Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Emerging Characteristics of Isotonitazene Involved.14Document3 pagesEmerging Characteristics of Isotonitazene Involved.14ABC Action News50% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Analgesic Used in Oral SurgeryDocument70 pagesAnalgesic Used in Oral SurgeryAkram ThabetPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Narcotics Controlled Drugs TableDocument4 pagesNarcotics Controlled Drugs TableDurgaNadellaPas encore d'évaluation
- Morphine Drug StudyDocument2 pagesMorphine Drug StudyNo Vem BerPas encore d'évaluation
- Biostatistics 22003Document35 pagesBiostatistics 22003god4alllPas encore d'évaluation
- Brand and Generic Medication Reference ListDocument6 pagesBrand and Generic Medication Reference ListAndi Dewi Pratiwi50% (2)
- Geriatric Risk Tool Guide for Safe Hospital DischargesDocument2 pagesGeriatric Risk Tool Guide for Safe Hospital Dischargesgod4alllPas encore d'évaluation
- Lined 2.5 ModifiedDocument2 pagesLined 2.5 Modifiedgod4alllPas encore d'évaluation
- Bioavail Equiv2Document17 pagesBioavail Equiv2god4alllPas encore d'évaluation
- HIPAA PHI List - 18 Identifiers and DefinitionDocument6 pagesHIPAA PHI List - 18 Identifiers and Definitiongod4alll0% (1)
- CCGP Handbook Oct 12 - CM2 PDFDocument21 pagesCCGP Handbook Oct 12 - CM2 PDFgod4alllPas encore d'évaluation
- Skin and Soft Tissue Infections: CellulitisDocument9 pagesSkin and Soft Tissue Infections: Cellulitisgod4alllPas encore d'évaluation
- Geriatric Risk Tool Guide for Safe Hospital DischargesDocument2 pagesGeriatric Risk Tool Guide for Safe Hospital Dischargesgod4alllPas encore d'évaluation
- C and S Reactive ProteinDocument3 pagesC and S Reactive Proteingod4alllPas encore d'évaluation
- Rptabstracts in Presentation Order 2013 PDFDocument283 pagesRptabstracts in Presentation Order 2013 PDFgod4alllPas encore d'évaluation
- Pharacokinatits and Pharma Co DynamicsDocument18 pagesPharacokinatits and Pharma Co DynamicsPrasad PoluPas encore d'évaluation
- Structural Heart DiseaseDocument1 pageStructural Heart Diseasegod4alllPas encore d'évaluation
- Pain Supporting Information PDFDocument59 pagesPain Supporting Information PDFgod4alllPas encore d'évaluation
- 0402 - Cycle Cellulities PDFDocument5 pages0402 - Cycle Cellulities PDFgod4alllPas encore d'évaluation
- Be Guidelines Draft Ver10 March 16, 05Document0 pageBe Guidelines Draft Ver10 March 16, 05Devianti YupzPas encore d'évaluation
- MUSC Opioid Analgesic Comparison Chart: C U O ADocument8 pagesMUSC Opioid Analgesic Comparison Chart: C U O Agod4alllPas encore d'évaluation
- Effects of Exercise On Insulin Sensitivity in Humans: John T. Devlin, MDDocument4 pagesEffects of Exercise On Insulin Sensitivity in Humans: John T. Devlin, MDgod4alllPas encore d'évaluation
- Significance Testing ExplainedDocument8 pagesSignificance Testing Explainedgod4alllPas encore d'évaluation
- Normal ValuesDocument6 pagesNormal ValuesMc Crister SilangPas encore d'évaluation
- Febrile Neutropenia: Guidelines For The Management ofDocument0 pageFebrile Neutropenia: Guidelines For The Management ofgod4alllPas encore d'évaluation
- COPD drug trial design evaluated in RCT crossover studyDocument67 pagesCOPD drug trial design evaluated in RCT crossover studygod4alllPas encore d'évaluation
- COPD drug trial design evaluated in RCT crossover studyDocument67 pagesCOPD drug trial design evaluated in RCT crossover studygod4alllPas encore d'évaluation
- FN 2011 IdsaDocument38 pagesFN 2011 IdsaNuttawath UngwichanpunyaPas encore d'évaluation
- ABSTRACT: Cancer Patients Who Develop Infections, Especially Those Receiving ChemotherapyDocument5 pagesABSTRACT: Cancer Patients Who Develop Infections, Especially Those Receiving Chemotherapygod4alllPas encore d'évaluation
- Febrile Neutropenia PDFDocument2 pagesFebrile Neutropenia PDFgod4alllPas encore d'évaluation
- ASHP Medication Use EvaluationDocument3 pagesASHP Medication Use EvaluationArslan BashirPas encore d'évaluation
- Naloxone: What Are Some Signs of An Opioid Overdose?Document4 pagesNaloxone: What Are Some Signs of An Opioid Overdose?Fajriah SaraswatiPas encore d'évaluation
- Contoh Gol. Obat KIEDocument5 pagesContoh Gol. Obat KIEYanuar prasetyoPas encore d'évaluation
- List Nama Obat Generik Kekuatan Sediaan Dan Nama DagangDocument13 pagesList Nama Obat Generik Kekuatan Sediaan Dan Nama DagangTius LenaPas encore d'évaluation
- Ketamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiDocument6 pagesKetamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiranirahmaniPas encore d'évaluation
- Autocoids 1Document9 pagesAutocoids 1Rutwik YPas encore d'évaluation
- ATI Flash Cards 04, Medications For Pain and InflammationDocument38 pagesATI Flash Cards 04, Medications For Pain and InflammationAhmed KamalPas encore d'évaluation
- Polmaforce RCPA Circular 16.10.23Document2 pagesPolmaforce RCPA Circular 16.10.23ALIPas encore d'évaluation
- Nervous System and Neurology Assignment - AcrobatiqDocument1 pageNervous System and Neurology Assignment - Acrobatiqjose. medina9Pas encore d'évaluation
- Prescription and Illicit Drug CRMs PDFDocument2 pagesPrescription and Illicit Drug CRMs PDFvasiliyPas encore d'évaluation
- Pain Relief Combo of Tramadol and ParacetamolDocument1 pagePain Relief Combo of Tramadol and Paracetamolenirdnas14100% (2)
- VivitrolFactSheet PDFDocument5 pagesVivitrolFactSheet PDFwebmaster@drugpolicy.org100% (1)
- Farmacologia Basica de Los OpioidesDocument6 pagesFarmacologia Basica de Los OpioidesMaría Alejandra García QPas encore d'évaluation
- Common Drugs for HODocument6 pagesCommon Drugs for HOAthirahRaraPas encore d'évaluation
- Tugas SBL Spesialit Antiinflamasi Dan AntiasmaDocument2 pagesTugas SBL Spesialit Antiinflamasi Dan AntiasmaAfifatul JannahPas encore d'évaluation
- Dr. Lola Susianti, Sppd-FinasimDocument28 pagesDr. Lola Susianti, Sppd-Finasimfahmy_tampanPas encore d'évaluation
- Missouri Counties Sue Drug Companies Over Opioid CrisisDocument274 pagesMissouri Counties Sue Drug Companies Over Opioid CrisisSam ClancyPas encore d'évaluation
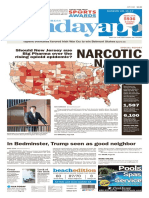
- Asbury Park Press Front Page, Sunday, June 11, 2017Document1 pageAsbury Park Press Front Page, Sunday, June 11, 2017Asbury Park PressPas encore d'évaluation
- Isoquinoline AlkaloidsDocument83 pagesIsoquinoline AlkaloidsAlan K MhamadPas encore d'évaluation
- Step Ladder in Pain Management (Dr. YNS)Document39 pagesStep Ladder in Pain Management (Dr. YNS)Erick Rangga JuniorPas encore d'évaluation
- Fluoxetina Medimart 20 MG 40 TabletasDocument51 pagesFluoxetina Medimart 20 MG 40 TabletasJose Manuel Rito GonzalezPas encore d'évaluation
- The Efficacy of Combination Analgesic Therapy in Relieving Dental PainDocument11 pagesThe Efficacy of Combination Analgesic Therapy in Relieving Dental Painjosselyn berrioPas encore d'évaluation
- Drugs Contraindicated in PregnancyDocument2 pagesDrugs Contraindicated in PregnancyErum IftikharPas encore d'évaluation
- Alphex PDFDocument1 pageAlphex PDFIdalia OrtegaPas encore d'évaluation
- Equate Wal MartDocument7 pagesEquate Wal MartNope nothingPas encore d'évaluation
- Opioid Receptor Agonists and AntagonistsDocument22 pagesOpioid Receptor Agonists and AntagonistsSiddharth Anand80% (5)