Vous aimerez peut-être aussi
- Department of Labor: Generalprovision 6 28 07Document6 pagesDepartment of Labor: Generalprovision 6 28 07USA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: Yr English GuideDocument1 pageDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Department of Labor: Aces CPDocument36 pagesDepartment of Labor: Aces CPUSA_DepartmentOfLabor100% (2)
- Department of Labor: YouthworkerDocument1 pageDepartment of Labor: YouthworkerUSA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: YouthRulesBrochureDocument12 pagesDepartment of Labor: YouthRulesBrochureUSA_DepartmentOfLaborPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Department of Labor: Final ReportDocument37 pagesDepartment of Labor: Final ReportUSA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: Niosh Recs To Dol 050302Document198 pagesDepartment of Labor: Niosh Recs To Dol 050302USA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: Niosh Letter FinalDocument3 pagesDepartment of Labor: Niosh Letter FinalUSA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: 20040422 YouthrulesDocument1 pageDepartment of Labor: 20040422 YouthrulesUSA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: ln61003Document2 pagesDepartment of Labor: ln61003USA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: JYMP 11x17 3Document1 pageDepartment of Labor: JYMP 11x17 3USA_DepartmentOfLaborPas encore d'évaluation
- Department of Labor: Yr English GuideDocument1 pageDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Islamic InsurancedlcDocument43 pagesIslamic InsurancedlcNadzirah SamsuddinPas encore d'évaluation
- ESISDocument28 pagesESISDhananjaySalgaonkarPas encore d'évaluation
- The Motor Vehicles Act, 1988 - History, ObjectDocument17 pagesThe Motor Vehicles Act, 1988 - History, ObjectAISHWARYA SURENDRAN VPas encore d'évaluation
- Exide Life Powering Life Limited Payment Endowment Plan (Elr) (Uin 114n010v01)Document7 pagesExide Life Powering Life Limited Payment Endowment Plan (Elr) (Uin 114n010v01)Navpreet Singh RandhawaPas encore d'évaluation
- Risk ManagementDocument3 pagesRisk ManagementMITHUN MOHANPas encore d'évaluation
- Credit Insurance AaaaaDocument21 pagesCredit Insurance AaaaaRohit GuptaPas encore d'évaluation
- FinalDocument23 pagesFinalNinie NegiPas encore d'évaluation
- A Virtual Assistant Defined Free ReportDocument3 pagesA Virtual Assistant Defined Free ReportdvictoriavaPas encore d'évaluation
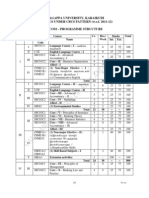
- Alagappa University, Karaikudi SYLLABUS UNDER CBCS PATTERN (W.e.f. 2011-12)Document26 pagesAlagappa University, Karaikudi SYLLABUS UNDER CBCS PATTERN (W.e.f. 2011-12)Mathan NaganPas encore d'évaluation
- Land, Building, and MachineryDocument6 pagesLand, Building, and MachineryPaula Rodalyn MateoPas encore d'évaluation
- Compensation Management Scenario in Pran-RFL Group and Akij Food and Beverage LTDDocument33 pagesCompensation Management Scenario in Pran-RFL Group and Akij Food and Beverage LTDMd. Nazmul Islam100% (2)
- Personal Assigment PDFDocument13 pagesPersonal Assigment PDFImran Azizi Zulkifli67% (3)
- Torts: Fortuitous Events, Waiver, Damnum AbsqueDocument14 pagesTorts: Fortuitous Events, Waiver, Damnum AbsqueReena MaPas encore d'évaluation
- Indias Top 500 Companies 2018Document502 pagesIndias Top 500 Companies 2018ayush guptaPas encore d'évaluation
- Ic s01 Survey and Loss AssessmentDocument55 pagesIc s01 Survey and Loss AssessmentRanjith33% (3)
- Insurance: M.J.Malik-Sba-Ahmedabad-09879094925MWPADocument21 pagesInsurance: M.J.Malik-Sba-Ahmedabad-09879094925MWPAkrunalk2003100% (1)
- Claim Reserving Estimation by Using The Chain Ladder Method: Conference PaperDocument13 pagesClaim Reserving Estimation by Using The Chain Ladder Method: Conference PaperAzhal23Pas encore d'évaluation
- FIDIC GuidelinesDocument30 pagesFIDIC GuidelinesVikas Reddy Marepally100% (3)
- Request For Premium Holiday PDFDocument2 pagesRequest For Premium Holiday PDFMarie CrystallinePas encore d'évaluation
- Financial Plan Gold Review: XXXX & FamilyDocument5 pagesFinancial Plan Gold Review: XXXX & FamilySachin BehlPas encore d'évaluation
- Kidnap and Ransom Proposal Form-1Document3 pagesKidnap and Ransom Proposal Form-1gargramPas encore d'évaluation
- Feasibility of Traditional Insurance Vs FinTechDocument12 pagesFeasibility of Traditional Insurance Vs FinTechKiamba M Kelvin100% (1)
- Benefits Summary Updated (Contractors) FinalDocument25 pagesBenefits Summary Updated (Contractors) FinalSithu HeinPas encore d'évaluation
- Malayan V CaDocument2 pagesMalayan V CaninaPas encore d'évaluation
- 2019 - BestPracticesAgritourism FINALDRAFT LoresDocument74 pages2019 - BestPracticesAgritourism FINALDRAFT Loresmilrosebatilo2012Pas encore d'évaluation
- Research ProposalDocument23 pagesResearch Proposalnidamah100% (2)
- Asymmetric InformationDocument15 pagesAsymmetric InformationKarpagam MahadevanPas encore d'évaluation
- Des Ques CutDocument39 pagesDes Ques CutS. NarangPas encore d'évaluation
- MIB Inc Medical Information Bureau Fact SheetDocument8 pagesMIB Inc Medical Information Bureau Fact Sheetannualmedicalreport.comPas encore d'évaluation
- Sempra Analysts Conference, June 2018Document115 pagesSempra Analysts Conference, June 2018Rob NikolewskiPas encore d'évaluation