Vous aimerez peut-être aussi
- The Ultimate Male Orgasm PDFDocument4 pagesThe Ultimate Male Orgasm PDFDavid Hosam50% (2)
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHDocument32 pagesICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Hesi Maternity Ob PDFDocument32 pagesHesi Maternity Ob PDFcclaire197% (37)
- 1000 Cuvinte EnglezaDocument10 pages1000 Cuvinte EnglezaNotar SorinPas encore d'évaluation
- 1000 Cuvinte EnglezaDocument10 pages1000 Cuvinte EnglezaNotar SorinPas encore d'évaluation
- The G-Spot FAQ PDFDocument2 pagesThe G-Spot FAQ PDFDavid HosamPas encore d'évaluation
- Procedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowDocument8 pagesProcedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowMarjorie Dulay Dumol80% (5)
- Earl Nightingale - Lead The FieldDocument7 pagesEarl Nightingale - Lead The Fieldontemp100% (3)
- C - VVV VV VVVV VVV - VVV VV - VVVV VV VVDocument3 pagesC - VVV VV VVVV VVV - VVV VV - VVVV VV VVBea Angela Bithao AnonoyPas encore d'évaluation
- Magnesium SulfateDocument5 pagesMagnesium SulfateRyan Inapan100% (1)
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarPas encore d'évaluation
- The Future Mixed TensesDocument4 pagesThe Future Mixed TensesChernykh Vitaliy100% (1)
- The Role of Magnesium Sulphate in Obstetrics: by Sneha Sehrawat M.S C Nursing I YearDocument18 pagesThe Role of Magnesium Sulphate in Obstetrics: by Sneha Sehrawat M.S C Nursing I YearRaja100% (1)
- DRUG STUDY Magnesium SulfateDocument4 pagesDRUG STUDY Magnesium SulfateTempoPas encore d'évaluation
- Drug Study On MAGNESIUM SULFATEDocument6 pagesDrug Study On MAGNESIUM SULFATEshadow gonzalezPas encore d'évaluation
- Creativity-Flow and The Psychology of Discovery and InventionDocument13 pagesCreativity-Flow and The Psychology of Discovery and InventionPratick Tibrewala50% (2)
- Magnesium Sulfate: Injection, USPDocument13 pagesMagnesium Sulfate: Injection, USPRagesh .MPas encore d'évaluation
- Magnesium Sulfate in Water For Injection: Flexible Plastic Container For Intravenous Use OnlyDocument5 pagesMagnesium Sulfate in Water For Injection: Flexible Plastic Container For Intravenous Use OnlyKN BaijuPas encore d'évaluation
- Magnesium Sulfate: Injection, UspDocument13 pagesMagnesium Sulfate: Injection, Uspnur-aisyahkPas encore d'évaluation
- Nalepsin: Presentation Drug InteractionsDocument1 pageNalepsin: Presentation Drug InteractionsAbid Hasan ZiKonPas encore d'évaluation
- Plumb 2Document3 pagesPlumb 2Erick ManosalvasPas encore d'évaluation
- Cloxacillin, Sodium: How Should I Take Cloxacillin?Document7 pagesCloxacillin, Sodium: How Should I Take Cloxacillin?Stacy MC PelitoPas encore d'évaluation
- Magnesium ReplacementDocument4 pagesMagnesium ReplacementArvenaa SubramaniamPas encore d'évaluation
- Magnesium Sulfa-WPS OfficeDocument21 pagesMagnesium Sulfa-WPS OfficeNeha SinghPas encore d'évaluation
- Magnesium Sulphate InjDocument2 pagesMagnesium Sulphate InjmahgadPas encore d'évaluation
- Mefenamic AcidDocument6 pagesMefenamic AcidArisa VijungcoPas encore d'évaluation
- Magnesium SulfateDocument2 pagesMagnesium SulfateKarla Karina Dela CruzPas encore d'évaluation
- Resurrection University Medication CardDocument2 pagesResurrection University Medication CardBohung ConPas encore d'évaluation
- UKMI QA How Is Acute Hypomagnesaemia Treated in Adults Update July 2017Document5 pagesUKMI QA How Is Acute Hypomagnesaemia Treated in Adults Update July 2017marwanPas encore d'évaluation
- Acetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, IncDocument9 pagesAcetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, Incandi hasri ainunPas encore d'évaluation
- Acetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, IncDocument13 pagesAcetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, Incandi hasri ainunPas encore d'évaluation
- OBG Latest DrugDocument71 pagesOBG Latest DrugT. Lamnunnem HaokipPas encore d'évaluation
- Acetazolamide For Injection, USPDocument5 pagesAcetazolamide For Injection, USPbishoy.youssef.cpiPas encore d'évaluation
- Magnesium Sulfate - Management of Hypertensive Disorders of PregnancyDocument7 pagesMagnesium Sulfate - Management of Hypertensive Disorders of PregnancySylvester J DakaPas encore d'évaluation
- SPC Pramipexole 0.7 MGDocument14 pagesSPC Pramipexole 0.7 MGJehan SarahdiniPas encore d'évaluation
- 8 Drug StudyDocument19 pages8 Drug StudyLoyloy D ManPas encore d'évaluation
- Antigout PDFDocument21 pagesAntigout PDFshaifPas encore d'évaluation
- Gout and HyperuricemiaDocument7 pagesGout and HyperuricemiaTaj lamajedPas encore d'évaluation
- Furosemide Tables:: Pharmacokinetics Bioavailability Peak Plasma Level Plasma Half-Life Active Metabolites EliminationDocument4 pagesFurosemide Tables:: Pharmacokinetics Bioavailability Peak Plasma Level Plasma Half-Life Active Metabolites Eliminationmole_fkPas encore d'évaluation
- Pepto - Bismol Rev 2009Document8 pagesPepto - Bismol Rev 2009martins0105Pas encore d'évaluation
- Myrin P ForteDocument3 pagesMyrin P ForteJohn Zedric Villanueva ArciagaPas encore d'évaluation
- Drug StudyDocument20 pagesDrug StudydjanindPas encore d'évaluation
- Magnesium, Phosporus and ChlorideDocument9 pagesMagnesium, Phosporus and ChlorideSophia Gayle RaagasPas encore d'évaluation
- MetFormin Generic Health TabDocument9 pagesMetFormin Generic Health TabNur Ekayani SyamPas encore d'évaluation
- Availability: Verapamil HydrochlorideDocument21 pagesAvailability: Verapamil Hydrochloridesteffy sojanPas encore d'évaluation
- The Role of Magnesium Sulphate in Obstetrics: by Sneha Sehrawat M. C Nursing I YearDocument18 pagesThe Role of Magnesium Sulphate in Obstetrics: by Sneha Sehrawat M. C Nursing I YearRajaPas encore d'évaluation
- Mag So4 Drug StudyDocument4 pagesMag So4 Drug StudyAra MiaPas encore d'évaluation
- Drug InfoDocument11 pagesDrug InfoArjun SinghPas encore d'évaluation
- EpitoinDocument2 pagesEpitoinmahgadPas encore d'évaluation
- Name of The Medicinal Product: 4.1 Therapeutic IndicationsDocument4 pagesName of The Medicinal Product: 4.1 Therapeutic IndicationsIndah BryanKeyPas encore d'évaluation
- Mepivacaine 3%Document6 pagesMepivacaine 3%Victor KurniawanPas encore d'évaluation
- Cardiovascular Agent Central-Acting, Antihypertensive Autonomic Nervous System Agent Alpha-Adrenergic Agonist (Sympathomimetic)Document13 pagesCardiovascular Agent Central-Acting, Antihypertensive Autonomic Nervous System Agent Alpha-Adrenergic Agonist (Sympathomimetic)Maica EspañolaPas encore d'évaluation
- Chapter FourDocument7 pagesChapter FourStanley AnadiPas encore d'évaluation
- Magnesium Sulphat RegimenDocument18 pagesMagnesium Sulphat Regimenmuhammad syamil mumtaz100% (2)
- PharmacologyDocument116 pagesPharmacologyvarghesePas encore d'évaluation
- Drug Study Cefuroxime 125mg IVP q8 No STDocument3 pagesDrug Study Cefuroxime 125mg IVP q8 No STAngge CapistranoPas encore d'évaluation
- AllopurinolDocument31 pagesAllopurinolbeewolPas encore d'évaluation
- For Intravenous Use and Urologic Irrigation: MANNITOL-mannitol Injection, S Olution Fres Enius Kabi USA, LLCDocument7 pagesFor Intravenous Use and Urologic Irrigation: MANNITOL-mannitol Injection, S Olution Fres Enius Kabi USA, LLCroykelumendekPas encore d'évaluation
- Obat Tugas Dokter PhathimhaDocument6 pagesObat Tugas Dokter PhathimhaMegan LewisPas encore d'évaluation
- Sulfa Sal AzineDocument2 pagesSulfa Sal Azineikke alma alukaPas encore d'évaluation
- Suxamethonium Dosage, Side Effect MIMS - Com PhilippinesDocument2 pagesSuxamethonium Dosage, Side Effect MIMS - Com PhilippinesWay LyanPas encore d'évaluation
- Summary of Product Characteristics: Adults (Including Elderly Patients)Document8 pagesSummary of Product Characteristics: Adults (Including Elderly Patients)Yuzark GumintangPas encore d'évaluation
- Leaflet - ProsoganDocument7 pagesLeaflet - ProsoganurmymelodyPas encore d'évaluation
- Calcium Gluconate-Calcium Gluconate Injection, Solution HF Acquisition Co LLC, Dba HealthfirstDocument9 pagesCalcium Gluconate-Calcium Gluconate Injection, Solution HF Acquisition Co LLC, Dba HealthfirstLalrinchhanaPas encore d'évaluation
- Furosemide Mims EngDocument17 pagesFurosemide Mims EngNur Ilmi SofiahPas encore d'évaluation
- Advanced Vision Co PDFDocument1 pageAdvanced Vision Co PDFDavid HosamPas encore d'évaluation
- TOR FOR IBBS Readvertisement PDFDocument10 pagesTOR FOR IBBS Readvertisement PDFDavid HosamPas encore d'évaluation
- Area List Home Delivery Rates PDFDocument3 pagesArea List Home Delivery Rates PDFDavid HosamPas encore d'évaluation
- Message PDFDocument2 pagesMessage PDFDavid HosamPas encore d'évaluation
- Message PDFDocument2 pagesMessage PDFDavid HosamPas encore d'évaluation
- Advanced Vision Co PDFDocument1 pageAdvanced Vision Co PDFDavid HosamPas encore d'évaluation
- Job-Specification - Senior Pharmacist PDFDocument5 pagesJob-Specification - Senior Pharmacist PDFDavid HosamPas encore d'évaluation
- Exam QNSDocument10 pagesExam QNSDavid HosamPas encore d'évaluation
- Mission Stat PDFDocument1 pageMission Stat PDFDavid HosamPas encore d'évaluation
- Mission PDFDocument1 pageMission PDFDavid HosamPas encore d'évaluation
- Positioning Explained PDFDocument3 pagesPositioning Explained PDFAmit GandhiPas encore d'évaluation
- Disney PaperDocument6 pagesDisney PaperTaffarel MicaloskiPas encore d'évaluation
- 1-What Is The Most Common Cause of Acne? A-Bacteria B-Virus C-Fungi D-Food E-None of The Above Ans-EDocument1 page1-What Is The Most Common Cause of Acne? A-Bacteria B-Virus C-Fungi D-Food E-None of The Above Ans-EMuhammad AminPas encore d'évaluation
- Entry Level PharmD Program PDFDocument2 pagesEntry Level PharmD Program PDFDavid HosamPas encore d'évaluation
- Disney PaperDocument6 pagesDisney PaperTaffarel MicaloskiPas encore d'évaluation
- Good CommunicationDocument6 pagesGood CommunicationKranthi KumarPas encore d'évaluation
- 12 The Elements of Great Managing Summarized by KentDocument0 page12 The Elements of Great Managing Summarized by KentSurabhi AroraPas encore d'évaluation
- العاطفة بين الإهمال والإغراقDocument9 pagesالعاطفة بين الإهمال والإغراقDavid HosamPas encore d'évaluation
- Antiflatulents: Labelling StandardDocument6 pagesAntiflatulents: Labelling StandardDavid HosamPas encore d'évaluation
- Anti TB Drugs PDFDocument2 pagesAnti TB Drugs PDFDavid HosamPas encore d'évaluation
- AntibioticsSimplified3e TOCDocument1 pageAntibioticsSimplified3e TOCDavid HosamPas encore d'évaluation
- كيف تواجه التوترDocument6 pagesكيف تواجه التوترDavid HosamPas encore d'évaluation
- AntihistaminesDocument2 pagesAntihistaminesmercywicherPas encore d'évaluation
- E-Therapeutics+ Complete - Therapeutic Choices - Drug Use During Pregnancy PDFDocument5 pagesE-Therapeutics+ Complete - Therapeutic Choices - Drug Use During Pregnancy PDFDavid HosamPas encore d'évaluation
- Code of Conduct For Public OfficialDocument17 pagesCode of Conduct For Public OfficialHaPas encore d'évaluation
- Dosificación Gac007-008 Sem2Document2 pagesDosificación Gac007-008 Sem2Ohm EgaPas encore d'évaluation
- RL78 L1B UsermanualDocument1 062 pagesRL78 L1B UsermanualHANUMANTHA RAO GORAKAPas encore d'évaluation
- 2017 Hu Spence Why Globalization Stalled and How To Restart ItDocument11 pages2017 Hu Spence Why Globalization Stalled and How To Restart Itmilan_ig81Pas encore d'évaluation
- Green ChemistryDocument17 pagesGreen ChemistryAaditya RamanPas encore d'évaluation
- GRADE 302: Element Content (%)Document3 pagesGRADE 302: Element Content (%)Shashank Saxena100% (1)
- Assignment # 1 POMDocument10 pagesAssignment # 1 POMnaeemPas encore d'évaluation
- Abbott 2021 ApJL 915 L5Document24 pagesAbbott 2021 ApJL 915 L5Manju SanthakumariPas encore d'évaluation
- P&CDocument18 pagesP&Cmailrgn2176Pas encore d'évaluation
- Dial 1298 For Ambulance - HSBCDocument22 pagesDial 1298 For Ambulance - HSBCDial1298forAmbulancePas encore d'évaluation
- Centric WhitepaperDocument25 pagesCentric WhitepaperFadhil ArsadPas encore d'évaluation
- Job Stress InterventionsDocument5 pagesJob Stress InterventionscocaralucamihaelaPas encore d'évaluation
- ZEROPAY WhitepaperDocument15 pagesZEROPAY WhitepaperIlham NurrohimPas encore d'évaluation
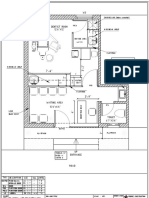
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- DGKCC Internship ReportDocument17 pagesDGKCC Internship ReportMuhammad AtharPas encore d'évaluation
- PCZ 1503020 CeDocument73 pagesPCZ 1503020 Cedanielradu27Pas encore d'évaluation
- Adolescence Problems PPT 1Document25 pagesAdolescence Problems PPT 1akhila appukuttanPas encore d'évaluation
- ReflectionDocument3 pagesReflectionapi-174391216Pas encore d'évaluation
- MVC Training Course Prerequisite: WWW - Focustech.InDocument2 pagesMVC Training Course Prerequisite: WWW - Focustech.InLakshman Samanth ReddyPas encore d'évaluation
- Part TOEFLDocument7 pagesPart TOEFLFrisca Rahma DwinantiPas encore d'évaluation
- Course 3 Mathematics Common Core Workbook AnswersDocument4 pagesCourse 3 Mathematics Common Core Workbook Answerspqdgddifg100% (1)
- Btech CertificatesDocument6 pagesBtech CertificatesSuresh VadlamudiPas encore d'évaluation
- Functions of The Gastrointestinal Organs: Muhammad ImranDocument21 pagesFunctions of The Gastrointestinal Organs: Muhammad ImranSalman KhanPas encore d'évaluation
- Kongsberg Oil and Gas Technology LimitedDocument1 pageKongsberg Oil and Gas Technology LimitedGhoozyPas encore d'évaluation
- Exchange 2010 UnderstandDocument493 pagesExchange 2010 UnderstandSeKoFiePas encore d'évaluation
- First Semester-NOTESDocument182 pagesFirst Semester-NOTESkalpanaPas encore d'évaluation
- PresentationDocument6 pagesPresentationVruchali ThakarePas encore d'évaluation
- Introduction To Cobit Framework - Week 3Document75 pagesIntroduction To Cobit Framework - Week 3Teddy HaryadiPas encore d'évaluation