Vous aimerez peut-être aussi
- Plant Nosodes - According To DR John Henry ClarkeDocument29 pagesPlant Nosodes - According To DR John Henry Clarkemelos24Pas encore d'évaluation
- List of Nosodes and Sarcodes (Clarke)Document3 pagesList of Nosodes and Sarcodes (Clarke)melos24100% (1)
- Allen - The Chronic Miasms - IndexDocument6 pagesAllen - The Chronic Miasms - Indexmelos24Pas encore d'évaluation
- Nosodes and Sarcodes - ClarkeDocument12 pagesNosodes and Sarcodes - Clarkemelos24Pas encore d'évaluation
- Sarcodes - John Henry ClarkeDocument156 pagesSarcodes - John Henry Clarkemelos24Pas encore d'évaluation
- The Materia Medica of The Nosodes - AllenDocument108 pagesThe Materia Medica of The Nosodes - Allenmelos24Pas encore d'évaluation
- Hahnemann - Chronic Diseases (1835)Document277 pagesHahnemann - Chronic Diseases (1835)melos24Pas encore d'évaluation
- Allen - The Chronic Miasms - Heart (Excerpt)Document6 pagesAllen - The Chronic Miasms - Heart (Excerpt)melos24Pas encore d'évaluation
- Clinical Experience With Some Rare NosodesDocument98 pagesClinical Experience With Some Rare Nosodesmelos2471% (7)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- India Internet Goldman SachsDocument86 pagesIndia Internet Goldman SachsTaranjeet SinghPas encore d'évaluation
- Boxnhl MBS (Design-D) Check SheetDocument13 pagesBoxnhl MBS (Design-D) Check SheetKumari SanayaPas encore d'évaluation
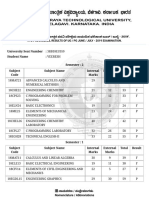
- VTU Result PDFDocument2 pagesVTU Result PDFVaibhavPas encore d'évaluation
- Ant Colony AlgorithmDocument11 pagesAnt Colony Algorithmjaved765Pas encore d'évaluation
- ECON266 Worksheet 8Document4 pagesECON266 Worksheet 8Oi OuPas encore d'évaluation
- 7 Critical Reading StrategiesDocument1 page7 Critical Reading StrategiesWilliam Holt100% (2)
- Lesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Document3 pagesLesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Lovella GacaPas encore d'évaluation
- Waterfront Development Goals and ObjectivesDocument2 pagesWaterfront Development Goals and ObjectivesShruthi Thakkar100% (1)
- Functions of Communication Oral Communication PDFDocument12 pagesFunctions of Communication Oral Communication PDFKrystle Francess Barrios0% (1)
- Hinog vs. MellicorDocument11 pagesHinog vs. MellicorGreta VilarPas encore d'évaluation
- History Paper 2 IB Study GuideDocument6 pagesHistory Paper 2 IB Study Guidersuresh1995100% (4)
- RK Modul 2 PDFDocument41 pagesRK Modul 2 PDFRUSTIANI WIDIASIHPas encore d'évaluation
- Local Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankDocument12 pagesLocal Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankJessicaPorterfqmei100% (18)
- Lolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad MedinaceliDocument3 pagesLolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad Medinacelichatmche-06Pas encore d'évaluation
- Chapter 23 AP World History NotesDocument6 pagesChapter 23 AP World History NotesWesley KoerberPas encore d'évaluation
- SDLC Review ChecklistDocument4 pagesSDLC Review Checklistmayank govilPas encore d'évaluation
- Blue Mountain Coffee Case (ADBUDG)Document16 pagesBlue Mountain Coffee Case (ADBUDG)Nuria Sánchez Celemín100% (1)
- Young Learners Starters Sample Papers 2018 Vol1Document15 pagesYoung Learners Starters Sample Papers 2018 Vol1Natalia García GarcíaPas encore d'évaluation
- GEHealthcare Brochure - Discovery CT590 RT PDFDocument12 pagesGEHealthcare Brochure - Discovery CT590 RT PDFAnonymous ArdclHUOPas encore d'évaluation
- Question No. 2: (Type Here)Document5 pagesQuestion No. 2: (Type Here)temestruc71Pas encore d'évaluation
- MathTextbooks9 12Document64 pagesMathTextbooks9 12Andrew0% (1)
- Pitch PDFDocument12 pagesPitch PDFJessa Mae AnonuevoPas encore d'évaluation
- Basa BasaDocument4 pagesBasa Basamarilou sorianoPas encore d'évaluation
- Ron Clark ReflectionDocument3 pagesRon Clark Reflectionapi-376753605Pas encore d'évaluation
- Basic Trigonometric FunctionDocument34 pagesBasic Trigonometric FunctionLony PatalPas encore d'évaluation
- Stat 201 - Project 1 - Spring 2019: Due Friday, February 8, 2019Document9 pagesStat 201 - Project 1 - Spring 2019: Due Friday, February 8, 2019Bao GanPas encore d'évaluation
- Contemporary Watchdogs Domesticated: Conduct of Punjabi Print Media in Punjab During The Assembly Elections of 2007Document20 pagesContemporary Watchdogs Domesticated: Conduct of Punjabi Print Media in Punjab During The Assembly Elections of 2007Sarban MalhansPas encore d'évaluation
- Your ManDocument5 pagesYour ManPaulino JoaquimPas encore d'évaluation
- Business Enterprise Simulation Quarter 3 - Module 2 - Lesson 1: Analyzing The MarketDocument13 pagesBusiness Enterprise Simulation Quarter 3 - Module 2 - Lesson 1: Analyzing The MarketJtm GarciaPas encore d'évaluation
- 4.1 Genetic Counselling 222Document12 pages4.1 Genetic Counselling 222Sahar JoshPas encore d'évaluation