clinical SymptomsDocument6 pagesSchizophrenia: From Neurophysiological Abnormalities To Clinical SymptomsPrya ChairullahPas encore d'évaluation
- IuihuidyejkdDocument1 pageIuihuidyejkdPrya ChairullahPas encore d'évaluation
- Dopamine and Sleep From S&HDocument13 pagesDopamine and Sleep From S&HPrya ChairullahPas encore d'évaluation
- Schizophrenia: From Neurophysiological Abnormalities To Clinical SymptomsDocument6 pagesSchizophrenia: From Neurophysiological Abnormalities To Clinical SymptomsPrya ChairullahPas encore d'évaluation
- DsiofhopweijropwerweDocument1 pageDsiofhopweijropwerwePrya ChairullahPas encore d'évaluation
- Curriculum Vitae Personal DetailsDocument3 pagesCurriculum Vitae Personal DetailsPrya ChairullahPas encore d'évaluation
- National Clinical Guidelines For Stroke Fourth EditionDocument232 pagesNational Clinical Guidelines For Stroke Fourth EditionAnna Apetri100% (1)
- PopreoporerpioDocument1 pagePopreoporerpioPrya ChairullahPas encore d'évaluation
- GhtytytDocument1 pageGhtytytPrya ChairullahPas encore d'évaluation
- Many Sleep Disturbance ParkinsonDocument7 pagesMany Sleep Disturbance ParkinsonPrya ChairullahPas encore d'évaluation
- Sleep Disturbance ParkinsonDocument8 pagesSleep Disturbance ParkinsonPrya ChairullahPas encore d'évaluation
- Reduced Striatal DopaminergicDocument7 pagesReduced Striatal DopaminergicPrya ChairullahPas encore d'évaluation
- Reduced Striatal DopaminergicDocument7 pagesReduced Striatal DopaminergicPrya ChairullahPas encore d'évaluation
- Dopamine and Sleep From S&HDocument13 pagesDopamine and Sleep From S&HPrya ChairullahPas encore d'évaluation
- Brain 2005 Stiasny Kolster 126 37Document12 pagesBrain 2005 Stiasny Kolster 126 37Prya ChairullahPas encore d'évaluation
- 55450048Document6 pages55450048Prya ChairullahPas encore d'évaluation
- Ni Hms 415433Document9 pagesNi Hms 415433Prya ChairullahPas encore d'évaluation
- Hijri Calander 1434Document1 pageHijri Calander 1434mameeranPas encore d'évaluation
- 2010 Article 154Document5 pages2010 Article 154Prya ChairullahPas encore d'évaluation
- Cho JYDocument1 pageCho JYPrya ChairullahPas encore d'évaluation
- Retinopati DiabetikDocument5 pagesRetinopati DiabetikMuhammad Afriadi HamdanPas encore d'évaluation
- Pi Is 1040842812001163Document12 pagesPi Is 1040842812001163Prya ChairullahPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Valproic Acid DsDocument2 pagesValproic Acid DsCarissa Mae Tapec EstradaPas encore d'évaluation
- HealthMeans Lets Talk About AutoimmunityDocument37 pagesHealthMeans Lets Talk About AutoimmunityvaleriabostanPas encore d'évaluation
- Non-Sickle HB Variants.091611Document44 pagesNon-Sickle HB Variants.091611Sumihar PasaribuPas encore d'évaluation
- Side EffectsDocument2 pagesSide EffectsFahad AlkenaniPas encore d'évaluation
- Alternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Document159 pagesAlternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Marvin T Verna100% (2)
- Produk Vaksin JapfaDocument46 pagesProduk Vaksin JapfaAnanda UNANDPas encore d'évaluation
- Personal Health Issues and ConcernDocument41 pagesPersonal Health Issues and Concernniña pinedaPas encore d'évaluation
- Learning Area Grade Level Quarter Date: English 9 4Document4 pagesLearning Area Grade Level Quarter Date: English 9 4Kim So-Hyun100% (1)
- Garssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPDocument3 pagesGarssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPkarinaPas encore d'évaluation
- Osce RadioDocument74 pagesOsce Radioberhanu nathanielPas encore d'évaluation
- Midterm Activity ScitechDocument3 pagesMidterm Activity ScitechKean KaiPas encore d'évaluation
- Aleukemic LeukemiaDocument3 pagesAleukemic LeukemialilisPas encore d'évaluation
- 2020 - Psychological Therapies For People With Borderline Personality Disorder - Storebø Et AlDocument522 pages2020 - Psychological Therapies For People With Borderline Personality Disorder - Storebø Et AlFabian MaeroPas encore d'évaluation
- Faisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Document37 pagesFaisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Muhammad Khairul AfifPas encore d'évaluation
- JH CERILLES STATE COLLEGE - Post TestDocument7 pagesJH CERILLES STATE COLLEGE - Post TestCrystal Ann TadiamonPas encore d'évaluation
- Lapp Jan2020Document88 pagesLapp Jan2020Siti RojanahPas encore d'évaluation
- Hypercalcemia in Dogs Emergent Care Diagnostics and TreatmentsDocument8 pagesHypercalcemia in Dogs Emergent Care Diagnostics and Treatmentstarilubis277Pas encore d'évaluation
- 1-4, 2016 qhd1Document205 pages1-4, 2016 qhd1waleed.almusharaf100% (1)
- 3rd Year Bcqs Hhhpathology-2Document38 pages3rd Year Bcqs Hhhpathology-2Hira PanhwerPas encore d'évaluation
- Assignment 1 Part 1 A1Document10 pagesAssignment 1 Part 1 A1garrenaPas encore d'évaluation
- CV of BaifengZhang.2023Document3 pagesCV of BaifengZhang.2023Baifeng ZhangPas encore d'évaluation
- Benign Breast DiseasesDocument35 pagesBenign Breast DiseasesBhim Nath KharelPas encore d'évaluation
- AZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Document1 pageAZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Brittany LudwigPas encore d'évaluation
- Child Abuse Nursing Care PlansDocument7 pagesChild Abuse Nursing Care PlansMAHESH KOUJALAGIPas encore d'évaluation
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 pagesPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuPas encore d'évaluation
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Journal Reading RPL EditDocument30 pagesJournal Reading RPL EditAnonymous l6Q1ROq2Pas encore d'évaluation
- Digital Covid Questionnaire For Revival Approval FormatDocument2 pagesDigital Covid Questionnaire For Revival Approval Formatsouravdey3Pas encore d'évaluation
- Heart Failure Case StudyDocument8 pagesHeart Failure Case StudyDavid PayosPas encore d'évaluation
- Depression and Diabetes Slides ENGDocument20 pagesDepression and Diabetes Slides ENGMaria Magdalena Dumitru100% (1)