Vous aimerez peut-être aussi
- Needle Akpt PDFDocument275 pagesNeedle Akpt PDFsolihati100% (1)
- Meridian Connective TissueDocument9 pagesMeridian Connective TissueklstrainPas encore d'évaluation
- Vol6.5 RonanDocument13 pagesVol6.5 RonanensemblenunPas encore d'évaluation
- Vol6.5 RonanDocument13 pagesVol6.5 RonanensemblenunPas encore d'évaluation
- Hammer Blocks StructureDocument20 pagesHammer Blocks StructureensemblenunPas encore d'évaluation
- Hammer Blocks StructureDocument20 pagesHammer Blocks StructureensemblenunPas encore d'évaluation
- Hammer Blocks StructureDocument20 pagesHammer Blocks StructureensemblenunPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Self-Critique and Learning Application AssignmentDocument2 pagesSelf-Critique and Learning Application Assignmentapi-548491914Pas encore d'évaluation
- Integrative Managerial IssuesDocument31 pagesIntegrative Managerial IssuesЗорана МанићPas encore d'évaluation
- Reggio EmiliaDocument5 pagesReggio EmiliaAnonymous a0cuWVM100% (3)
- Research Chapter 1 SampleDocument5 pagesResearch Chapter 1 Samplebea gPas encore d'évaluation
- FossilizationDocument4 pagesFossilizationKrySt TeyPas encore d'évaluation
- Enhanced Intervention PosterDocument1 pageEnhanced Intervention PosterInclusionNorthPas encore d'évaluation
- Lock WallaceDocument2 pagesLock WallaceVeronika CalanceaPas encore d'évaluation
- 1-4 Learners' Packet in PRACTICAL RESEARCH 1Document33 pages1-4 Learners' Packet in PRACTICAL RESEARCH 1Janel FloresPas encore d'évaluation
- Soft Skills EssayDocument2 pagesSoft Skills Essayapi-5228592320% (1)
- Problems Encountered by Beginning Family and Consumer Sciences TeachersDocument12 pagesProblems Encountered by Beginning Family and Consumer Sciences TeachersTayo BethelPas encore d'évaluation
- Issue Brief: Effects of COVID-19 On Our Mental Health and The Call For ActionDocument3 pagesIssue Brief: Effects of COVID-19 On Our Mental Health and The Call For ActionJoshua TejanoPas encore d'évaluation
- ESSAYDocument2 pagesESSAYJohn Rey De Asis0% (1)
- Instructor II: Instructor and Course EvaluationsDocument42 pagesInstructor II: Instructor and Course Evaluationsjesus floresPas encore d'évaluation
- 09 PEDIA250 (5) Developmental Pediatrics PDFDocument5 pages09 PEDIA250 (5) Developmental Pediatrics PDFJudith Dianne IgnacioPas encore d'évaluation
- Temporary Progress Report Card For ElementaryDocument4 pagesTemporary Progress Report Card For ElementaryJay Ralph Dizon100% (1)
- Tip 5Document3 pagesTip 5api-454303170Pas encore d'évaluation
- Closing The GapactionplansocialDocument1 pageClosing The Gapactionplansocialapi-363248890100% (1)
- Infidelity and Behavioral Couple TherapyDocument12 pagesInfidelity and Behavioral Couple TherapyGiuliutza FranCescaPas encore d'évaluation
- An Experimental Study To Assess-5996Document5 pagesAn Experimental Study To Assess-5996Priyanjali SainiPas encore d'évaluation
- 11 Hmef5053 T7Document12 pages11 Hmef5053 T7kalpanamoorthyaPas encore d'évaluation
- Research Paper 1Document3 pagesResearch Paper 1api-551958955Pas encore d'évaluation
- A Thesis Submitted To The Department of English and Humanities of BRAC University by Ishrat Akhter ID: 15163012Document66 pagesA Thesis Submitted To The Department of English and Humanities of BRAC University by Ishrat Akhter ID: 15163012Asma RaniPas encore d'évaluation
- WinnerDocument586 pagesWinnerJames AdhikaramPas encore d'évaluation
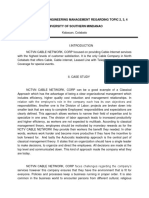
- A Case Study in Engineering Management Regarding Topic 2, 3, 4 University of Southern MindanaoDocument2 pagesA Case Study in Engineering Management Regarding Topic 2, 3, 4 University of Southern MindanaoMaechille Abrenilla CañetePas encore d'évaluation
- Parenting Styles Thesis PDFDocument5 pagesParenting Styles Thesis PDFljctxlgld100% (1)
- College of Criminal Justice Education: Rizwoods CollegesDocument10 pagesCollege of Criminal Justice Education: Rizwoods CollegesVin SabPas encore d'évaluation
- Theoriess - Mr. BajetDocument61 pagesTheoriess - Mr. BajetMaria Cristina DelmoPas encore d'évaluation
- (Module 9) - Case Study AnalysisDocument20 pages(Module 9) - Case Study AnalysisAnonymous EWWuZKdn2w100% (5)
- Trends Summative 3Document3 pagesTrends Summative 3fio jennPas encore d'évaluation
- Functions and Principles of School Administration and SupervisionDocument56 pagesFunctions and Principles of School Administration and SupervisionVallerie Breis71% (7)