Vous aimerez peut-être aussi
- Implant SeminarDocument62 pagesImplant SeminarDr. Abdulsalam Awas Dental CenterPas encore d'évaluation
- Computer-Assisted Craniomaxillofacial Surgery: Sean P. EdwardsDocument18 pagesComputer-Assisted Craniomaxillofacial Surgery: Sean P. Edwardshasan nazzalPas encore d'évaluation
- Three Dimensional Imaging in DentistryDocument26 pagesThree Dimensional Imaging in Dentistrydorasani99Pas encore d'évaluation
- Small Pox: A Child Infected With SmallpoxDocument5 pagesSmall Pox: A Child Infected With SmallpoxJavee_Viccent__5618Pas encore d'évaluation
- Somniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeDocument58 pagesSomniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeSudheera RachamallaPas encore d'évaluation
- Pharmacology Neurotropic Drugs 2015Document44 pagesPharmacology Neurotropic Drugs 2015Migz BrosasPas encore d'évaluation
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- Triage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.Document73 pagesTriage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.ShrutiPas encore d'évaluation
- Dealing With Shift Work and FatigueDocument14 pagesDealing With Shift Work and FatigueA. AkbariPas encore d'évaluation
- Color Atlas of Temporomandibular Joint Surgery - QuinnDocument248 pagesColor Atlas of Temporomandibular Joint Surgery - QuinnAnonymous LnWIBo1G100% (2)
- AppendectomyDocument8 pagesAppendectomyDark AghanimPas encore d'évaluation
- An Investigatory Project ProposalDocument13 pagesAn Investigatory Project ProposalJeg B. Israel Jr.Pas encore d'évaluation
- GlossitisDocument7 pagesGlossitisLjubomirErdoglija100% (3)
- Clinical Maxillary Sinus Elevation SurgeryD'EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoPas encore d'évaluation
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsPas encore d'évaluation
- A Surgical Planning and Guidance System For High Tibial OsteotomyDocument11 pagesA Surgical Planning and Guidance System For High Tibial OsteotomyKiran Kumar KalyanamPas encore d'évaluation
- 2018 - Optimizing Accuracy in Computer-Guided Implant Surgery WithDocument5 pages2018 - Optimizing Accuracy in Computer-Guided Implant Surgery WithLenny GrauPas encore d'évaluation
- Image Guided Oral Implantology and Its Application in The Placement of Zygoma ImplantsDocument12 pagesImage Guided Oral Implantology and Its Application in The Placement of Zygoma ImplantsDenisa CorneaPas encore d'évaluation
- DownloadDocument22 pagesDownloadhasan nazzalPas encore d'évaluation
- Cat e ImplantesDocument5 pagesCat e ImplantesBlas García GarcíaPas encore d'évaluation
- Cirugia Asistida Por ComputadoraDocument18 pagesCirugia Asistida Por ComputadoraPaola Alexandra LaguadoPas encore d'évaluation
- Cohen2019 Atualização Sobre Os Aspectos Atuais Da Imagem Orbital .Tomografia Computadorizada, Ressonância Magnética e UltrassonografiaDocument11 pagesCohen2019 Atualização Sobre Os Aspectos Atuais Da Imagem Orbital .Tomografia Computadorizada, Ressonância Magnética e Ultrassonografiaana clara scopelPas encore d'évaluation
- Implant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyDocument6 pagesImplant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyPraveen Raj ThakurPas encore d'évaluation
- An Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningDocument7 pagesAn Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Implant OlogyDocument14 pagesImplant OlogyAya M RashidiPas encore d'évaluation
- Three-Dimensional Facial Simulation in BDocument10 pagesThree-Dimensional Facial Simulation in BVLAKORADOSPas encore d'évaluation
- FacialSurgery MMVR2005Document3 pagesFacialSurgery MMVR2005Mohamed AhmedPas encore d'évaluation
- 2019 - Yeung Et Al - Accuracy and Precision of 3d-Printed Implant Surgical Guideswith Different Implant Systems An in Vitro StudyDocument8 pages2019 - Yeung Et Al - Accuracy and Precision of 3d-Printed Implant Surgical Guideswith Different Implant Systems An in Vitro StudyRafael FedaltoPas encore d'évaluation
- From Implant Planning To Surgical Execution An Integrated Approach For Surgery in Oral ImplantologyDocument10 pagesFrom Implant Planning To Surgical Execution An Integrated Approach For Surgery in Oral ImplantologyDenisa CorneaPas encore d'évaluation
- Accuracy of Implant Placement With A Esterolitografia PDFDocument8 pagesAccuracy of Implant Placement With A Esterolitografia PDFSamuel Flores CalderonPas encore d'évaluation
- AJODO-2013 Bae 143 6 893Document9 pagesAJODO-2013 Bae 143 6 893player osamaPas encore d'évaluation
- Radiological Templates and Cad/Cam Surgical Guides-A Literature ReviewDocument37 pagesRadiological Templates and Cad/Cam Surgical Guides-A Literature ReviewMaqbul AlamPas encore d'évaluation
- 10 1016@j Prosdent 2019 05 027Document8 pages10 1016@j Prosdent 2019 05 027OctavioJose DuarteFrenkyPas encore d'évaluation
- Periodontal Plastic Surgery For Esthetic Crown LengtheningDocument4 pagesPeriodontal Plastic Surgery For Esthetic Crown LengtheningAbdelrahman GalalPas encore d'évaluation
- Accuracy of Using Computer-Aided Rapid Prototyping Templates For Mandible Reconstruction With An Iliac Crest GraftDocument9 pagesAccuracy of Using Computer-Aided Rapid Prototyping Templates For Mandible Reconstruction With An Iliac Crest GraftHương LanPas encore d'évaluation
- Intelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeDocument7 pagesIntelligent X-Ray Based Training System For Pedicle Screw Placement in Lumbar VertebraeCatalina Sorina ParfenePas encore d'évaluation
- 3D Jaw Modeling and AnimationDocument7 pages3D Jaw Modeling and AnimationOral SurgeonPas encore d'évaluation
- Mandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaDocument35 pagesMandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaGabriela Lizbeth ArmentaPas encore d'évaluation
- Three-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentreDocument9 pagesThree-Dimensional Navigation-Guided Percutaneous Screw Fixation For Nondisplaced and Displaced Pelvi-Acetabular Fractures in A Major Trauma CentrePierre MartzPas encore d'évaluation
- Moamen M Sarhan Evaluation of The Accuracy of ImplantDocument8 pagesMoamen M Sarhan Evaluation of The Accuracy of ImplantHayley NicPas encore d'évaluation
- Rahim Ov 2011Document11 pagesRahim Ov 2011Muslikah IkaPas encore d'évaluation
- Resume C-ArmDocument4 pagesResume C-Armp27838121011Pas encore d'évaluation
- FullMouthImplant SupportedRehabilitationDocument5 pagesFullMouthImplant SupportedRehabilitationSherif HamdyPas encore d'évaluation
- Seminario 6. Implant Placement Accuracy Using Dynamic NavigationDocument8 pagesSeminario 6. Implant Placement Accuracy Using Dynamic NavigationLenny GrauPas encore d'évaluation
- Comparison Ofthree Facebowsemiadjustable Articulator2233Document6 pagesComparison Ofthree Facebowsemiadjustable Articulator2233Brijesh MaskeyPas encore d'évaluation
- Virtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDDocument8 pagesVirtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDR KPas encore d'évaluation
- Efficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraDocument6 pagesEfficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraГне ДзжPas encore d'évaluation
- Preoperative Radiologic Planning of Implant Surgery in Compromised PatientsDocument14 pagesPreoperative Radiologic Planning of Implant Surgery in Compromised PatientskochikaghochiPas encore d'évaluation
- Obturator 2023Document7 pagesObturator 2023Dina AbdelmoezPas encore d'évaluation
- Intraoperative Imaging in Orbital Reconstruction: How Does It Affect The Position of The Implant?"Document6 pagesIntraoperative Imaging in Orbital Reconstruction: How Does It Affect The Position of The Implant?"quetmauhamPas encore d'évaluation
- Ecr2011 C-1038Document12 pagesEcr2011 C-1038guilhermeytoPas encore d'évaluation
- Accuracy of Surgical Positioning of Orthodontic Miniscrews With A Computer-Aided Design and Manufacturing TemplateDocument10 pagesAccuracy of Surgical Positioning of Orthodontic Miniscrews With A Computer-Aided Design and Manufacturing TemplateDONGXU LIUPas encore d'évaluation
- Radiological Templates and Cad/Cam SURGICAL GUIDES. A Literature ReviewDocument11 pagesRadiological Templates and Cad/Cam SURGICAL GUIDES. A Literature ReviewMaqbul AlamPas encore d'évaluation
- Use of Computer Navigation in Orthopedic OncologyDocument8 pagesUse of Computer Navigation in Orthopedic OncologyFrontiersPas encore d'évaluation
- Journal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj HowladerDocument7 pagesJournal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj Howladerlowjy119411Pas encore d'évaluation
- Mock SurgeryDocument7 pagesMock SurgeryElegant Dental clinicPas encore d'évaluation
- ASME IMECE2019 CuttingGuides RevisedDocument7 pagesASME IMECE2019 CuttingGuides Revisedalexis jonathanPas encore d'évaluation
- Establishing Orbital Floor Symmetry To Support Mirror Imaging in Computer-Aided Reconstruction of The Orbital FloorDocument3 pagesEstablishing Orbital Floor Symmetry To Support Mirror Imaging in Computer-Aided Reconstruction of The Orbital FloorМихаил КуликовPas encore d'évaluation
- DocumentDocument9 pagesDocumentSuma_DewiPas encore d'évaluation
- Harvard Digital Full ArchDocument6 pagesHarvard Digital Full ArchAmit SadhwaniPas encore d'évaluation
- Conebeam CT of The Head and Neck, Part 2: Clinical ApplicationsDocument8 pagesConebeam CT of The Head and Neck, Part 2: Clinical ApplicationshaneefmdfPas encore d'évaluation
- Ankle-Foot Orthosis Made by 3D Printing TechniqueDocument7 pagesAnkle-Foot Orthosis Made by 3D Printing Techniquejose diazPas encore d'évaluation
- Klatt 2013Document4 pagesKlatt 2013Sung Soon ChangPas encore d'évaluation
- Guided Transplantation TeethDocument6 pagesGuided Transplantation TeethDrMarkHoganPas encore d'évaluation
- Eth 28049 02Document126 pagesEth 28049 02raku2121Pas encore d'évaluation
- Park 2012Document6 pagesPark 2012Yassin SalahPas encore d'évaluation
- Navigation FessDocument5 pagesNavigation FessAravind NooneyPas encore d'évaluation
- Advanced Applications of Cone Beam Computed Tomography in OrthodonticsDocument15 pagesAdvanced Applications of Cone Beam Computed Tomography in Orthodonticsaung NaingmyoPas encore d'évaluation
- Three-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional ApplianceDocument12 pagesThree-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional AppliancealejandroPas encore d'évaluation
- Jomi 5004Document8 pagesJomi 5004Fernando Ari del CorroPas encore d'évaluation
- Alternative Method For Fabrication of Power ArmDocument2 pagesAlternative Method For Fabrication of Power ArmVikas VatsPas encore d'évaluation
- Evoked PotentialDocument6 pagesEvoked PotentialVikas VatsPas encore d'évaluation
- Facial AnatomyDocument11 pagesFacial AnatomySneha SthaPas encore d'évaluation
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDocument6 pagesVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsPas encore d'évaluation
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDocument17 pagesPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsPas encore d'évaluation
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDocument2 pagesBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsPas encore d'évaluation
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Document5 pages1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsPas encore d'évaluation
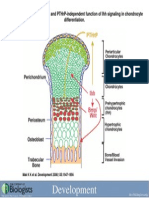
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Document1 pageDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsPas encore d'évaluation
- 4 Circulation Disorders PDFDocument69 pages4 Circulation Disorders PDFSetiawan SukmadjaPas encore d'évaluation
- Pelvix Organ ProlapsDocument5 pagesPelvix Organ ProlapskazugawaPas encore d'évaluation
- Metastases Bone DiseaseDocument59 pagesMetastases Bone Diseasemuhammad rustamPas encore d'évaluation
- Asthma Treatment GuidlineDocument56 pagesAsthma Treatment GuidlineEsther OdumanyePas encore d'évaluation
- User Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement ProgramDocument40 pagesUser Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement Programbobobobo12341212Pas encore d'évaluation
- CGHS Rates 2014 - Nagpur1Document58 pagesCGHS Rates 2014 - Nagpur1RajatPas encore d'évaluation
- Blood Cells LabDocument7 pagesBlood Cells LabKameron WardPas encore d'évaluation
- Reading - Age With Moderate DehydrationDocument8 pagesReading - Age With Moderate DehydrationSophia IbuyanPas encore d'évaluation
- Ascorbic Acid (Vitamin C) - Side Effects, Interactions, Warning, Dosage & UsesDocument4 pagesAscorbic Acid (Vitamin C) - Side Effects, Interactions, Warning, Dosage & UsesMuhammad ZuhriPas encore d'évaluation
- Parasitology - TrematodesDocument16 pagesParasitology - TrematodesMarlex SuanPas encore d'évaluation
- Lifetree Gut Relax, An Ayurvedic Health SupplementDocument13 pagesLifetree Gut Relax, An Ayurvedic Health SupplementLifetree WorldPas encore d'évaluation
- Levonorgestrel Emergency Contraception: (Plan B or Generic Equivalent)Document2 pagesLevonorgestrel Emergency Contraception: (Plan B or Generic Equivalent)AdityaWijayaPas encore d'évaluation
- JIA - Information For TeachersDocument4 pagesJIA - Information For TeachersragingreaderPas encore d'évaluation
- LT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewDocument3 pagesLT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewfatimaPas encore d'évaluation
- 2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPDocument4 pages2017 Spine CPT Code Changes: Kim Pollock, RN, MBA, CPC, CMDPZakariaAwaludinPas encore d'évaluation
- UNEP Directory March 2021Document34 pagesUNEP Directory March 2021Perera KusalPas encore d'évaluation
- Mycobacterial Infections Hcu Aug 2016 PDFDocument5 pagesMycobacterial Infections Hcu Aug 2016 PDFumarPas encore d'évaluation
- Pengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaDocument6 pagesPengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaevangelinePas encore d'évaluation
- 2012.tips For Healthy LivingDocument2 pages2012.tips For Healthy LivingNoelia Conca FrancésPas encore d'évaluation
- India's 1 Health Management LabDocument14 pagesIndia's 1 Health Management LabAjay Kumar dasPas encore d'évaluation
- Toronto Cataract ConferenceDocument6 pagesToronto Cataract ConferenceDee Margaux SantiagoPas encore d'évaluation
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezPas encore d'évaluation