Vous aimerez peut-être aussi
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoPas encore d'évaluation
- Journal Read ChiaDocument14 pagesJournal Read ChiaChris Tine ChiaPas encore d'évaluation
- Vap NicuDocument8 pagesVap NicuWiwit ClimberPas encore d'évaluation
- Neonatal PneumoniaDocument8 pagesNeonatal PneumoniaAde Gustina SiahaanPas encore d'évaluation
- Minor Diagnostic Factors in Ventilator Associated Pneumonia in ChildrenDocument9 pagesMinor Diagnostic Factors in Ventilator Associated Pneumonia in ChildrenmariskaPas encore d'évaluation
- VAP Incidence, Risk Factors and Bacteria in PICUDocument6 pagesVAP Incidence, Risk Factors and Bacteria in PICURabiatul 'raney' AdawiyahPas encore d'évaluation
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurPas encore d'évaluation
- Risk Factor TaiwanDocument5 pagesRisk Factor TaiwanMira ApriliaPas encore d'évaluation
- ADW Presentasi - Epidemiologi VAP Hippi 2023Document30 pagesADW Presentasi - Epidemiologi VAP Hippi 2023ERIE YUWITA SARIPas encore d'évaluation
- Risk Factors for Suppurative Complications in Children with PneumoniaDocument6 pagesRisk Factors for Suppurative Complications in Children with PneumoniaWilson LeccaPas encore d'évaluation
- Carraro 2013 RSBMTV 46 N 2 P 161Document5 pagesCarraro 2013 RSBMTV 46 N 2 P 161Emerson CarraroPas encore d'évaluation
- Microbiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitDocument4 pagesMicrobiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitIJAR JOURNALPas encore d'évaluation
- 209 Full PDFDocument8 pages209 Full PDFAngga PratamaPas encore d'évaluation
- JCDR 10 SC06Document6 pagesJCDR 10 SC06YANPas encore d'évaluation
- CAPDocument21 pagesCAPLoids IgnacioPas encore d'évaluation
- Ventilator Associated Pneumonia: Incidence, Profile and Outcome in Pediatric Intensive Care Unit of Tertiary Care CentreDocument5 pagesVentilator Associated Pneumonia: Incidence, Profile and Outcome in Pediatric Intensive Care Unit of Tertiary Care CentreJoaquín SosaPas encore d'évaluation
- Clinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapyDocument10 pagesClinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapySuci ZahraniPas encore d'évaluation
- AygunDocument5 pagesAygunotheasPas encore d'évaluation
- Oseltamivir For Coronavirus Illness:: ResearchDocument6 pagesOseltamivir For Coronavirus Illness:: ResearchellaPas encore d'évaluation
- Jurnal 2Document12 pagesJurnal 2zingioPas encore d'évaluation
- Effect of Reusing Suction Catheters On The Occurrence of Pneumonia in ChildrenDocument9 pagesEffect of Reusing Suction Catheters On The Occurrence of Pneumonia in ChildrenSitti Rosdiana YahyaPas encore d'évaluation
- Critical Care InfectionDocument15 pagesCritical Care InfectionTito Ahmad RizkiawanPas encore d'évaluation
- Covid Ihu 2 1 PDFDocument28 pagesCovid Ihu 2 1 PDFSayed MachfudPas encore d'évaluation
- Covid Ihu 2 1 PDFDocument28 pagesCovid Ihu 2 1 PDFhlim_13Pas encore d'évaluation
- Original Article: Evaluation of Microbial Flora in Chronic Tonsillitis and The Role of TonsillectomyDocument5 pagesOriginal Article: Evaluation of Microbial Flora in Chronic Tonsillitis and The Role of TonsillectomyAmril BillahmarPas encore d'évaluation
- Mortality in Typhoid Intestinal Perforation-A Declining TrendDocument3 pagesMortality in Typhoid Intestinal Perforation-A Declining Trendaura009Pas encore d'évaluation
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiPas encore d'évaluation
- Lau 2015Document25 pagesLau 2015tifanny carolinaPas encore d'évaluation
- Neonatal Pneumonia Incidence and Outcomes in BangladeshDocument6 pagesNeonatal Pneumonia Incidence and Outcomes in BangladeshAnonymous Us5v7C6QhPas encore d'évaluation
- A Prospective, Randomized Study of Ventilator-Associated Pneumonia in Patients Using A Closed vs. Open Suction SystemDocument7 pagesA Prospective, Randomized Study of Ventilator-Associated Pneumonia in Patients Using A Closed vs. Open Suction SystemFebri Nick Daniel SihombingPas encore d'évaluation
- BJC 2017154Document8 pagesBJC 2017154Altair CamargoPas encore d'évaluation
- Covid NiñosDocument9 pagesCovid NiñosPaola ZuluagaPas encore d'évaluation
- Streptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanDocument8 pagesStreptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanInternational Medical PublisherPas encore d'évaluation
- Hospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionDocument7 pagesHospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionadhitiaPas encore d'évaluation
- Persistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneDocument7 pagesPersistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneMark ReinhardtPas encore d'évaluation
- Endocervical Polyps in High Risk Human Papillomavirus InfectionsDocument4 pagesEndocervical Polyps in High Risk Human Papillomavirus InfectionsGLAYZA CLARITOPas encore d'évaluation
- Predictors of Urinary Tract Infection Among Febrile Children Attending at Bugando Medical Centre Northwestern, TanzaniaDocument7 pagesPredictors of Urinary Tract Infection Among Febrile Children Attending at Bugando Medical Centre Northwestern, TanzaniaInternational Medical PublisherPas encore d'évaluation
- Journal of Pediatric Sciences: Diphtheria: Is It Really OUT?Document5 pagesJournal of Pediatric Sciences: Diphtheria: Is It Really OUT?ayuPas encore d'évaluation
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaPas encore d'évaluation
- 2 Dümichen2012Document6 pages2 Dümichen2012Sergio SampaioPas encore d'évaluation
- En 13Document8 pagesEn 13Bruna CarvalhoPas encore d'évaluation
- Typhoid JournalDocument7 pagesTyphoid JournalRegina AyediaPas encore d'évaluation
- Jurnal Kritis ICU Bundle Vap PneumoniaDocument6 pagesJurnal Kritis ICU Bundle Vap PneumoniaAdzkia PintaPas encore d'évaluation
- Ak 2011Document6 pagesAk 2011bouchra8blsPas encore d'évaluation
- Marneffei: Cytological Diagnosis of Penicillium InfectionDocument5 pagesMarneffei: Cytological Diagnosis of Penicillium InfectionAnonymous oQtve4oPas encore d'évaluation
- Bacterial Tonsillar Microbiota and Antibiogram in Recurrent TonsillitisDocument5 pagesBacterial Tonsillar Microbiota and Antibiogram in Recurrent TonsillitisResianaPutriPas encore d'évaluation
- Nosocomial Pneumonia in AdultsDocument28 pagesNosocomial Pneumonia in AdultsAndrie WigunaPas encore d'évaluation
- Antimicrobial Susceptibility Among Pathogens Isolated in Early-Versus Late-Onset Ventilator-Associated PneumoniaDocument10 pagesAntimicrobial Susceptibility Among Pathogens Isolated in Early-Versus Late-Onset Ventilator-Associated PneumoniaJeremy CPas encore d'évaluation
- Abdul CadarDocument4 pagesAbdul CadarVitta Kusma WijayaPas encore d'évaluation
- Ebn RespiDocument17 pagesEbn RespilablabkurmPas encore d'évaluation
- 6 Original CandiduriaDocument7 pages6 Original CandiduriaHarnadi WonogiriPas encore d'évaluation
- Use and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General PracticeDocument9 pagesUse and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General Practicemicrobehunter007Pas encore d'évaluation
- EwswsawnDocument5 pagesEwswsawnProbioticsAnywherePas encore d'évaluation
- TurquiaDocument8 pagesTurquiaanselmopesquisa2769Pas encore d'évaluation
- Clinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency DepartmentDocument5 pagesClinical Predictors of Radiographic Abnormalities Among Infants With Bronchiolitis in A Paediatric Emergency Departmentnavali rahmaPas encore d'évaluation
- Typhoid Immunization Strategy for Children in PakistanDocument24 pagesTyphoid Immunization Strategy for Children in Pakistanmoon1312Pas encore d'évaluation
- Comparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-AcquiredDocument9 pagesComparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-Acquiredjuloc34Pas encore d'évaluation
- VAP Diagnosis 2009Document8 pagesVAP Diagnosis 2009Illham Setiawan SulistioPas encore d'évaluation
- Pediatric Tuberculous Pleural EffusionDocument5 pagesPediatric Tuberculous Pleural EffusionAnnisa SasaPas encore d'évaluation
- Hipertensi PBLDocument41 pagesHipertensi PBLAl MuzakkiPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaAl MuzakkiPas encore d'évaluation
- Kul. Gagal JantungDocument28 pagesKul. Gagal JantungAl MuzakkiPas encore d'évaluation
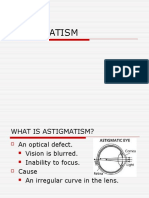
- ASTIGMATISM (Lucas Vigneaux) FinalDocument11 pagesASTIGMATISM (Lucas Vigneaux) FinalAl MuzakkiPas encore d'évaluation
- Paliatif CareDocument13 pagesPaliatif CareAl MuzakkiPas encore d'évaluation
- Unlock-Induction ANSE10 WMDocument8 pagesUnlock-Induction ANSE10 WMAl MuzakkiPas encore d'évaluation
- Jijin 140725134811 Phpapp01Document52 pagesJijin 140725134811 Phpapp01Al MuzakkiPas encore d'évaluation
- TSWJ2014 270120Document6 pagesTSWJ2014 270120Al MuzakkiPas encore d'évaluation
- Journal Rockey MountainDocument4 pagesJournal Rockey MountainAl MuzakkiPas encore d'évaluation
- Activate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechDocument9 pagesActivate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechAl MuzakkiPas encore d'évaluation
- Clin Gui EncephalitisDocument9 pagesClin Gui EncephalitisAl MuzakkiPas encore d'évaluation
- AktifasiDocument1 pageAktifasiAl MuzakkiPas encore d'évaluation
- Enable .NET Framework 3.... Iew To Run ApplicationsDocument12 pagesEnable .NET Framework 3.... Iew To Run ApplicationsAl MuzakkiPas encore d'évaluation
- Patient Risk Factors Best Practices SsiDocument9 pagesPatient Risk Factors Best Practices SsiAl MuzakkiPas encore d'évaluation
- Activate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechDocument9 pagesActivate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechAl MuzakkiPas encore d'évaluation
- JADWAL OPERASI INSTALASI BEDAH SENTRAL RSUD dr. ZAINOEL ABIDIN BANDA ACEHDocument27 pagesJADWAL OPERASI INSTALASI BEDAH SENTRAL RSUD dr. ZAINOEL ABIDIN BANDA ACEHAl MuzakkiPas encore d'évaluation
- Activate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechDocument9 pagesActivate Win8 Via KMS (WORKING!) (12!12!2012) (UPDATED+SUPPORT) (ProWMC Permanent Activation Added) - Windows 8 - 7pm TechAl MuzakkiPas encore d'évaluation
- CDC - Ventilator-Associated Pneumonia (VAP) EventDocument13 pagesCDC - Ventilator-Associated Pneumonia (VAP) EventAl MuzakkiPas encore d'évaluation
- SuisseMed Company ProfileDocument60 pagesSuisseMed Company ProfileCarepro AsiaPas encore d'évaluation
- Test Bank For Understanding The Essentials of Critical Care Nursing 2nd Edition Kathleen Ouimet Perrin Carrie Edgerly MacleodDocument9 pagesTest Bank For Understanding The Essentials of Critical Care Nursing 2nd Edition Kathleen Ouimet Perrin Carrie Edgerly MacleodFelix Guy100% (26)
- Medical Vocabulary: Part of Speech AdjDocument11 pagesMedical Vocabulary: Part of Speech Adjhisamol956Pas encore d'évaluation
- Algorithm For COVID19 Referral and TriageDocument1 pageAlgorithm For COVID19 Referral and Triagejeffrey ordonezPas encore d'évaluation
- Empanelment On 19.10Document8 pagesEmpanelment On 19.10api-3832244100% (1)
- Mind Invaders - Dave HuntDocument331 pagesMind Invaders - Dave Huntinfomih70100% (2)
- Pressure Ulcer Assessment and Treatment (PDFDrive)Document88 pagesPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliPas encore d'évaluation
- ICU Prophylaxis ChecklistDocument41 pagesICU Prophylaxis ChecklistBharti NaraPas encore d'évaluation
- CS HF Directory 2018 Print PDFDocument80 pagesCS HF Directory 2018 Print PDFAt Day's WardPas encore d'évaluation
- Urinary Tract Infections 2021 UpdateDocument14 pagesUrinary Tract Infections 2021 UpdateSandy GaresPas encore d'évaluation
- 7.2post Resus Algorithms 1Document1 page7.2post Resus Algorithms 1Massimo Di BenedettoPas encore d'évaluation
- Procalcitonin Guided Antibiotic TherapyDocument20 pagesProcalcitonin Guided Antibiotic TherapyhziglamPas encore d'évaluation
- Sample: Reading Sub-Test - Question Paper: Parts B & CDocument16 pagesSample: Reading Sub-Test - Question Paper: Parts B & CSajana Thulung100% (1)
- Gandaki Medical College: Teaching Hospital & Research Centre Pvt. LTDDocument2 pagesGandaki Medical College: Teaching Hospital & Research Centre Pvt. LTDSushant AcharyaPas encore d'évaluation
- Critical care patients' psychosocial problemsDocument5 pagesCritical care patients' psychosocial problemsSaif Ahmed jubarPas encore d'évaluation
- PICU NICU OrientationDocument8 pagesPICU NICU OrientationSony PrabowoPas encore d'évaluation
- ProspectusDocument64 pagesProspectusIMRANPas encore d'évaluation
- ABC Hospital OverviewDocument12 pagesABC Hospital OverviewKrishna100% (1)
- Policy - Document LIC TusharDocument54 pagesPolicy - Document LIC Tusharwaghtushar1212Pas encore d'évaluation
- Vol 4 DBR EPC AIIMS GKPR - 21.01.2018Document234 pagesVol 4 DBR EPC AIIMS GKPR - 21.01.2018Shyam SinghPas encore d'évaluation
- Evaluation of Antimicrobial Activity of a Natural Fogging SolutionDocument16 pagesEvaluation of Antimicrobial Activity of a Natural Fogging SolutionednisoPas encore d'évaluation
- Musallam 2018Document7 pagesMusallam 2018Koup NuPas encore d'évaluation
- Trauma TriageDocument34 pagesTrauma TriageMonica FalconePas encore d'évaluation
- Covid-19 Supporting Nurses' Psychological and Mental HealthDocument10 pagesCovid-19 Supporting Nurses' Psychological and Mental HealthIka JuitaPas encore d'évaluation
- ResumeDocument3 pagesResumeapi-383804230Pas encore d'évaluation
- Close, OpenDocument7 pagesClose, OpenNoeRhul M-lhati OelfhaPas encore d'évaluation
- VAP Prevention StrategiesDocument6 pagesVAP Prevention StrategiesCGKN BanyuwangiPas encore d'évaluation
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument17 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakayashramawatPas encore d'évaluation
- 22PG MATH-plus-Rationale-Journal-of-Intensive-Care-Medicine-Dec2020Document22 pages22PG MATH-plus-Rationale-Journal-of-Intensive-Care-Medicine-Dec2020Barbara RowePas encore d'évaluation
- Nursing Students Experiences in Critical Care Course A Qualitative StudyDocument7 pagesNursing Students Experiences in Critical Care Course A Qualitative StudyEkoArsetyantoPas encore d'évaluation