Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Esbl Producing eDocument45 pagesEsbl Producing eapi-205355237Pas encore d'évaluation
- Dettol HygieneDocument20 pagesDettol Hygieneruchita1989Pas encore d'évaluation
- Pox Viruses: Structure and ReplicationDocument5 pagesPox Viruses: Structure and ReplicationIDRAAK HUSSAINPas encore d'évaluation
- Specimen Collection, Transport and ProcessingDocument29 pagesSpecimen Collection, Transport and ProcessingGladys Marie WillkomPas encore d'évaluation
- MastitisDocument2 pagesMastitisJuviely PremacioPas encore d'évaluation
- FAMILY PLanning FinalDocument23 pagesFAMILY PLanning FinalLebo Ramokolo100% (1)
- Communicable and Infectious Disease Nursing-NewDocument15 pagesCommunicable and Infectious Disease Nursing-NewShandz de RosasPas encore d'évaluation
- Biology Set 1 QuestionsDocument15 pagesBiology Set 1 QuestionsAnkit RaoPas encore d'évaluation
- Novel Coronavirus Landscape Covid 19Document9 pagesNovel Coronavirus Landscape Covid 19kenPas encore d'évaluation
- Nursing Care Plan for Acute Pain in TonsillitisDocument5 pagesNursing Care Plan for Acute Pain in Tonsillitisesteffie21100% (1)
- 04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years OldDocument2 pages04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years Oldapi-309082881Pas encore d'évaluation
- NSTP QUIZ - Feb. 14, 2022 - Google FormsDocument3 pagesNSTP QUIZ - Feb. 14, 2022 - Google FormsDarlene De PazPas encore d'évaluation
- ESSAY - MELI MIRANDA Impact of The Pandemic On The Education SectorDocument2 pagesESSAY - MELI MIRANDA Impact of The Pandemic On The Education SectorMeli Miranda TambunanPas encore d'évaluation
- Actinomycetes: Gram-positive filamentous bacteriaDocument18 pagesActinomycetes: Gram-positive filamentous bacteriayota_ahlyPas encore d'évaluation
- Clinical Laboratory Science Review by Theriot - JarreauDocument12 pagesClinical Laboratory Science Review by Theriot - JarreauJuneya Koo100% (1)
- Background Information - Ebola Virus DiseaseDocument5 pagesBackground Information - Ebola Virus DiseaseFlabberPas encore d'évaluation
- What Is Flariasis?: Symptoms of Acute InfectionDocument3 pagesWhat Is Flariasis?: Symptoms of Acute InfectionRoshni ChoudharyPas encore d'évaluation
- Differential Diagnosis of Lymphadenopathy in ChildrenDocument21 pagesDifferential Diagnosis of Lymphadenopathy in ChildrenAnaPas encore d'évaluation
- Management of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument13 pagesManagement of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurPas encore d'évaluation
- IVRSDocument61 pagesIVRSAndrew ChinchillaPas encore d'évaluation
- Abscess Scrotum DrainageDocument7 pagesAbscess Scrotum DrainageRosyPas encore d'évaluation
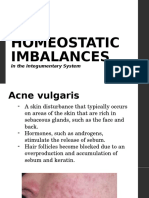
- Homeostatic Imbalances: in The Integumentary SystemDocument27 pagesHomeostatic Imbalances: in The Integumentary SystemMarilou Dacles IIPas encore d'évaluation
- HepatitisDocument20 pagesHepatitishnndisfh100% (1)
- Risk Management Prelim ReviewerDocument3 pagesRisk Management Prelim ReviewerCharmaigne BañaresPas encore d'évaluation
- Rubella & FlavivirusDocument53 pagesRubella & Flaviviruskiedd_04Pas encore d'évaluation
- Nursing Considerations for MeropenemDocument2 pagesNursing Considerations for MeropenemKullin Rain100% (1)
- Traditional Chinese Medicine For Human Papillomavirus (HPV) Infections: A Systematic ReviewDocument7 pagesTraditional Chinese Medicine For Human Papillomavirus (HPV) Infections: A Systematic ReviewDiego Gomes100% (1)
- Medical ProtozoologyDocument6 pagesMedical ProtozoologyRaymund MontoyaPas encore d'évaluation
- Daftar PustakaDocument4 pagesDaftar Pustakapiko pikoPas encore d'évaluation
- Tell Me Why My Children Died by Charles L. Briggs and Clara Mantini-BriggsDocument46 pagesTell Me Why My Children Died by Charles L. Briggs and Clara Mantini-BriggsDuke University PressPas encore d'évaluation