Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
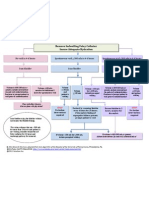
- SOP - Legal and Clinical Check - WebsiteDocument3 pagesSOP - Legal and Clinical Check - WebsiteMaddy SweetPas encore d'évaluation
- Marx Letter FDA CanadianHealth-NJUADocument5 pagesMarx Letter FDA CanadianHealth-NJUAmarxdocPas encore d'évaluation
- Brachytherapy in The Treatment of Cervical CancerDocument10 pagesBrachytherapy in The Treatment of Cervical CancervchendilPas encore d'évaluation
- Radiotherapy For Liver Metastases - A Review of Evidence PDFDocument11 pagesRadiotherapy For Liver Metastases - A Review of Evidence PDFvchendilPas encore d'évaluation
- Treatment of Locally Advanced Pancreatic Cancer - The Role of Radiation Therapy PDFDocument11 pagesTreatment of Locally Advanced Pancreatic Cancer - The Role of Radiation Therapy PDFvchendilPas encore d'évaluation
- Chamberlain - Practical Guidelines For The Treatment of Malignant GliomasDocument7 pagesChamberlain - Practical Guidelines For The Treatment of Malignant GliomasvchendilPas encore d'évaluation
- Gynaecological Clinical Guidelines - NHSDocument39 pagesGynaecological Clinical Guidelines - NHSvchendilPas encore d'évaluation
- Antimicrobial ResistanceDocument11 pagesAntimicrobial Resistanceapi-253312159Pas encore d'évaluation
- Foly Catheter Removal ProtocolDocument1 pageFoly Catheter Removal ProtocolMostafa ShamaaPas encore d'évaluation
- Brushing Teeth and RecessionDocument16 pagesBrushing Teeth and RecessionWayan SubadiPas encore d'évaluation
- "Heimlich Maneuver For Asthma" Study Reportedly Conducted On 67 Children in Barbados, W.I., Aged Six To 16, Funded by The Heimlich Institute and The Rotary Foundation of CincinnatiDocument156 pages"Heimlich Maneuver For Asthma" Study Reportedly Conducted On 67 Children in Barbados, W.I., Aged Six To 16, Funded by The Heimlich Institute and The Rotary Foundation of CincinnatiPeter M. HeimlichPas encore d'évaluation
- Biostatistics ServicesDocument2 pagesBiostatistics ServicesGVK Bio Sciences Private LimitedPas encore d'évaluation
- Applied Spectroscopy ReviewsDocument47 pagesApplied Spectroscopy ReviewsNicholas GravesPas encore d'évaluation
- English Medication and Medical Equipment GlossaryDocument7 pagesEnglish Medication and Medical Equipment GlossaryVeronicaGelfgrenPas encore d'évaluation
- Audits & Inspections CRO Perspective: DR - Prashant BodheDocument74 pagesAudits & Inspections CRO Perspective: DR - Prashant BodheJayanta DasguptaPas encore d'évaluation
- 57 TH Short Course ScheduleDocument10 pages57 TH Short Course SchedulevaluatPas encore d'évaluation
- Adverse Event Tracking Log: Subject Initials Subject ID# Page ofDocument1 pageAdverse Event Tracking Log: Subject Initials Subject ID# Page ofPratyPas encore d'évaluation
- Guideline On Active Substance Master File Procedure - EuropeanDocument22 pagesGuideline On Active Substance Master File Procedure - EuropeanNhonPhanThanhPas encore d'évaluation
- Cabana Lawsuit 2Document43 pagesCabana Lawsuit 2Paige OsburnPas encore d'évaluation
- Fda 1571Document2 pagesFda 1571Nitin KashyapPas encore d'évaluation
- RAC Candidate GuideDocument25 pagesRAC Candidate Guideasifmdzakaria100% (1)
- Sadowsky Et Al 2015 PDFDocument3 pagesSadowsky Et Al 2015 PDFeili1Pas encore d'évaluation
- Fixed FunctionalDocument14 pagesFixed FunctionalsuchitraPas encore d'évaluation
- Latanya Brown em ResumeDocument4 pagesLatanya Brown em Resumeapi-285904187Pas encore d'évaluation
- A Sistematic Review of Clinical Effectiveness of Wound Edge Protector Device in Abdominal Surgery Sajid2017Document8 pagesA Sistematic Review of Clinical Effectiveness of Wound Edge Protector Device in Abdominal Surgery Sajid2017andreigustvPas encore d'évaluation
- Assessment: Mental Health Care PlanDocument3 pagesAssessment: Mental Health Care PlannamitaPas encore d'évaluation
- FDA-1572 - Instr Supplmnt - 508 (7.13) PDFDocument3 pagesFDA-1572 - Instr Supplmnt - 508 (7.13) PDFJay BingoPas encore d'évaluation
- New Drug Delivery Systems: A Global OpportunityDocument24 pagesNew Drug Delivery Systems: A Global OpportunityRugun Clara SamosirPas encore d'évaluation
- Hodgkins PortugueseDocument77 pagesHodgkins PortugueseSaadina HijaziPas encore d'évaluation
- Epidemiology ReviewDocument29 pagesEpidemiology Reviewjohnkad100% (4)
- Oral Vaccine OM 89 in The Recurrent Urinary Tract Infection Prophylaxis A Realistic Systematic Review With Meta-Analysis PDFDocument6 pagesOral Vaccine OM 89 in The Recurrent Urinary Tract Infection Prophylaxis A Realistic Systematic Review With Meta-Analysis PDFLili SaquingaPas encore d'évaluation
- Gunapadam Jeevam VagupuDocument24 pagesGunapadam Jeevam VagupuDr. S. MerishPas encore d'évaluation
- Stretch For The Treatment and Prevention of Contracture An Abridged Republication of A Cochrane Systematic ReviewDocument9 pagesStretch For The Treatment and Prevention of Contracture An Abridged Republication of A Cochrane Systematic ReviewAnna Azizah100% (1)
- Journal Club Template: For Randomized Controlled TrialsDocument19 pagesJournal Club Template: For Randomized Controlled TrialsAndrew DavidsonPas encore d'évaluation
- S22083en PDFDocument179 pagesS22083en PDFIndra MaulanaPas encore d'évaluation