Académique Documents
Professionnel Documents
Culture Documents
Pharm Article#1
Transféré par
Michael KuzbytDescription originale:
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Pharm Article#1
Transféré par
Michael KuzbytDroits d'auteur :
Formats disponibles
Nilam A.Gadhave et al.
/ Journal of Pharmacy Research 2011,4(7),2107-2119
Review Article ISSN: 0974-6943
Available online through www.jpronline.info
Tuberculosis: A dreaded or curable disease- A Review
Nilam A. Gadhave*, Kedar S. Lade 1 ,Meera C. Singh 2, Sanjay D. Sawant3 Smt. Kashibai Navale College Of Pharmacy, Saswad Kondhwa Road, S. No 40/4, near Octroi post, Kondhawa (Bk), Pune 411048, Maharashtra, India.
Received on: 12-04-2011; Revised on: 18-05-2011; Accepted on:21-06-2011 ABSTRACT
Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis is usually involves the lungs but may affect any organ or tissue in the body. Tuberculosis granulomas undergoes cereous necrosis among medically and economically deprived persons through out the world. TB continues to be the leading killer disease for Indian adults amongst all infectious diseases. More than 80% of TB patients have pulmonary TB. The WHO recommended DOTS strategy is the most effective tool for TB control. All treatment regimens is RNTCP have two phases; an intensive phase & continuation phase. MDR- TB is caused by strain of the TB bacteria resistant to at least the two most effective Anti-TB drugs; namely Isoniazid & Rifampicin. To prevent MDR-TB is to ensure the provision of effective regimens of short-course treatment with first-line drugs. Also laboratory test use for diagnosis of TB. It is estimated that one third of world population is infected with TB. Development of drug resistance in the population has increased concern that TB may once again become an incurable disease (MDR-TB) .The insufficient knowledge of the mechanism of pathogenesis and protection from it, creates a need to establish long-term and effective tuberculosis treatment and control programmes Key words: Mycobacterium tuberculosis, MDR- TB, Middlebrooks medium, Lowenstein-Jensen medium.
INTRODUCTION
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis. Pulmonary tuberculosis is the most common form of TB (more than 85% of all TB cases.), While extra-pulmonary tuberculosis can affect almost any organ in the body. Transmission occurs by airborne spread of infectious droplets and droplet nuclei containing the tubercle bacilli. The source of infection is a person with sputum smear-positive pulmonary TB. Transmission often occurs indoors, where droplets and droplet nuclei can stay in the air for a long time. There were globally an estimated 8.8 million new cases of TB, of which 3.9 million were sputum smear positive, and 80% were in 22 high burden countries. One fifth of the global TB incidence is in India, with 1.8 million new cases occurring every year and 0.8 million of these being infectious smear-positive cases. In India, an estimated 4 lakh deaths occur from TB every year. Every Day, in India. More than 5000 develop TB disease. More than 1000 people die of TB ( 2 deaths every 3 minutes) TB is a serious public health problem in India causing immense morbidity, mortality and distress to individuals, families and communities. TB kills more adults in India than any other infectious disease. The disease incidence peaks in people belonging to the most economically productive age group of 15-60 years. The link between TB and HIV is quite significant with WHO estimating that 5% of TB patients are also co infected with HIV. Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis is usually involves the lung but may affect any organ or tissue in the body. Tuberculosis granulomas undergo cereous necrosis among medically and economically deprived persons through out the world. TB remains a leading cause of death. Since time immemorial Tuberculosis (TB) has been a scourge to mankind. Fossil bones dating back to 8000 BC provide the earliest evidence of TB in man and animal. TB was responsible for 20% of deaths in London in 1651. Benjamin Morton made the first credible speculation on the infection nature of TB in 1722. In early 19 th Century, TB probably accounted for a third of all deaths in Paris. In 1890, Koch announced that culture filtrate of tubercle bacilli tubercle bacilli cured the disease. Those filtrates, later partially purified, become the principal means to establish infection the tuberculin skin test. During late 19 Century, pasteurization of cow, milk was started to reduce the possibility of infection of Mycobacterium bovis being a cause of human TB. In 1908, Albert Calmette and Camille Guerin, seeking to overcome the problem of bacillary clumping associated with Mycobacteria, grew bovine tubercle bacilli in dispersed culture that contained ox bile. The varian 231 st passage was first used to immunize a child whose died of TB after childbirth. This vaccine, BCG (bacilli Calmette Guerin) is still the most widely used vaccine in the world. The discovery of p -amino salicylic acid by Bernhein in 1941 was the first step in the development of effective anti- TB therapeutic agents. The introduction antibiotics, streptomycin in 1947 were the first successful antibiotics in chemotherapeutics intervention of TB. But its full therapeutic potential could be utilized only after 1952 when isoniazid ( INH) was used simultaneously with streptomycin. Though isoniazid was first synthesized in 1912, its effectiveness against TB was not known for long time until its successful use in 1952. Even today, isoniazid is the most potent anti-TB drug both singly and in combinations (including FDCs i.e. fixed dose combinations) it is the most important, effective and potent first line anti-TB drug susceptible strains of tubercular mycobacteria in man. The major problem of INH is the most commonly used anti-TB drug because of it s better therapeutic efficacy and safety over other available antiTB drugs. Tuberculosis is estimated to affect 1.7 billion individual worldwide, with 8 to 10 million new cases and 1.7 million deaths each year. After HIV, tuberculosis is the leading infection cause of death in the world. Infection with HIV makes people susceptible to rapidly progressive tuberculosis; over 50 million people are infected with both HIV and M. tuberculosis. From 1985 to 1992, the number of tuberculosis cases in the United States increased by 20% because of increase in the disease among people with HIV, among immigrants, and among those in jail or homeless shelters. Because of increased public health efforts, the number of cases of tuberculosis has declined since 1993. Currently, there are about 16, 00 new cases of active tuberculosis in the united states annually, and about 45% of theses are in immigrants. Tuberculosis flourishes wherever there is poverty, crowding, and chronic debilitating illness. In the United States, tuberculosis is mainly a disease of the elderly, the urban poor, and people with AIDS. Certain disease states also increase the risk; diabetes mellitus, Hodgkins lymphoma, chronic lung disease (particulary silicosis), chronic renal failure, malnutrition, alcoholism, and immunosuppression. More than half (50%) of cases involving foreign-born individuals in 2005 were reported in persons from Mexico (25%), Philippines (11%), Vietnam (8%), India (7%), & China (5%). Foreign-born persons account for a steadily increasing proportion of all reported TB cases. An estimated 10-15 million people in the United- states have latent infection.
*Corresponding author.
Nilam A. Gadhave Smt. Kashibai Navale College of Pharmacy, Saswad Kondhwa Road, S. No 40/4, near Octroi post, Kondhawa (Bk), Pune 411048, Maharashtra, India. Tel.: + 91-9960237674 E-mail: nilam.gadhave@yahoo.in
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
It is important that infection with M. tuberculosis be differentiated from disease. Infection is the presence of organism, which may or may not cause clinically significant disease. Typical signs of TB are: Chronic or persistent cough and sputum production. If the disease is at an advanced stage the sputum will contain blood. Fatigue. Lack of appetite. Fever. Night sweats. The general symptoms of TB disease including feeling sick or weak, weight loss, fever and chest pain. Other symptoms depend on the part of body that is affected. Most infections are acquired by person-to-person transmission of airborne droplets of organisms from an active case to a susceptible host. In most people, primary tuberculosis is asymptomatic, although it may cause fever and pleural effusion. Generally, the only evidence of infection, if any remains, is a tiny, fibrocalcific nodule at the site of the infection; viable organisms may remain dormant in such lesions for decades. When the persons immune defenses are lowered, the infection may reactivate to produce communicable and potentially life-threatening disease. Infection with M. tuberculosis typically leads to the development of delayed hypersensitivity to M. tuberculosis antigens, which can be detected by the tuberculin (Montoux) test. About 2 to 4 weeks after infection, intracutaneous injection of purified derivative of M. tuberculosis (PPD) induces visible and palpable induration that peaks in 48 to 72 hours. TB :THE STUDY As per WHO 1.7 billion people infected worldwide. 3 millions deaths occur per year and about 8 million new cases admit per year. Tuberculosis is an infectious disease, that usually affect the lungs but that can attack other parts of the body. There are two forms of tuberculosis-TB infection & TB disease. Most people with TB have TB infection. Common symptoms of TB loss of strength, weight loss, rise in temperature mostly in evening time, cough, pain in chest, blood in the sputum. And also a common cause of TB Alcohol, smoking, mental stress & strain, unhealthy living style, loss of sleep, exposure to cold, hence it is estimated that one third of world population is infected with TB, so it is required to development of drugs resistance in population has increased concern that TB may once again become an incurable disease (MDR-TB) . Also there is insufficient knowledge of the mechanisms of it s pathogenesis and protection from it, so it is necessary to establish long-term and effective tuberculosis treatment and control programmed. CAUSATIVE ORGANISM - MYCOBACTERUM TUBERCULOSIS .1 Mycobacteria are transition from between bacteria and fungi. These genus mycobacteria belong to the order actinomycetaes and family mycobacteriaseae. Non-motile, non- sporulating rods that resist decolorisation with acidified organic solvents. For this reason, they are called acid-fast bacteria. Mycobacteria are slender bacilli and sometimes exhibit filamentous forms resembling fungal mycelium. They are difficult to stain by ordinary stains because of the presence of waxy materials in their cell walls. Four very closely related species are responsible for mammalian tuberculosis, M. tuberculosis (human tubercle bacillus), and M. bovine tubercle bacillus) M. microti (vole tubercle bacillus) and M. africanum (intermediate in form between human and bovine types) Tubercle bacilli are thin straight rods, measuring about 0.4-3. Mycobacteria are strict aerobes and derive energy from the oxidation of many simple carbon compounds. Increased CO2 tension enhances growth. CULTURE Tubercle bacilli are aerobes, grow slowly (generation time 14-15hrs.) optimum temperature 37 C, PH-6.4-7.0 They grow only in specially enriched media containing egg, asparagines, and potatoes, serum and meat extracts. Colonies appear in 2-6 weeks. Mycobacteria are be killed by exposure to direct sunlight for 2hrs. However bacilli may remain alive for 20-30hrs.In sputum culture viable for 6-8 months at room temperature and may be stored for two years at-20 C. Reaction to physical and chemical agentsMycobacteria tend to be more resistant to chemical agents than other bacteria of the hydrophobic nature of cell surface and their clumped growth. Mycobacteria are relatively to chemical disinfectants surviving exposure. They are better stained by hot carbol fuchsin and once stained, they resist decolourisation by dilute mineral acid and are therefore referred to as acid fast bacilli is called as gram-positive bacteria. CULTURE MEDIUM A) LIQUID MEDIUM Liquid media are used for drug sensitivity, biochemical tests and preparation of antigen and vaccine. The bacilli grow either on surface as pellicle or as floccules throughout the medium due to hydrophobic nature of their cell wall (lipid) diffuse bacterial growth can be obtained by addition of a detergent tween-80. Dubo s medium containing casein hydrolysate, bovine serum albumin, aspargine and certain salts with Tween 80 is widely used liquid medium. B) SOLID MEDIUM Most solid medium contain egg, blood, serum or potato. Lowenstein-Jensen (Lj) Medium is the most widely used solid medium. It contains hens egg, aspargine, buffer solution and malachite green. Malachite green inhibits contaminants. Glycerol is replaced by pyruvic acid. In Lj medium, visible colonies appear after 2-6 week, incubation for 6-8 week before being discarded. The colonies of M.tuberculosis appear dry rough, yellowish or buff colored and those of M.bovise are moist, smmoth, flat and white. Two media are used to grow M.TB. Middlebrooks medium which is an agar based medium and Lowenstein-Jensen medium which is an egg based medium. M.TB. colonies are small and buff colored when grown on either medium. Both types of media contain inhibitors to keep contaminants from out-growing M.TB. It takes 4-6 weeks to get visual colonies on either type of media.
Fig1. Mycobacterium tuberculosis. Acid-fast stain. CDC.
Fig 2. Colonies of Mycobacterium tuberculosis on Lowenstein-Jensen medium. CDC
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
BIOCHEMICAL REACTION The following biochemical tests are helpful in distinguishing different species of Mycobacteria. 1. NIACIN TEST Although all Mycobacteria produce niacin, a nicotinic acid, during growth, but only M.Tuberculosis produces niacin, a sufficient quantities in egg medium to give a positive test. The reagent contains 10%cyanogens bromide & 40%aniline in ethanol. When a freshly prepared reagent is added to a suspension of bacterial culture, a canary yellow color shows a positive reaction. Positive niacin test is also seen with culture of M.Chelonee and M. Simiae. 2. ARY SULPHATASE TEST The test becomes positive in culture at atypical mycobacteria as they from the enzyme arylsulphatase. The bacteria are grown in media containing tripotassium phenolphthalein disulphate (0.001M) for 2-4 weeks. To the culture medium when 0.2 N NaOH is added drop by drop, a pink color develops in positive reaction due to liberation off free phenolphthalein. 3. CATALASE TEST Most atypical mycobacteria are strongly catalase positive and peroxide negative. The tubercle bacilli (M.Tuberculosis, M. bovis ) are peroxides, positive and weakly. Catalase positive and weakly catalase positive. Tubercle bacilli loose peroxides and catalase activity when they become INH- resistant. The reagent is prepared by mixing equal volume of 30% volume H2O2 and 0.27% catechol in distilled water. This reagent is added to a 5ml test culture in phosphate buffer (PH-7) at 68 C in a water bath and left for few minutes for the reaction to occur catalase production is indicated by and effervescence and peroxidase activity by browning of colonies. 4. NEUTRAL RED TEST The virulent, strains of tubercle bacilli can bind neutral red in alkaline buffer solution whereas avirulent strains fail to do so. Positive result are with the M.tuberculosis, M.bovis, M.avium, M.ulcerrans. 5. AMIDASE TEST Atypical mycobacteria are differentiated by their ability to split amides. The amides commonly used for the test are acetamide, benzamide, carbamide, nicotinamide and pyrazinamide M.tuberculosulsis nicotinamidase and pyrazinamidase. 6. NITRATE REDUCTION TEST M.tuberculosis can reduced nitrate but in M.bovis cannot. The test organism is Suspended in a buffer solution containing nitrate and incubated at 57C for 3hrs. Then sulphanilamides and N-Napthylethlene diamine dihydrochloride solution is added. Positive reaction is indicated by development of pink or red color. 7. SUSCEPTIVILITY TO PYRAZINAMIDE M.tuberculosis is sensitive to 50g/ml pyraziamide while either mycobacteria including M.bovis are resistant. 8. SUSCEPTABILITY TO THIOPHEN-2-CARBOXYLIC ACID HYDRZIDE (TCH) The growth of M.tuberculosis is usually not inhibited by addition of 10g/ml TCH. However south Indian strains of M.tuberculosis are susceptible M.bovis is usually susceptible to the chemical. MODE OF TRANSMISSION Human being acquires infection with tubercle bacilli by one of the following routes Inhalation of organism present on free cough droplet or in dried sputum from an open case of pulmonary tuberculosis. Ingestion of the organism leads to development of tonsillar or intestinal tuberculosis. This mode of infection of human tubercle bacilli is from selfswallowing of infected sputum of an open case of pulmonary tuberculosis, or ingestion of bovine tubercle bacilli from milk of diseased cows. Inoculation of the organism into the skin may rarely occur from infected postmortem tissue. Tranplacental route result in development of congenital tuberculosis in foetus from infected mother& is a rare mode of transmission. SPREAD OF TUBERCULOSIS The disease spreads in the body by various routes1 . Local spread This takes place by macrophages carrying the bacilli it to surrounding tissues.
Figure No-3. The natural history and spectrum of tuberculosis.
2. Lymphatic spread Tuberculosis is primarily an infection of lymphoid tissues. The bacilli may pass into lymphoid follicles of pharynx, bronchi, intestine or regional lymph nodes resulting in regional tuberculous lymphadenities which is typical of children infections. Primary complex is primary focus with lymphangitis &lymphadenitis. 3. Haematogenous spread This occurs either as a result of tuberculous bacillaemia because of the drainage of lymphatics into the venous system or due to caseous material escaping through ulcerated wall of a vein. This produces millet seed-sized lesions in different organs of the body like lungs, liver, kidneys, bones and other tissues and is known as milltary tuberculosis. 4 . by the natural passages a. Lung lesion into pleura (tuberculous pleurisy ) b. Transbronchial spread into the adjacent lung segments. c. Tuberculous salpingitis into peritoneal cavity.(tuberculous peritonitis) d. Infected sputum into larynx (Tuberculous laryngitis) e. Swallowing of infected sputum (ileocaecal tuberculosis) f. Renal lesions into ureter &down to trigone of bladder. HYPERSENSITIVITY AND IMMUNITY IN TUBERCULOSIS 3 Hypersensitivity or allergy, and immunity or residence, play a major role in the development of lesions in tuberculosis. Tubercle bacilli as such do not produce any toxins. Tissue changes seen in tuberculosis instead the result of host response to the organism which is in the form of development of cellmediated hypersensitivity (or type IV hypersensitivity) and immunity. Both these host responses develop as a consequence of several lipids present in the microorganism which include the following. 1. Mycosides such as cord factor which are essential for growth and virulence of the organism in the animals; and 2. Gycolipids present in the mycobacterial cell wall like Wax-D ; which acts as an adjuvant acting along with tuberculoprotein. It has been known since the time of Robert Koch that the tissue reaction to tubercle bacilli is different in healthy animal that is previously ingested (primary infection) from an animal that is previously infected (secondary infection)
1. In the primary infection, intradermal injection of tubercle bacilli into the skin of a healthy guinea pig evokes on visible reaction for 10-14 days. After this period a nodule develops at the inoculation site, which subsequently ulcerated and heals poorly as the guinea pig unlike human begins, does not possess any natural resistance. The regional lymph nodes also develop type of hypersensitivity and are comparable to primary tuberculosis in children although healing invariably occurs in children. 2. In the secondary infection, the sequence of changes is different. The tubercle bacilli are injected into the skin of the guinea pig that has been infected with tuberculosis 4-6 weeks earlier. In 1-2 days, the site of inoculation is indurate which heals quickly and the regional lymph nodes are indicative of hypersensitivity and immunity in the host. Similar type of changes can be produced if injection of live tubercle bacilli is replaced with old tuberculin (OT). Hypersensitivity and immunity are closely and are initiated through T lyumphocytes sensitized against specific antigen in tuberculin. As a result of
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
this sensitization, lymphokines are released from T cells which induced increased microbicidal activity of the macrophages. PATHOGENENESIS OF TUBERCULOSISStages of disease: Disease progression depends on: Strain of M.TB. Prior exposure. Vaccination. Infectious dose. Immune status of the host. Stage 1 Droplet nuclei are inhaled. One droplet nuclei contains no more than 3 bacilli Droplet nuclei are so small that they can remain air-born for extended of time the most effective ( infect ive) droplet nuclei tend to have a diameter of 5 m. Droplet nuclei are generated by during talking, coughing & sneezing. Coughing generates about 3000 droplet nuclei. Talking for 5 minutes generates. 3000 droplet nuclei in one minute. Sneezing generates t he most droplet nuclei by far, which can spread to individuals up to 10 feet away. It is at this stage that the individual becomes tuberculin-positive. This positive tuberculin reaction the result of the host developing a vigorous cell mediated immune (CMI) response. A CMI response must be mounted to control an M.T.B. infection. An antibody mediated immune (AMI) will not aid in the control of a M.T.B infection because M.T.B is intracellular and if extra cellular, it is resistant to complement killing due to the high lipid concentrated in its cell wall. Stage 4 Although a CMI response is necessary to control an M.TB. Infection, it is also responsible for much of the pathology associated with tuberculosis. Activated macrophages may release lytic enzymes and reactive intermediates that facilitate the development of immune pathology. Activated macrophages and T-cells also secrete cytokines that may also play a role in the development of immune pathology, including interleukin I (IL-I), tumor necrosis factor (TNF), and gamma IFN. It is also at this stage that tubercle formation begins. The center of the tubercle is characterized by caseation necrosis meaning semi-solid or cheesy consistency M.T.B. cannot multiply within these tubercle because of the low PH and anoxic environment M.T.B. can however, persisted within these tubercle for extended periods. Although many activated macrophages can be ford surrounding the tubercles, many other macrophages to replicate and hence the tubercle grows.The growing tubercle may invade a bronchus if this happens; M.T.B infection can spread to other parts of the lung. Similarly the tubercle may invade an artery or other blood supply line. The hematogenous spread of M.T.B. may result in extra pulmonary tuberculosis otherwise known as milliary tuberculosis. The name milliary is derived from the fact that metastasizing tubercles are about the same size as a millet seed, a grain commonly grown in Africa.The secondary lesions caused by milliary TB can occur at almost any anatomical location, but usually involve the genitourinary system, bones, joints, lymph nodes, and peritoneum. These lesions are of two types1.Exudative lesions Result from the accumulation of PMNs around M.TB. Here the bacteria replicate with virtually no resistance. This situation gives rise to the formation of a soft tubercle.
Spread of droplet nuclei from one individual to another. CDC. After droplet nuclei are inhaled, the bacteria are nonspecifically taken up by alveolar macrophages. However, the macrophages are not activated and are unable to destroy the intracellular organism.
Tuberculosis begins when droplet nuclei reach the alveoli. When a person inhales air that contains droplets most of the larger droplets become lodged in the upper respiratory tract (the nose and throat), where infection is unlikely to develop. However, the smaller droplet nuclei may reach the small air sacs of the lung (the alveoli), where infection begins. Spread of droplet nuclei from one individual to another. CDC after droplet nuclei are inhaled, the bacteria are nonspecifically taken up by alveolar macrophages. However the macrophages are not activated and are unable to destroy the intracellular organisms. Tuberculosis begins when droplet nuclei reach the alveoli. When a person inhales air that contains droplet most of the larger droplets becomes lodged in the upper respiratory tract. (The nose and throat), where infection is unlikely to develop. However, the smaller droplet nuclei may reach the small air sacs of the lung (the alveoli), where infection begins. Stage 2 Begins 7-21 days after initial infection. M.TB. multiplies virtually unrestricted within inactivated macrophages until the macrophages are burst. Other macrophages begin to extravassate from peripheral blood. These macrophages also phagocytes M.TB but they are also inactivated and hence destroy M.TB. Stage 3 At these stages lymphocytes begins to infiltrate. The lymphocytes specifically T-cells recognize processed and presented M.TB. Antigen in context of MHC molecules. This result in T- cell activation and the liberation of cytokines including gamma interferon (IFN) The liberation of IFN causes in the activation of macrophages. These activated macrophages are now capable of destroying M.TB.
Figure No- 4 The sequence of events in Primary Pulmonary Tuberculosis.
1.Productive or granuliomatous lesions Occur when the becomes hypersensitive to tuberculoprotein. This situation gives rise to the formation of a hard tubercle For unknown reason the caseous centers of the tubercles liquefy. This liquid is very conductive to M. TB. Growth and hence the organism begins to rapidly multiply intracellular. After time, the large antigen load causes the walls of nearby bronchi to becomes necrotic and rupture. This results in cavity formation. This also allows M.TB to spill into other airways and rapidly spread to other parts of the lung. As stated previously, only a very small percent of M.TB. Infection result in disease and even a smaller percentage of M.TB. Infections progress to an advanced stage. Usually the host will begin to control the infection at some point. When the primary lesion heals, it becomes fibrous and calcifies. When
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
this happens the lesions is referred to as the Ghon complex. Depending on the size and severity, the Ghon complex may never subside. Typically the Ghon complex is readily visible upon chest X-ray.Small metastatic foci containing low numbers of M.TB may also calcify. However, in many cases these foci will contain viable organisms. These foci are referred to Simon foci. The Simon foci are also visible upon chest X- ray and are often the site of disease reactivations. TYPE OF TUBERCULOSIS : Lung is the main organ affected in tuberculosis. Depending upon the type of tissue response and age, the infection with tubercle bacilli is of 2 main types. I.Primary tuberculosis & ll. Secondary tuberculosis. I . Primary tuberculosis 5: The infection of an individual who has not been previously infected or immunized is called primary tuberculosis or Ghons complex or childhood tuberculosis.
5
In the case of primary tuberculosis of alimentary tract due to ingestion of tubercle bacilli, a small primary focus is seen in the intestine with enlarged mesenteric lymph nodes producing tabs mesenterica. The enlarged and caseous mesenteric lymph nodes may rupture into peritoneal cavity and cause tuberculous peritonitis. FATE OF PRIMARY TUBERCULOSIS 7 Primary complex may have one of the followed sequences: 1.The lesions of primary tuberculosis of lung commonly do not progress but instead heal by fibrous, and in time undergo calcification and even ossification. 2. In some cases, the primary focus in the lung continues to grow and the caseous material is disseminated through bronchi to the other parts of the same lung or the opposite lung. This is called progressive primary tuberculosis. 3. At times, bacilli may enter the circulation through erosion in a blood vessel and spread to various tissues and organs. This is called primary military tuberculosis and the lesions are seen in organs like liver, spleen, kidney, brain and bone marrow.
Figure No- 5 Primary Plumonary Tuberculosis Figure No-7 Fate of Primary Tuberculosis
The complex or Ghons complex is the lesion produced at the portal of entry with foci in the draining lymphatic vessels and lymph nodes. The most commonly involved tissues for primary complex are lungs and hilar lymph nodes. The other tissues, which may show primary complex, are tonsils and cervical lymph nodes. And in the case of ingested bacilli the lesions may be found in small intestine and mesenteric lymph nodes. The incidence of disseminated from of progressive primary tuberculosis is particularly high in immunocompromised host e.g. in patients of AIDS. Primary complex or Gnons complex in lungs consists of 3 components. 1. Pulmonary component lesions in the lung are the primary focus or Ghons focus. It is 1-2 cm solitary area of tuberculosis pneumonia located under the pleura. In the pleura. In the lower part of upper lobe.
4. In certain circumstances like in lowered resistance and increased hypersensitivity of the host, the healed lesion of primary tuberculosis may get reactivated. The bacilli lying dormant in a cellular caseous material are activated and cause progressive secondary tuberculosis. It affects children more commonly but adult may also develop this kind of progression. II.SECONDARY TUBERCULOSIS 8 The infection an aceullar who has been previously infected or sensitized is called secondary, or post previously or reinfection, or chronic tuberculosis. The infection may be acquired from, 1.Endogenous source such as reactivation or dormant primary complex. 2.Exogenous source such as fresh dose of reinfection by the tubercle bacilli. Secondary tuberculosis occurs most commonly in lungs in the resions of apex. Other sites and tissue, which can be involved, are tonsils. Pharynx, larynx, small intestine and skin. Secondary tuberculosis of other organs and tissues is described in relevant chapters later while that of lungs is discussed here.
Figure No-6 Primary complex or Gnons complex
2. Lymphatic vessel component the lymphatic draining the lung lesion contain phagocytes containing bacilli and may develop beaded. Military tubercles along the The primary complex composed of three components: Ghons locus, draining lymphatics and Hilar lymph nodes. 3. Lymph node component. This consists of enlarged hilar and tracheobronahil lymph nodes in the area drained. The affected lymph nodes are matted and show caseation necrosis.
Figure No-8 Progressive Secondary Tuberculosis
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
Figure No-9 Secondary Pulmonary Tuberculosis
Figure No-11 A Fiberocaseous Tuberculosis
The lesions in secondary pulmonary tuberculosis usually begin as 1-2 cm apical area of consolidation the lung. This may in time develop a small area of central caseation necrosis and peripheral fibrous. It occurs by haematogenous spread of infection from primary complex to the apex of the affected lung where the oxygen lesion is high and favorable for growth of aerobic tubercle bacilli. Microscopically, the appearance is typical of tuberculous granulomas with mcaseation necrosis.Patients with HIV infection previously exposed to tuberculous infection have particularly high incidence of reactivation of primary of primary tuberculosis and the pattern of lesions in such cases is similar to that of primary of lesions in such cases is similar to that of primary tuberculosis i.e. with involvement of hilar lymph nodes rather than cavitary and apical in the lung. In addition opportunistic infection with M. avium intracellular can occurs in cases of AIDS. FATE OF SECONDARY PULMONARY TUBERCULOSIS 10: The sub apical lesions in lungs can have the following courses. 1. The lesions may heal with fibrous scarring and calcification. 2. The lesions may coalesce together to from larger area of tuberculous pneumonia and produce progressive secondary pulmonary tuberculosis with the following pulmonary and extra pulmonary involvements:
The cavity provides favorable environment for proliferation of tubercle bacilli due to high oxygen tension. The cavity may communicate with bronchial tree and becomes the source of spread of infection (open tubercle) the open case of secondary tuberculosis may implant tuberculous lesions on the mucosal lining of air passages producing endobroncial and endotracheal tuberculosis. Ingestion of sputum containing and intestinal tuberculosis. Complications of cavitary secondary tuberculosis are: Aneurysms of patent arteries crossing the cavity producing haemoptysis. Extension to pleura producing bronchopleural fistula. Tuberculous empyema from deposition of caseous material on the pleural surface. Thickened pleura from adhesions of parietal pleura. TUBERCULOUS CASEOUS PNEUMONIA11: The caseous material from a case of secondary tuberculosis in an individual with high degree of hypersensitivity may spread to rest of the lung producing caseous pneumonia.
Figure No- 11 B Tuberculous Caseous Pnemonia
II.MILIARY TUBERCULOSIS 11: This is lymphaematogenosis spread of tuberculous infection from primary focus or later stages of tuberculosis. The spread may occur at systemic organs or isolated organ. The spread is either by entry of infection into pulmonary vein producing disseminated.
Figure No-10 Fate of Secondary Pulmonary Tuberculosis
I.Fibrocaseous tuberculosis. II.Tuberculous caseouas pneumonia. III.Military tuberculosis. I.FIBEROCASEOUS TUBERCULOSIS 11: The sub apical area of tuberculous pneumonia undergoes massive central caseation necrosis which may. Either breaks into a bronchus from a cavity (cavitary or open fibercaseous). Remain as a soft caseous lesion without drainage into a bronchus or bronchiole to produce a non-cavitary lesion (chronic fibrocaseoouss tuberculosis.)
Figure No- 11 C Miliary Tuberculosis
Isolated organ lesion in different extra-pulmonary sites (e.g. liver, spleen, kidney, brain and bone marrow) or into pulmonary artery restricting the development of military lesions within the lung. The military lesions are millet seed-sized (1 mm diameter), yellowish, firm areas without grossly visible caseation necrosis.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
False positive tests usually manifest themselves as lesser reactions. These lesser reaction could indicate prior exposure or infection with other Mycobacteria or vaccination with BCG. However, in places were the vaccine is not used lesser reactions should be regarded as highly suspicious. False negative are rarer than false positives but are especially common in AIDS patients as they have an impaired CMI response, other conditions such as malnutrition, steroids etc. can rarely result in a false negative reaction.
Figure No- 12 Miliary Tuberculosis of the spleen.
CLINICAL FEATURE OF TUBERCULOSIS: The clinical manifestation in tuberculosis may be variable depending upon the location. Extent and type of lesions. However, in secondary pulmonary tuberculosis which is the common type. The usual clinical features are as under: 1.Referable to lung- such as productive cough, may be with haemoptysis, pleural effusion, dyspnoea, orthopnea etc. chest x-ray may show typical changes like pleural effusion, modularity, and military or diffuse infiltrates in the lung parenchyma. 2.Systemic feature- such as fever, night sweats, fatigue. Loss of weight and appetite. Long-standing and untreated cases of tuberculosis may develop systemic secondary amlyoidosis. Courses of death in pulmonary tuberculosis are usually pulmonary insufficiency, pulmonary haemorrhage, sepsis due to disseminated military tuberculosis, cor pulmonale or secondary amyloidosis. CLINICALLY IDENTIFICTION & DIGNOSIS OF TUBERCULOSIS 13T he diagnosis of T.B requires detections of acid-fast bacilli in sputum via the Ziehl-Neelsen methods as previously described. The organism must then be cultured from sputum, first the sputum sample is treated with NaoH. This skills other containing bacteria but does not kill the M.TB. Present because M.TB. Is resistant to alkaline compounds by virtue of its lipid layer. The media used for growth and the resulting colony morphology have been described previously. However; methods of culturing can take 4-6 weeks to yield visible colonies. As a result; another method is commonly used call the BACTEC system. The media used in the BACTEC system contains radiolabeled palmitate as the sole carbon source. As M.TB, multiplies, it breaks down the palmitate and liberates radio- labeled CO2, using the BACTEC system, M.TB. Growth can be detected in 9-16 days vs. 4-6 weeks using conventional media. Skin testing is performed as the tuberculin or Mantoux test. PPD (purified protein derivative.) is employed as the test antigen in the Mantoux test. PPD is generated by boiling a culture of M.TB, specifically old Tuberculin (OT), 5TU (Tuberculin units), which equals 0.0001 mg of PPD; in a 01 ml volume is intracutaneously injected in the forearm. The test is read within 48-72 hours.
SYMPTOMS As stated, symptoms can vary depending on which part of the body is infected. Tuberculosis can infect almost any part of the body including, but not limited to, the lungs, heart, brain, bone, spine, stomach, kidneys, and fallopian tubes. The specific symptoms depend on the area of the body infected. Some general symptoms include weight loss, loss of appetite, low- grade fever, night sweats, and fatigue. Pulmonary Tuberculosis Occurs when the organism infected a cough, which may be dry or productive of phlegm. Often, there is coughing up of blood. An examination may not reveal any significant abnormalities. Occasionally, the doctor may detect the presence of fluid collection in the lungs. Tuberculosis Meningitis Is a tuberculosis infection of the brain or spinal cord? Symptoms may start with irritability and restlessness. Eventually, the patient develops stiff neck, headache, vomiting, seizures, and changes in mental condition in mental condition or behavior, or coma. Intestinal Tuberculosis Is an infection of the intestinal tract? It was not very common in the United States until AIDS; some of the symptoms include stomach pain, Diarrhea, Intestinal Obstruction, granuloma formation, intestinal ulceration with bleeding, or narrowing of the intestines. Tuberculosis lymphadenitis Involves M.Tuberculosis infecting the lymph nodes, causing enlargement of the nodes and forming masses in the neck. This is known as scrofula, and may sometimes drain to the skin. Tuberculosis Pericarditis Occurs when the organism invades and infects the lining of the heart. This can cause fluid build-up around the heart, leading to more significant problems, including shortness of breath, fluid build-up in the lungs, low blood pressure, are even death. Tuberculosis peritonitis Involves an infection and fluid build-up in the abdomen. This is often very difficult to diagnose and is often missed. In addition to build-up of fluid in the abdomen, symptoms may include fever, weight loss, and weakness. Even with testing of the fluid, it is difficult to diagnose and may necessitate Laparoscopy to confirm diagnosis. Tuberculosis salpingitis Is an infection of the uterine fallopian tubes that cause pelvic pain? Examination may reveal the patient may report irregular periods. it is not sexually transmitted. It is important to understand that many of these symptoms may also be present with numerous other medical conditions, quite often, Tuberculosis is not even suspected until other more common condition are treated without success. Cause As above, Tuberculosis is caused by Mycobacterium Tuberculosis, an organism found throughout the world. Respiratory droplets most often spread it person- to- person when people when people cough. Initially, the infection is acquired from another person. Once the organism enters the body. It spread via the bloodstream and lymph system throughout the body. This is called primary tuberculosis, and often there are no symptoms. The immune system fights off the infection, destroying the majority of organisms. Some become dormant and survive within the body for years or even decades. These organisms usually do not cause any problems. However, in a few cases, reactivation of the disease occurs. This does not require any new infection. The organism, dormant and inactive for years, has become active again.
Figure No 13- Administering the Mantoux test. CDC.
ADMINISTERING THE MANTOUX TEST- CDC. The test is considered positive if the diameter of the resulting lesions is 10 mm or greater. The lesions is characterized by erythma (redness) and swelling and indurations (raised & hard) 90% of people that have a lesions of 10 mm or greater are currently infected with M.TB. Or have been previously exposed to M.TB. 100% of people have a lesions of 15mm or greater are currently infected with M.TB. Or have been previously exposed to M.TB.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
The risk of reactivation increases if the immune system is weakened for any reason. On average, a normal person who has been infected with tuberculosis has about a 10% chance of developing a reactivation of the disease over the course of their lifetime. In people with HIV, however, they have a risk of about 7% per year. In the past, it was thought that almost all adult cases of tuberculosis were due to reactivation. However, newer testing methods have revealed that a sizeable number of adult cases may actually be due to newly acquired infections, especially in areas where there are a large number of people with tuberculosis. People from certain parts of the world, such as the Philippines, china, Southeast Asia, Haiti, and India have a much higher risk of having resistant tuberculosis. Resistant tuberculosis occurs when the organism is not sensitive to the usual anti-tuberculosis medicines. LABORATORY DIAGNOSIS OF TB: A) SKIN TESTS: REAGENTS: 1.OLD TUBERCULIN (OT): Kochs old tuberculin is a crude preparation of a 6-8 week culture filtrate of tubercle bacilli grown in 5% glycerol broth concentrated by evaporation on a heated water bath. 2.PURIFIED PROTEIN DERIVATIVE (PPD): A purified preparation of active tuberculoprotein has prepared by Sichert (1941) from old culture by precipitating with 50% ammonium sulphate. This standardized and stable antigen as purified protein derivative (ppd) is now generally employed for allergic skin tests instead of OT. .METHOD: The tuberculin tests are based on reaction to intradermal inoculation of tuberculins. 1. This is the method of choice and performed by intracutaneous injection of 0.1 ml of PPD into flexor aspect of forearm. B) HEAF TEST: It makes use of multiple puncture apparatus; which pricks the skin through a film of tuberculin. RESULT: Result is read within 48-72 hrs after intradermal injections of 0.1 ml PPD. 1.POSITIVE TEST: In a positive reaction there is a local oedema (indurations) of 10mm diameter surrounded by erythema at the site of injection. Positive test confirm past infection by tubercle bacilli but does not indicate present active stage of the disease. 2.FALSE NEGATIVE RESULT: The test may become negative in tuberculosis patients with military tuberculosis. C) BACTERIOLOGICAL DIAGNOSIS: SPECIMENSpecimen is collected from the suspected site of lesion. Pulmonary tuberculosis-sputum. Meningitis-CSF. Bone and joints- aspirated fluid. Renal- three consecutive morning sample of urine. DIRECT MICROSCOPY : Smears made from the specimen in new glass slides are stained by ZiehlNeelsen method. The acid-fast bacilli appear as pink brightened rods. Smears stained by fluorescent stains such as auramine phenol or aura mine rhodamine are examined under UN light the bacilli appear as bright rods against dark background. CONCENTRATION OF SPECIMENS : The bacteria are decontaminated and concentrated in a small volume without inactivation. Such concentrate is mostly used for culture and animal inoculation test and sometime for smear examination. METHODS IN USE: 1.PETROFFS METHOD: Sputum mixed with equal volume of 4% sodium hydroxide is infected at 37c for about 30 min. the mixture is frequently shaken till it gets liquefied and become clear. Sodium hydroxide also kills the contaminating bacteria. After centrifugation at 3000 r. p. m. for 30 mins. It is neutralized with 8% HCL in presence pf a drop of phenol red indicator. The deposit is used for smear, a culture and animal inoculation. AIM OF TREATMENT: To cure the patient of TB. To prevent death from active TB or its late effects. To prevent relapse of TB To decrease transmission of TB to others. To prevent of development of acquired drug resistance. It is vital to achieve these aims while preventing the selection of resistant bacilli in infection patients. The therapy of tuberculosis has undergoes remarkable chance during last two decades. The conventional 12-18 months treatment has been largely replaced by more effective and less toxic 6 months treatment, which also yield higher completion rates, i.e. better compliance. VACCINES: Anti-tubercular vaccines were developed much before the development of anti-tubercular TB drugs to prevent incidence or to build immunity against TB but such vaccines have significant failures too. E.g. BCG vaccine. a. STRAINS OF BCG VACCINE: Albert Calmettte and Calmette Guerin (1921) prepared an attenuated strain of M.bovis by growing it to potato medium for 13 years (1908-1921). When stain proved incapable of producing TB in susceptible guinea pig. It was named Bacilli Calmette Guerin (BCG). b.DOSE AND ADMINISTRATION: It is available in liquid and lyophilized from. The lyophilized vaccine is reconstituted by sterile physiological saline solution to make final concentrating of 0.1mg in 0.1 ml of vaccine. Vaccine once reconstituted should be utilized within 3-6 hrs. Administration by oral route. It is now given intradermally. c.AGE OF VACCINATION : It should be administered soon after birth or any time during the first year of life. d.OBSERVATION : A popular develops at the site of vaccination after 2-3 weeks after intradermal injection, which increase slowly and in about five weeks it break into shallow ulcer, which heals up leaving permanent round scar. Such individual becomes tuberculin positive after 4-6 weeks. e.PROTECTIVE EFFICACY: Major Field trial of BCG vaccine was undertaken in different countries before 1970 and result varied greatly ranging from 0 to 80%.
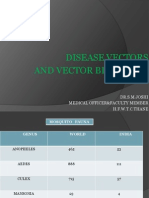
REGION North American Indian Great Britain Chicago, USA. Puerto, Rico. South India (Bang lore) Georgia & Alabama, USA. Georigia, USA. Illinois , USA South India (Chinglepur) AGE RANGE (YEARS) 0-20 14-15 Neonates 1-13 All ages >5 6-17 Young adult All age PROTECTION % 80 78 75 31 30 14 0 0 0 YEAR OF COMMENCEMENT. 1935 1950 1937 1949 1950 1997 1950 1947 1968
2.HOMOGENISATION METHOD: The specimen is treated with diluted acids as 8% sulphuric acid.3% hydrochloric acid or 5% oxalic acid then clearing the acid by repeated washing with sterile normal saline. 3.TRISODIUM PHOSPHATE METHOD: Trisodium phosphate is lethal for many contaminating bacteria but tubercle bacilli remain unaffected. SENSITIVITY TESTING: The isolated tubercle bacilli is tested for drug sensitivity in Dubos medium or L J medium after incorporating different concentrations of anti-tubercular drugs in the media before inoculation. PREVENTION AND TREATMENT-
The difference in protection appears to be related to exposure of individual to environmental mycobacteria that had already occurred before BCG vaccination. The variation in protection may also be contributed by some other factors such as virulence of organism in different communities and potency of vaccines. PRINCIPLE ROLE OF BCG: Vaccination does not give absolute protection against tuberculosis. Vaccines prevent serious forms of primary tuberculosis such as meningitis, skeletal TB and military spread of disease.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
B) CHEMOTHERAPUTIC AGENTS: M.Tuberculosis can cause chronic and fatal condition in humans known as tuberculosis. No effective chemotherapeutic agent was available for treating. TB as late as1940.The discovery of p-amino salicylic acid by Bernhein in 1941 was the first step in the development of effective anti-TB therapeutic agents. Remarkable progress has been made in the last 45 years. In 1943, anti-TB research resulted in the discovery of active anti0TB antibiotic, Streptomycin.A number of clinically useful drugs have been discovered since 1940s, including isoniazid (1952), pyrazinamide (1952), cycloserine (1952) ethionamide (1950), rifampin (1971), ethambutol (1962). Drugs used to treat TB disease. From left to right isoniazid, rifampin, pyrazinamide, and ethambutol. Streptomycin (not shown) is given by injection. CDC. Since the successful introduction of Rifampicin in the early 1970s as the AntiTB drugs, TB control and treatment were largely successful during 1970s as the combined use of available drugs. This led to negligible of TB research due to less interest and less market. No new drugs were developed during the last thirty years. Though there were continuously increased since 1980s report of incidence of TB and Multi-drugs resistance TB (MDR-TB) and even co-infection with AIDS. The world health organization declared emergency in TB on 1993. Increasing report of MDRTB since 1990s have posed a serious threat to mankind again as there will be no remedy or treatment of TB in man again in the face of war or challenge of mycobacteria of MDR-TB. PROFILE OF CURRENTLY AVAILABLE DRUGS FOR TB: Many drugs are selectively active against tubercle bacilli (TB) while some inhibit other microbes as well, though their use is primarily limited to TB. FIRST LINE: These drugs have high antitubercular efficacy as well as low toxicity
OH
Drug Isoniazid ( INH) Streptomycin ( SM)
Adverse effects Hepatitis, Peripheral Neuropathy, Hypersensitivity. Ototoxicity, Nephrotoxicity.
Route of administration Orally, Parent rally. Intramuscularly, intradermally.
Resistance Resistance is by mutation of the of catalase peroxidase gene so that the bacilli generate the active metabolite of isoniazid. Many drugs develop rapid resistance to streptomycin either by one step mutation or by acquition of plasmid, which codes for inactivating enzymes. Resistance to ethambutol develops slowly, in many cases due to alteration in the drug target gene. Rifampin resistance is nearly always due to mutation in the repo B gene (the target of rifampin action) reducing its affinity for the drug. Resistance develops rapidly if it is used alone, & is due to mutation in the gene which encodes for the enzymes generating the active metabolite of pyrizinamide.
Ethambutol ( Emb) Rifampin (Rmp)
Optic neuritis and hypersensitive. Hepatitis, fever, thrombocytopenia.
Orally.
Orally.
Pyrizinamide (pzm)
Hepatotoxicity, Hyperuricemia.
Orally.
II. Second line agents:
Drug p-amino salicylic acid (PAS) Kanamycin Structure a b Mecanism of action Inhibit respiration of M. tuberculosis. Aminoglycosides like kanamycin irreversibly bind to specific 30S-subunit proteins and 16S rRNA. Specifically Kanamycin binds to four nucleotides of 16S rRNA and a single amino acid of protein S12. This interferes with decoding site in the vicinity of nucleotide 1400 in 16S rRNA of 30S subunit. Inhibit peptide synthesizing M.TB by blocking the incorporation of amino acids containing sulphur (cysteine, Methionin.) Active against drug resistant strains of M.tuberculosis. Inhibition of protein synthesis.
Ethionamide Cycoloserin Caprepmycin
O OH
c d e
H2NH2C
O HO H2N HO OH HO O
NH 2
NH 2
SECOND LINE: These drugs have low antitubercular efficacy or high toxicity or both. 1. FIRST LINE AGENTS:
Drug Isoniazid (IHD) Streptomycin (Sm) Ethambutol ( Emb) Rifampin (Rmp) Pyazinamide (Pzm)
CO NH NH 2
a
4-am ino-2 -h ydroxyb enzoi c acid
NH2
HUH2C HO
OH
b c
C 2H5
Structure a b c d e
Mechanism of action Mycolic acid synthesis is inhibited resulting in loss of some areas of outer membrane and thinness of the cell wall. Inhibition of enzymatic polymerization of amino acids i.e. bactericidal. Prevent synthesis of protein and DNA and reduces RNA synthesis Inhibit DNA-directed RNA synthesis. Active against drug resistant strains of M. tuberculosis.
H 2N NH OH
3-ethylbenz othioamide
NH2
O NH H 2N O
H N H H H
H H H H N H O H N H H H O N H H H N H N N H O N H O N H H H N H H
4 - am i n o i s o x a zo l i d i n -3 - o n e
d
OH
H
H N
HN H N
NH OH OH
H H H O H
O H N
i sonicoti nohydrazi de
NH2 H 3C HO
O CHO
N H HO
a b
H H H
O H O H2 C HO OH NHCH3
c
O NH
2
H H
H H N H H HH H N H H H O
H H H H H H N H N N H H H H H H H N H H H H H H H
H H H H H H H
H H H H H H O H O H H H O H O O H H H O O H H H H H O H H H H O O O H H H O
Drug
N N
Adverse effects GI intolerance, Hepatotoxicity, Hypersensitivity, Fluid retention. Ototoxicity, Nephrotoxicity, Ototoxicity, Nephrotoxicity, Hypersensitivity. Hepatotoxicity, Hyperuricemain. Ototoxicity, Nephrotoxicity.
Route of administration. Orally. Intramuscularly. Orally. Orally. Intramuscularly.
P-amino salicylic acid ( PAS) Kanamycin Ethionamide Cycoloserin Caprepmycin
p y r az i n e- 2 - ca r b o x a m i d e
e
Journal of Pharmacy Research Vol.4.Issue 7. July 2011 2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
DOTS THEROPY14: Sputum smear microscopy provides definitive diagnosis. It is easy to perform, is replicable and cost effective. If good diagnosis practices are followed. It is expected that more than 50% of the new pulmonary TB patients will be smear positive. Chest X-ray examination, though sensitive, is not specific and has a wide inter-observer variability. The tuberculin test gives only evidence of infection and does not differentiate between infection and disease. ESR is also not specific and is unreliable as a tool for diagnosis or evaluation. Culture of sputum is highly sensitive and specific, but it is costly, not freely available and takes a long time in reporting. Other new investigation are not reliable, are expensive and not useful in tackling a public health problem like TB. The high false positivity (non- TB patients getting diagnosed as TB) and low replicability (repeated tests giving different results.) are the factors which make newer tests inferior to sputum smear examination. Besides, the high specificity of sputum microscopy (only actual TB cases getting diagnosed as positive) almost eliminates the chance of a non-TB patients getting treated for TB. Domiciliary chemotherapy has been proved to be as effective as sanatoria treatment. Studies in the India have shown that TB patients do not get any additional benefit by bed rest or special diet. The risk of infection among contacts of patients does not increase with domiciliary treatment and there is no need for hospitalization for most patients. The economic burden on society is also lowered by domiciliary treatment. Several studies in India by reputed researchers have shown that six months of chemotherapy gives favourable results when compared with longer terms of treatment for new sputum positive TB patients. It has also been proven that eight months of treatment is adequate for patient undergoing retreatment. These durations of treatment are adequate to prevent emergence of drug resistance. Short-course chemotherapy (SCC) is therefore more convenient and economical than convectional treatment with longer duration. In addition the shorter period of time makes direct observation more feasible and improves patient adherence to treatment. Fully intermittent chemotherapy has been found to be as effective as daily chemotherapy. Studies in animal models demonstrated that for Isoniazid, Rifampicin, And Pyrazinamide, intermittent dosing actually increased the efficacy of treatment. In vitro experiments demonstrated that, after a culture of M. tuberculosis is exposed to certain drugs for some time, it takes several days before new growth occurs ( The lag phase ) all the commonly used anti-TB drugs induce lag phases ranging from two days to forty days. Therefore these drugs can be given intermittently; intermittent regimens make treatment observation more feasible and convenient for DOT relapse rates. As the quality of drugs consumed is less, adverse reactions and costs are allowing organisms to re-enter the active metabolite phase in which the bactericidal drugs are more effective. Direct observation of treatment (DOT): Ensures the best possible results in treatment of TB. Here an observer watches and assists the patient in swallowing the tablet, thereby ensuring that the patient receives the medication. Many patients who do not receive directly observed treatment stop taking drugs after two months because they feel better. Studies in India and many other countries consistently shows that at least one third of patients do not take medicines regularly. It is neither possible to predict who these patients will be nor to reliably prevents during the entire course of treatment health education. Studies have shown that there will be poor treatment outcomes and high death rates in the absence of direct observation, even when regular supply of drugs is ensured. Hence, by observing the patients during the entire course of treatment, one ensures that they right drugs, in the right doses, at the right intervals and fore the right duration. The bacillary sub-population in TB is of four kinds and different drugs act on different kind of bacteria. These are tabled below:
TYPE OF TB BACILLI Extra-cellular rapidly multiplying Extra-cellular intermittently multiplying/ semi-dormant Intra- and extra-cellular acidic environments intermittently multiplying/semi-dormant. Dormant. EFFECTIVE DRUGS Rifampicin, Isoniazid, Streptomycin, Ethambutol. Rifampicin. Pyrazinamide. No drug.
Figure No-14 DOTS Theropy
DOTS (Directly observed treatment, short- course chemotherapy.) The essential principles of DOTS were first demonstrated in India. The determine that tuberculosis patients need not be hospitalized and the necessity treatment was first proven at the tuberculosis research center in Chennai in the 1950s and 1960s. The key to the success & DOTS strategy is that is places the responsibility for curing TB patients on the health workers not the patient on the health workers not the patients. This strategy proven successful through out the than 550 million people with cure rate of more than 90%. COMPONENTS OF DOTS : A DOT is a systematic strategy having 5 components: Political and administrative commitment. Good quality diagnoses, primarily by sputum smear microscopy. Uninterrupted supply of good quality drugs. Directly observed treatment (DOT). Systematic monitoring and accountability. Political and administrative commitment: TB is the leading infectious cause of death among adults. As TB can be cured, and the epidemic reversed, it warrants topmost priority. TB control has been given this priority by the Government of India as well as the state, district and local governments and administration. Good quality diagnosis : Diagnosis of TB is made primarily by sputum smear microscopy among chest symptomatic patients attending health facilities. This policy allows effective diagnosis in all setting and appropriate prioritization of efforts. Sputum microscopy is a reliable, simple and cost effective test. Good quality drugs: An uninterrupted supply of good quality anti-TB drugs must be available. In the revised national TB control programme (RNTCP).A box of medication containing the entire course of treatment is earmarked for each patient, ensuring the availability of drugs for the full course of treatment. Hence in RNTCP, the treatment never fails on account of non-availability of medicines. Short- course chemotherapy given in a programme of direct observation: The RNTCP uses the anti-TB drugs available. But, unless these drugs are consumed properly by the patient, the treatment will fail. This is why the heart of the DOTS strategy is Directly Observed Treatment (DOTS) in which a health worker or a trained person watches which the patient swallows the medicines. This simple principle ensure adherence, helps prevent drug resistance to anti-TB medicines and achieves high cure rates. Systematic monitoring and accountability : Quality of treatment is monitored by 1) Follow-up sputum examinations during and at the treatment, and 2) By using a robust and comprehensive recording and reporting system that evaluates and monitors the outcomes the outcomes of every patient on treatment. This is carried out by trained supervisory staff in the programme. Sputum smear conversion rate, cure rate and other key indicators are monitored at different levels. If a defined area is not achieving 90% sputum smear conversion rate at the end of three months and 85% cure rate, supervision is intensified. In RNTCP, the patient is the VIP . RNTCP has shifted the responsibility for cure from the patient to the health system. SCIENTIFIC BASIS OF DOTS : DOTS is primarily based on sputum microscopy, domiliary treatment, short course chemotherapy, and directly observed treatment.
The phenomenon of Persisters explains to some extent why all bacilli are not killed during treatment. Relapse with drug-susceptible organisms after the end of treatment or endogenous reactivation may be bacilli that have persisted in residual lesion for a long time in a semi-dormant/ dormant state.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
Currently recommended treatment regimens aim to: Cure the patient. Prevent death from active disease or form its late effects. Prevent the emergence and spread of drug-resistant organisms. Minimum relapse. Protect the community from continued of infection. All treatment regimens consist of two phases: INTENSIVE PHASE (IP): Aims for a rapid killing of bacilli. This means a shorter duration of infectiousness (d2 weeks), usually with rapid smear conversion (80%-90%) after 2 to 3 months of treatment. Each dose in this phase should be directly observed to ensure adherence and involves 3 to 5 drugs depending on the category into which the patient has been placed. CONTINUATION PHASE (CP): Eliminates most residual bacilli and reduces failures and relapses. At the start of the CP, there are low numbers of bacilli and less chance of drug resistance mutants. Therefore fewer drugs are needed during this phase. NUMERICAL FACTOR: The number of tubercle bacilli in a patient varies widely with the type of lesion the patient has. Data shows that the number of bacilli in a medium- sized cavity communicating with the bronchi is about 10 (one hundred million) whereas, in an encapsulated nodular lesion of the same size with no bronchial communication. It can be as low as 10 (one hundred). The numbers are also low in extra-pulmonary lesions of the skin, lymph glands, meninges and bones. The larger the bacterial load, the higher is the probability that resistant mutant are present even before treatment has been initiated. EXTRA- PULMONARY TUBERCULOSIS (EP TB): The management of extra- pulmonary TB differs forms that of TB mainly due to the difficulty in making a conclusive diagnosis. This can lead to empirical treatment and thereby to over-diagnosis and unnecessary treatment of a large number of patients. EP TB is usually paucibacillary (with relatively less number of bacilli). Any treatment regimen of treatment, extra-pulmonary TB is classified into seriously ill and not-seriously ill forms (detailed under the section on treatment). The difficulty in establishing a clear-cut end-point of treatment in EP TB often leads to treating these patients for longer durations then required. Studies have clearly established the efficacy of short-course chemotherapy in children and adults. Intermittent regions in EP TB have also been proven to be as effective as daily regimens.
CATEGORIES OF TREATMENT:
CATEGORY OF TREATMENT Category I Category II TYPE OF PATIENT REGIMEN 2H3RZ3E3+4H3R3. 2H3R3Z3E3S3+ 1H3R3Z3E3+5H3R3E3.
Isoniazid, Rifampicin, Pyrazinamide and Ethambutol, given for two months (8 weeks: 24 doses). At the time of the 22 dose, the patients is referred for follow-up sputum examination so that the result are available by the end of IP ( 24 dose), if follow-up sputum examination is negative, CP is started and consists of 4 months of treatment ( 18 week; 54 doses) with Isoniazid and Rifampicin, given three times a week is directly observed. Alternate days. During CP. at least the first dose two months into the start of and at the end of CP. If the sputum smear is positive after 2 months of treatment, IP drugs are extended for another one month (12 doses from a prolongation pouch) before starting CP. A follow up sputum examination is repeated at the extended IP (3 months). This helps in assessment of the progress of treatment and sputum conversion rate. Irrespective of the smear status, the patient is put on CP drugs and next follow up sputum examination is done at 5 months. If the sputum smear is positive after 5 months or more of started treatment, the treatment outcome of the patient is declared as failure and (s) he is started afresh on CAT II treatment. in the rare situation in which a CAT I smear-positive patient has a negative sputum after 2 months of treatment and a positive sputum smear after 4 months of treatment , another sputum smear should be examined at 5 months. If this is also positive, the patient is considered a treatment failure and is started afresh on CAT II treatment. CATEGORY II: This is used to treat retreatment cases namely relapse failure treatment after default and others. Such patients are generally sputum smear-positive, the IP consists of two months (8 week: 24 doses) of Isoniazid, Rifampicin, Pyrazinamide, Ethambutol and streptomycin; all given under directs observation three times a week on alternate days. This is followed by another one months (4 week; 12 doses) of Isoniazid, Rifampicin, Pyraziamide and Ethambutol, all of which are given under direct observation three a week on alternate days. This is immediately followed by CP, which consists of 5 months (22 weeks, 66 doses) of Isoniazid, Rifampicin and Ethambutol given three a week on alternate days. The first dose of every week being directly observed. If the sputum smear is positive after 3 months of treatment, the four oral IP drugs are continued for another one month (4 week, 12 doses) before starting the 5months CP. Patients who have been previously treated are at an increased risk of having drug resistant bacilli. For this reason, such patients are given a more intensive regimen, namely CAT II. Experience in India and elsewhere has shown that CAT II treatment, if taken regularly by the patient, is effective and result in curing in most patients. Patients who relapse generally have better outcomes than those who are failure or treatment after default cases, but even these latter types of patients respond well to treatment, provided them it regularly and are well supervised. CATEGORY III: This is used for patients who are smear- negative PTB or EP TB, and are not seriously ill. The IP lasts for 2 months (8 weeks; 24 doses) with Isoniazid, Rifampicin, and And Pyrazinamide given under direct observation three times a week on alternate days. This is followed by CP, which consists of 4 months (18 weeks: 54 doses) of first dose of every week being directly observed. If a patients receiving CAT III regimen has a positive sputum smear at any stage of the treatment, (s) he should be declared a failure, re-registered, and treated afresh with the CAT II regimen.
TREATMENT REGIMEN:
CATEGORY OF TREATMENT Category I 1) Intensive phase. PHASE TREATMENT 2 months PERIOD & DRUG REGIMEN
Category III
New sputum smear-positive. Seriously ill **new sputum smear-negative. Seriously ill** new extra-pulmonary. Sputum smear-positive relapse Sputum smear-positive failure Sputum smear-positive treatment after default Other*** New sputum smear-negative, not seriously ill New extra-pulmonary, not seriously ill.
2H3R3Z3+4H3R3.
The subscript after the letters refers to the number of dosage per week. The dosage strengths are as follows: H: Isoniazid (600mg), R: Rifampicin (450mg), Z: Pyrazinamide (1500mg), E: Ethambutol (1200mg), S: Streptomycin (750mg). ** Seriously ill also including, any patient, pulmonary or extra-pulmonary who is HIV positive? *** In rare and exceptional cases, patients who are sputum smear-negative or who have extra-pulmonary disease can have Relapse or Failure.
The codes and dosage strengths:
MEDICATION ISONIAZID RIFAMPICIN PYRAZINAMIDE ETHAMBUTOL STREPTOMYCIN DOSE(THRICE A WEEK) 600 mg 450 mg 1500 mg 1200 mg 0.75 mg NUMBER OF PILL IN COMBIPAKE. 2 1 2 2 _
2) Continuous phase. 4 months Category II 1) Intensive phase. 3 months
2) Continuous phase. 5 months. Category III 1)Intensive phase 2)Continuous phase 2 months. 4 months
CATEGORY I: This is used for new patients who are sputum smear-positive or seriously ill sputum smear-negative or seriously ill EP TB patients. Treatment is given in two phases intensive phase (IP) and continuation phases (CP). IP consists of
Isoniazid- 2 tab of 300 mg rifampicin- 1 cap of 450 mg pyrazinamide- 2 tab of 750 mg ethambutol 2 tab of 600 mg. Isoniazid- 2 tab of 300 mg. Rifampicin- 1 cap of 450 mg. Isoniazid- 2 tab of 300 mg Rifampicin-1 cap of 450 mg. Ethambutol- 2 tab of 600 mg. Inj. Of streptomycin 0.75 g one inj alternate day only for 2 months. Isoniazid- 2 tab of 300 mg. Rifampicin - 1 cap of 450 mg. Ethambutol- 2 tab of 600 mg Isoniazid 2 tab of 300 mg Rifampicin- 1 cap of 450 mg. Pyrazinamide 2 tab of 750 mg. Isoniazid- 2 tab of 300 mg. Rifampicin 1 cap of 450 mg.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
TREATMENT OF REGIMEN OF TB: THE RELATIVE ACTIVITY OF FIRST- LINE DRUGS IN ACHIEVING THESE GOALS IS:
GOALS Early bactericidal Sterilizing Resistance prevention HIGH ING Rmp,Pzm. INH, Rmp MODERATE Rmp, Emb ING Emb, Sm LOW Sm, Pzm. Sm, Emb. Pzm.
The problem is multiplied due to increasing emergence of multi-drug-resistance strains of M. tuberculosis. Scince, 1980s and further complicated with TB in ADIS patient with less immune capacity making them more susceptible to infection. The problem is aggravated further due to our insufficient knowledge about the detail molecular mechanism of action of anti- TB drugs and on development of new effective better anti-TB drugs and on development of new effective better anti- TB drugs during last three decades. Though the Mycobacteria is gradually developing its own mechanism of living in presence of our arsenals (i.e the existing anti-TB drugs) by natural mutational changes. CURRENT RESEARCH PROGRAMS ON TB: Due to improper and incomplete implementation of prescribed drugs- regimens, the resurgence of TB particularly with drug resistant strains, the resurgence of TB particularly with drug resistant strains, the TAACF southern Research institute, P.O. Box 55305.Birmingham.AL. Is giving services to investigation for screening their anti- TB drug samples. Since the later of 1994, the TAACF has actively pursued comp for screening from academic, government agencies, and industry. The ongoing efforts of the TAACFcontinually reward the scientific community with valuable data on potential drug candidates with activity against tuberculosis. Word Health Organization (WHO) has declared emergency research in tuberculosis region and so it is motivating new researchers to work in this area by providing fund and facilities. Pharmaceutical companies like Lupine, Astra Zeneca, Haffkine. Wockhardt: Sadoz -novartis are seriously involved in research on TB and also helping new researchers. Many government funded research organizations and universities are also seriously involved in research on TB, its prevention, control and treatment through various programs. STRATEGIES FOR ANTI MYCOBACTERIA: 1)Analogs and derivatives for existing and their SAR Improved therapeutic index Activity against drug sensitive strains Improved bioavailability Better tolerance and safely pharmacokinetics. 2)Broad Screening Novel mode of action 3) Target directed Mycobacterial specific targets E.g. Arabinomannan, liporabinogalactan, and Mycolic acid. GOALS OF THE PROGRAMS: 1)New anti- TB drugs preferentially for use against MDR TB. New mechanism of action 2) New anti TB drugs are more potent, selective and quicker acting Decrease over all treatment time Bactericidal activity 3) New anti TB drugs that can be effective in a drugs cocktail 4) Facilities early stage drug development 5) Encourge the development of research ideas relating to anti Mycobacteria drug Development New Molecules, Mechanism of action, Molecular biology, New targets, The Global Alliance for TB drug development is interested in forwarding rube loses drug development projects throughout the R & D process, but is specifically interested in drug discovery (preclinical)projects clinical development projects. The Alliance recognizes three primary reasons why new TB drugs are needed specifically. Shorter and more easily administered treatments improved treatment of patients with MDR TB More acceptable and effective treatment of high risk patients with latent TB infection. DRUGS UNDER DEVELOPMENT: It is recommended that the compounds listed below are worthy of further pursuit by global R & D community. A) DISCOVERY RESEARCH: Thiolactomycin analogues. SWOT analysis.
CONVENTIONAL REGIMEN: These consist of INH+Tzn (Thiacetazone) or Emb with or without Sm (for initial 2 months) optimum result require 12-18 months. To improves compliance and to reduce treatment cost, after the initial 2 months of daily therapy as above drug (unhandy other) are given twice a week under supervision. SHORT COURSE REGIMENS: Trail of combinations of drugs with high bactericidal, sterilizing and resistance preventing activities have shown that duration of treatment can be reduced to 6-9 months. THE REGIMENS BEING USED ARE: Four drugs INH+ Rmp+ Pzn+ Emb or Sm daily 2 months, followed by 2 drugs INH+ Rmp daily for another 4 months, total 6 months.The above initial treatment followed by INH+ Tzn or Emb daily for another 6 months, total 8 months. This reduces cost of treatment.Thrice a week INH+R mp+ Pzm Sm or Emb under supervision for 2 months with INH+Rmp+Rmp thrice a week for another 4 months in continuation phase, total 6 months.Recently it has been shown that Sm/Emb can eliminate as a routine adjunct unless INH resistance is suspected. TREATMENT OF RESISTANT CASES: When sputum remains positive even after 6 months treatment with any regimen, resistant organisms are most likely present. THE CHOICE OF DRUGS DEPSNDS ON: Drug combination employed in the previous regimen. Dosage and regularly with which these drugs were taken. Presence of associated disease if any-leukemias, diabetes, ADIS. The NTP regimen for relapse & failure cases is INH+ Rmp+ Pzn+ Sm for 2 months then 4 drugs(-sm) for another 1 months and 3 drugs ( INH + Rmp + Emb) for next 5 months.( total 8 months) If sputum is found positive at 3 months, the 4 drugs therapy is extended by 1 month more. EXTRAPULMONARY TUBERCULOSIS: Fresh patient of abdominal, genitourinary, lymphatic bone/ joint, disseminated or meningeal tuberculosis are treated on the same lines with the same drugs on for pulmonary tuberculosis.INH, Pzn, Emb, Cys (Cycloserine) have very good CSF penetrability.In tubercle meningitis higher dose of INH (with pyridoxine cover) its used and Pzm is always included along with Rmp+ Emb or Sm. It is also advised to extend the total duration of treatment to 9 months. TUBERCULOSIS IN PREGNACY: INH, Rmp, Emb and possibly pzn are to the foetus. The standard 6 months INH+ Rmp (with pzn for initial 2 months) should be added during late but not early in pregnancy. TUBERCULOSIS IN ADIS PATIENTS: The standard short course regimen with INH+ Rmp (pzn + Emb for initial 2 months) Be extended to 9 months. Another regimen of INH + Rmp+ Emb for 6 months supplemented with pzn in the first 2 months has been found satisfactory. PROBLEMS DUE TO IGNORANCE: Our ignorance of molecular of molecular basis of pathogenesis of TB and virulence of causative and Mycobacteria is great. Mycobacteria are daunting organism to study. Inn contrast to the most commonly used organism for molecular biological studies, E. coli which produces a visible colon (10.7 bacilli) in about 8 hrs. M.tuberculosis requires 3 to 4 weeks to yield a comparable colony. It has a formidable waxy coat composed of multiple complex lipids and carbohydrates that renders it impermeable to many common drugs. The bacilli tend to clump, which makes working with them and quantitation of them is difficult, Because of its ability to remain dormant working for a long time after infection and sudden activation due to unknown reasons, researchers avoid working with Mycobacterium out of fear of being contaminated and infected. Current bio safety regulations require that work with is expensive and not widely available. Hence, research the pathogen is slow and demanding.
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Nilam A.Gadhave et al. / Journal of Pharmacy Research 2011,4(7),2107-2119
STRENGTHS Synthetic routes to thiolactomycin and analogues have been developed.The mechanism of action is known. Active against isoniazid- resistant strains. Well absorbed orally. OPPORTUNITIES Both pharmas and academia are pursuing inhibitors of FAS-II and progress might be accelerated by collaborating with GATB/TDR. WEAKNESSES No report of in vivo activityM. tuberculosis. Present molecule is chiral cost. Implications if analogues also chiral. THREATS Unknown at this stage.
GEMIFLOXACIN SWOT analysis;
STRENGTHS Potent 4th generation fluoroquinolone. Well absorbed and tolerated in man. OPPORTUNITIES Collaboration with GATB/WHO might encourage SKB or LG chemicals to generate more definitive TB data. WEAKNESSES No in vivo TB data. Data from healthy volunteers suggest difficulty in reaching a therapeutic dose for TB. THREATS Many other quinolones either in development or marketed already.
Mefloguine/halofantrine analogues. SWOT analysis.
STRENGTHS More potent in vivo than ethambutol. Likely to have less toxicity than ethambutol. OPPORTUNITIES Progress might be accelerated by collaborating with GATB/TDR. WEAKNESSES Cytostatic action. Parent molecule is chiral-cost implications if analoguesalsochrial THREATS Unknown at this stage.
T-3811ME. SWOT analysis:
STRENGTHS Potent, broad-spectrum quinolone lacking 6-F atom present in all other 3rd /4th generation fluoroquinolones. Progressing into phase III trial so presumably well absorbed and tolerated in man. OPPORTUNITIES Collaboration with GATB/WHO might encourage Toyoma or BMS chemicals to generate more TB data. WEAKNESSES No in vivo TB data. No ADME data in public domain. THREATS The company has indicated a lake of enthusiasm for developing the drugs for a TB indication.
B)PRECLINICAL DEVELOPMENT: CALANOLIDES A AND B. SWOT analysis.
STRENGTHS Possible dual role in treating TB and ADIS. Synthetic route developed to calanolide A and analogues calanolide B readily obtaibale B readily obtaibale from renewable natural sources. No cross- resistant with rifampicin or streptomycin. OPPORTUNITIES Collaboration with GATB / WHO could induce Sarawak to proceed with the TB indication. WEAKNESSES For the TB indication, no I vivo efficacy. ADME or toxicity data
It was also recommended that the families of antifungal azoles, antibacterial nitroimidazole and oxazolidinones be further studied in the discovery research phase in an identify molecules with greater anti-TB potential than current candidates which have been discussed specifically in this report. The use of inhibitors of bacterial drug efflux mechanism and small molecules immunomodulators were also felt to be areas worth investigation further in order to identify agents as possible adjunts to existing TB drug regimen. FUTURE DIRECTION IN TB RESEARCH: New approaches for discovering new, more selective anti- TB agents the mapping of M. tuberculosis genome, the delineation of the pathways in Mycobacteria call wall biosynthesis (e.g. glycosylation, pathway, fatty acid biosynthesis, diaminopimelic acid biosynthesis ) , the discovery of genes involved in latency and virulence and the application of DNA micro-array technology to M.tuberculosis. Application of combination chemistry and high throughout screening to antiTB drug discovery promises to greatly accelerate the drug discovery process. Training to increase the number and improved delivery methods will be integral parts of a strategy to full control future outbreaks of TB, particularly MDRTB which has severely challenge the limited number of effective treatment options. To develop and review national TB control proramme plans based on the DOTS strategy. To build capacity to implement, monitor and evaluate national TB control programmers. To evaluate cost- effectiveness and impact of TB control interventions. To develop and implement interventions to combat the dual TB and HIV/ ADIS epidemic (in close collaboration with ADIS control programmers. REFERENCES
1. 2. Replika press pvt. Ltd. Nerala Delhi, 4th Ed, 1999, 65-66. Tortora, Berdell R. Funke, Christine L. Case, Microbiology an introduction, Addison Wesley Longman, Inc, California ; 6th Ed, 1998; 637-641. C. Dey, D. Sinha, M. Dey, Medical bacteriology including medical mycology and ADIS; New central book agency (P) Ltd, Calcutta: 17th Ed, 1999: 605-625. Ernest Jawetz, Joseph L. mellnick, Edward A. Adelberg, (Eds.), Review of Medical Microbiology, Large Medical Publication; Maruzen Company Limited, Japan; 7th Ed; 1966; 194-202. P. Chakra borty, a Textbook of Microbiology, New central book agency (P) limited Calcutta; 1st Ed, 1995; 351-365. K. D. Tripathi, Essentials of medical pharmacology; Jaypee brothers medical publishers (P) Ltd, New Delhi; 4th Ed; 2001, 752-763. R.S. Satoskar, S.D. Bhandarkar, S.S. Ainapure, Pharmacology and Pharmacotherapeuties; Popular Prakashan, Mumbai; 15th Ed, 2, 1997; 690-706. Manfred. E.Wolff Burgers Medicinal Chemistry and Drug Discovery ; volume 2- therapeutic agents; A Wiley interscience publication, John Wiley & sons, Inc. New York; 5th Ed 1996; 575-636. Harsh Mohan, Textbook of pathology; Jaypee Publication, New Delhi India, 4th Ed, 2002, 139-143. Wilson and Gisvolds, Textbook of organic medicinal and Pharmaceutical Chemistry; Lippincott Williams & Wilkins, Baltimore (USA), 11th Ed, 2004, 254-259. William David A. Lemke L., Thomas, Foyes principle of Medicinal chemistry; Lippinocott Williams and Wilkins, 5th Ed, 2002. F. S. K. Barar; Essentials of Pharmacotherapeutics; S. Chand & Company Ltd. Ram nagar New Delhi, 3rd Ed, 434-441. Literature Review of Central T.B. Division; Director General of health services; Ministry and family welfare. .H. Rang, M. Dale, J. Ritter, P. Moore, Pharmacology, Churchill Livingstone an imprint of Elsevier, 5th Ed, 2003, 649-951. t K. Park, Parks Preventive & Social Medicine, M/S Banarasides Bhanot Publishers Jabalpure, 15h Ed, 1998. Dr. P.S. Ghadi, Pathophysiology, Career Publication Nashik 1st Ed, 2000. J. Cappuccino, N. Sherman, Microbiology a laboratory manual, Replika press pvt.Ltd.Nerala Delhi,4th Ed,1999,65-66. S.S Kadam, K. R. Mahadik K. G. Bothara, Principles of Medicinal Chemistry, Nirali Publication Pune, 11th Ed, 1, 2003. 107-19.
THREATS Unless funds become available, Sarawak will concentrate on the ADIS indication.
QUINOLONES PD 161148 AND CS- 940 SWOT analysis;
STRENGTHS Potent bactericidal activity. Active against both quinolone-sensitive andresistant M. tuberculosis. OPPORTUNITIES Collaboration with GATB / WHO might induce pharmas toprogress the compoundsrapidly for TB . WEAKNESSES No in vivo TB efficacy, ADME or toxicity data available . From structural considerations, the molecules do not appear to be too metabolically robust. THREATS Numerous other quinolones are indevelopment.
POLOXAMER 315. SWOT analysis;
STRENGTHS Acts on microbes extra & intra cellularly. Synergises with other anti-TB drugs. IND obtained. OPPORTUNITIES Collaboration with GATB / WHO may encourage clinical progression for TB indication. WEAKNESSES Non-specific mechanism of action. Accumulation in tissues may be problematic with long treatment regimens THREATS None perceived.
3. 4. 5. 6.
C) CLINICAL DEVELOPMENT: MOXIFLOXACIN SWOT analysis
STRENGTHS Safe and well tolerated Excellent oral bioavailability & long 11/2 Already registered in Germany other approvals expected soon. OPPORTUNITIES Collaboration with GATB/WHO might encourage Bayer to generate clinical TB data. WEAKNESSES No clinical data for TB indication. THREATS Many other quinolones either in development or marked already.
7. 8. 9. 10. 11. 12. 13 14.
SITAFLOXACIN SWOT analysis;
STRENGTHS Potent 4th generation fluroquinolones. Well absorbed and tolerated in man. OPPORTUNITIES Collaboration with GATB/WHO might encourage indication. WEAKNESSES No in vivo TB data. THREATS The company has indicated a lake of enthusiasm for developing the drug for a TB Dalichi to generate clinical TB data.
15. 16. 17.
Source of support: Nil, Conflict of interest: None Declared
Journal of Pharmacy Research Vol.4.Issue 7. July 2011
2107-2119
Copyright of Journal of Pharmacy Research is the property of Journal of Pharmacy Research and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.
Vous aimerez peut-être aussi
- Interpretation of Up & Go Test For Older AdultsDocument1 pageInterpretation of Up & Go Test For Older AdultsMichael KuzbytPas encore d'évaluation
- Hypervolemia and Hypovolemia Nursing CareDocument2 pagesHypervolemia and Hypovolemia Nursing CareMichael KuzbytPas encore d'évaluation
- TB Standards 2007Document450 pagesTB Standards 2007Michael Kuzbyt100% (1)
- TelmisartanDocument2 pagesTelmisartanMichael Kuzbyt100% (1)
- Windshield Survey ToolDocument8 pagesWindshield Survey Toolkenneth_rhea100% (1)
- Oxycodone Hydro ChlorideDocument3 pagesOxycodone Hydro Chlorideapi-3797941Pas encore d'évaluation
- Interpretation of Up & Go Test For Older AdultsDocument1 pageInterpretation of Up & Go Test For Older AdultsMichael KuzbytPas encore d'évaluation
- Windshield Survey TemplateDocument6 pagesWindshield Survey TemplateMichael Kuzbyt100% (1)
- Windshield Survey ToolDocument8 pagesWindshield Survey Toolkenneth_rhea100% (1)
- Opioid Equianalgesic ChartDocument1 pageOpioid Equianalgesic Chartdamondouglas100% (7)
- Zocor SimvastatinDocument1 pageZocor SimvastatinMichael KuzbytPas encore d'évaluation
- RamiprilDocument3 pagesRamiprilMichael KuzbytPas encore d'évaluation
- VerapamilDocument2 pagesVerapamilMichael KuzbytPas encore d'évaluation
- Aminoxin: Clinical Medications WorksheetsDocument1 pageAminoxin: Clinical Medications WorksheetsMichael KuzbytPas encore d'évaluation
- VerapamilDocument2 pagesVerapamilMichael KuzbytPas encore d'évaluation
- BetamethasoneDocument3 pagesBetamethasoneMichael KuzbytPas encore d'évaluation
- Zopiclone clinical worksheetDocument2 pagesZopiclone clinical worksheetMichael KuzbytPas encore d'évaluation
- Atenolol drug guide for hypertension and anginaDocument2 pagesAtenolol drug guide for hypertension and anginaMichael Kuzbyt100% (1)
- Venlafaxine XRDocument2 pagesVenlafaxine XRMichael KuzbytPas encore d'évaluation
- Fall Prevention FactSheetDocument2 pagesFall Prevention FactSheetMichael KuzbytPas encore d'évaluation
- XareltoDocument2 pagesXareltoMichael Kuzbyt100% (1)
- IsoniazidDocument2 pagesIsoniazidMichael Kuzbyt100% (1)
- Aminoxin: Clinical Medications WorksheetsDocument1 pageAminoxin: Clinical Medications WorksheetsMichael KuzbytPas encore d'évaluation
- Interpretation of Up & Go Test For Older AdultsDocument1 pageInterpretation of Up & Go Test For Older AdultsMichael KuzbytPas encore d'évaluation
- LorazepamDocument1 pageLorazepamMichael KuzbytPas encore d'évaluation
- Ferrous GluconateDocument2 pagesFerrous GluconateMichael Kuzbyt0% (1)
- MMSE Interpretation of ResultsDocument1 pageMMSE Interpretation of ResultsMichael KuzbytPas encore d'évaluation
- Clinical Medications WorksheetsDocument2 pagesClinical Medications WorksheetsMichael Kuzbyt0% (1)
- Dipimide: Clinical Medications WorksheetsDocument2 pagesDipimide: Clinical Medications WorksheetsMichael KuzbytPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Techtalk August2010Document2 pagesTechtalk August2010Abu KhalidPas encore d'évaluation
- Preoperative Hair Removal A Case Report With Implications ForDocument32 pagesPreoperative Hair Removal A Case Report With Implications ForJasmine RogersPas encore d'évaluation
- Louis Pasteur (1822-1895)Document12 pagesLouis Pasteur (1822-1895)NercyPas encore d'évaluation
- Root Coverage PDFDocument24 pagesRoot Coverage PDFJason Pak100% (1)
- Question Bank Biology Class 12Document7 pagesQuestion Bank Biology Class 12Mᴀïᴢᴍɛɛŋ AŋꜱᴀʀïPas encore d'évaluation
- Multiple Sclerosis: A Guide to Causes, Symptoms and TreatmentDocument22 pagesMultiple Sclerosis: A Guide to Causes, Symptoms and TreatmentJemai O. Bico ÜPas encore d'évaluation
- Statistical Methods for Calculating Vaccine PD50Document1 pageStatistical Methods for Calculating Vaccine PD50Joshua WelchPas encore d'évaluation
- Trans Pulmopatho ColoredDocument8 pagesTrans Pulmopatho Colored2012Pas encore d'évaluation
- The Animal Rules 1962 MalaysiaDocument11 pagesThe Animal Rules 1962 MalaysiaMelissa GimballPas encore d'évaluation
- Intro To Parasitology PDFDocument4 pagesIntro To Parasitology PDFMatt M. MendozaPas encore d'évaluation
- HHS & Fda 1984Document4 pagesHHS & Fda 1984Heather X Rhodes100% (1)
- Amoxicillin Tri Hydrate Table FormatDocument2 pagesAmoxicillin Tri Hydrate Table FormatNico DonatoPas encore d'évaluation
- Exually Tran Mitted Disease: Rean Jane EscabarteDocument14 pagesExually Tran Mitted Disease: Rean Jane EscabarteRan Jung EscabartePas encore d'évaluation
- Edexcel GCE: Biology (Salters-Nuffield)Document16 pagesEdexcel GCE: Biology (Salters-Nuffield)jjjggg888Pas encore d'évaluation
- Specific Nursing Care Rendered in Hepatic Encephalopathy Contemporary Review and New Clinical Insights 2167 1168 1000264Document7 pagesSpecific Nursing Care Rendered in Hepatic Encephalopathy Contemporary Review and New Clinical Insights 2167 1168 1000264zeljko_vlaisavl4859Pas encore d'évaluation
- A Short Review of ImmunochemistryDocument6 pagesA Short Review of ImmunochemistryHauwa'u Abubakar MahePas encore d'évaluation
- Input 3 Assessment of Nutritional StatusDocument81 pagesInput 3 Assessment of Nutritional StatusRauell Rhaj SantosPas encore d'évaluation
- Toy Cleaning 1Document6 pagesToy Cleaning 1didikPas encore d'évaluation
- Red Biotechnology ProjectDocument5 pagesRed Biotechnology ProjectMahendrakumar ManiPas encore d'évaluation
- Inactivation of E Coli Mo157 h7 Listeria and SalmonellaDocument5 pagesInactivation of E Coli Mo157 h7 Listeria and SalmonellaadiazcalidadPas encore d'évaluation
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddlePas encore d'évaluation
- Synonyms Egg Drop, Egg Drop Syndrome 76, EDS-76Document17 pagesSynonyms Egg Drop, Egg Drop Syndrome 76, EDS-76rahma tamren100% (1)
- Yellow Fever FactsDocument2 pagesYellow Fever FactsFactPalooza100% (1)
- Disease Vectors and Vector BionomicsDocument16 pagesDisease Vectors and Vector BionomicsSuhas JoshiPas encore d'évaluation
- American Jurisprudence Proof of Facts 3d Database - Lyme DiseaseDocument76 pagesAmerican Jurisprudence Proof of Facts 3d Database - Lyme DiseaseMetacumet Bey50% (2)
- 2.5 - Regional Update: Latin AmericaDocument10 pages2.5 - Regional Update: Latin AmericaAqua LakePas encore d'évaluation
- DR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryDocument40 pagesDR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryPrincewill SeiyefaPas encore d'évaluation
- Pidato DBDDocument7 pagesPidato DBDLuh Putu SukmayantiPas encore d'évaluation
- Hiv Current Trend in The Use of HaartDocument19 pagesHiv Current Trend in The Use of Haartapi-3705046Pas encore d'évaluation
- Blood and Body Fluid SpillageDocument4 pagesBlood and Body Fluid SpillageSony AntonyPas encore d'évaluation