Vous aimerez peut-être aussi
- Peptide and Protein DeliveryD'EverandPeptide and Protein DeliveryChris Van Der WalleÉvaluation : 2 sur 5 étoiles2/5 (1)
- Impact of Coenzyme Q10 On Inflammatory Biomarkers and Its Role in Future Therapeutic StrategiesDocument6 pagesImpact of Coenzyme Q10 On Inflammatory Biomarkers and Its Role in Future Therapeutic StrategiesMichael Kohlberger, BSc MScPas encore d'évaluation
- Mmunotec Edical UblicationsDocument23 pagesMmunotec Edical Ublicationsapi-26034055Pas encore d'évaluation
- Co Enzyme Q10's Potential Aids Chronic Condition SymptomsDocument2 pagesCo Enzyme Q10's Potential Aids Chronic Condition Symptomsraliaga59Pas encore d'évaluation
- A Pilot Study of Vidofludimus Calcium For Treatment of Primary Sclerosing CholangitisDocument9 pagesA Pilot Study of Vidofludimus Calcium For Treatment of Primary Sclerosing CholangitisrachelPas encore d'évaluation
- Fecal Calprotectin in IBDDocument34 pagesFecal Calprotectin in IBDNathania Nadia BudimanPas encore d'évaluation
- Fecal Calprotectin in IBDDocument34 pagesFecal Calprotectin in IBDNathania Nadia Budiman100% (1)
- FK concentration in celiac diseaseDocument3 pagesFK concentration in celiac diseaseNejc KovačPas encore d'évaluation
- Coq10 As Ubiquinone & Ubiquinol:: For Cardiovascular Health & MoreDocument3 pagesCoq10 As Ubiquinone & Ubiquinol:: For Cardiovascular Health & MorekPas encore d'évaluation
- 10 1210@clinem@dgaa336 PDFDocument37 pages10 1210@clinem@dgaa336 PDFAuliya BintanPas encore d'évaluation
- nutrients-12-01423Document14 pagesnutrients-12-01423Nejc KovačPas encore d'évaluation
- CoQ10 and the treatment of periodontitisDocument8 pagesCoQ10 and the treatment of periodontitismichael DariasPas encore d'évaluation
- Update On Cancer CachexiaDocument4 pagesUpdate On Cancer CachexiaIyanPas encore d'évaluation
- Impact of Synbiotics and Urate-Lowering Therapy on Gut Microbiota and CytokinesDocument9 pagesImpact of Synbiotics and Urate-Lowering Therapy on Gut Microbiota and CytokinesBagastyoPas encore d'évaluation
- Research Proposal Final ProjectDocument16 pagesResearch Proposal Final Projectapi-534383603Pas encore d'évaluation
- Fungi & Cancer TherapyDocument18 pagesFungi & Cancer TherapyLynn McdonaldPas encore d'évaluation
- Gut Dysbiosis and Fecal Calprotectin Predict Response to Immune CheckpointDocument10 pagesGut Dysbiosis and Fecal Calprotectin Predict Response to Immune CheckpointMartinaPas encore d'évaluation
- Coenzyme Q10 (Coq10) : Nccih - Nih.GovDocument6 pagesCoenzyme Q10 (Coq10) : Nccih - Nih.GovCameronPas encore d'évaluation
- Cognitive Concept Map - Case of The Week - USMLE Genetics - All About Cystic Fibrosis (CF) - DR Kumar Ponnusamy & DR Jegathambigai RNDocument2 pagesCognitive Concept Map - Case of The Week - USMLE Genetics - All About Cystic Fibrosis (CF) - DR Kumar Ponnusamy & DR Jegathambigai RNPonnusamy KumarPas encore d'évaluation
- ERC PotasioDocument10 pagesERC PotasioAbrilPas encore d'évaluation
- Thno 54961r2 3Document45 pagesThno 54961r2 3Eduardo JuarezPas encore d'évaluation
- Nutricion PerioperatoriaDocument11 pagesNutricion PerioperatoriaAndres Neira QuezadaPas encore d'évaluation
- Abstract. Vascular Endothelial Growth Factor (VEGF) Report-: ONCOLOGY LETTERS 5: 1682-1686, 2013Document5 pagesAbstract. Vascular Endothelial Growth Factor (VEGF) Report-: ONCOLOGY LETTERS 5: 1682-1686, 2013yuliaPas encore d'évaluation
- A Randomized, Placebo-Controlled, Pilot ClinicalDocument10 pagesA Randomized, Placebo-Controlled, Pilot ClinicalJUAN SEBASTIAN AVELLANEDA MARTINEZPas encore d'évaluation
- BiomedicinesDocument22 pagesBiomedicinesJohn BartleyPas encore d'évaluation
- Nutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalDocument4 pagesNutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalhafiezAmandaPas encore d'évaluation
- 2003 Probiotic and IBDDocument5 pages2003 Probiotic and IBDsujata sharmaPas encore d'évaluation
- Scientific Evidence Underlying Contraindications TDocument11 pagesScientific Evidence Underlying Contraindications TChon ChiPas encore d'évaluation
- One 64 Citations 23 AbstractsDocument21 pagesOne 64 Citations 23 Abstractsapi-3714923Pas encore d'évaluation
- Kwashiorkor - ProQuest CentralDocument4 pagesKwashiorkor - ProQuest CentralDrbee10Pas encore d'évaluation
- A Low Carbohydrate, High Protein Diet Slows Tumor Growth and Prevents Cancer InitiationDocument11 pagesA Low Carbohydrate, High Protein Diet Slows Tumor Growth and Prevents Cancer Initiationanna.andreouu321Pas encore d'évaluation
- Nutritional Support in Patients With Oesophageal CancerDocument10 pagesNutritional Support in Patients With Oesophageal Cancersinghurvashi365Pas encore d'évaluation
- Nanoparticle-Mediated-Therapeutic-Approach-for-Ulcerative-Colitis-TreatmentDocument22 pagesNanoparticle-Mediated-Therapeutic-Approach-for-Ulcerative-Colitis-TreatmentAchudan JiiPas encore d'évaluation
- A prospective pilot study of a gluten‐free diet for primary sclerosingDocument13 pagesA prospective pilot study of a gluten‐free diet for primary sclerosingNejc KovačPas encore d'évaluation
- Li 2021Document8 pagesLi 2021Neil Patrick AngelesPas encore d'évaluation
- Cell EncapsulationDocument7 pagesCell EncapsulationmitkazPas encore d'évaluation
- Colitis Microscópica y Gluten InglésDocument18 pagesColitis Microscópica y Gluten InglésjaznarPas encore d'évaluation
- GlutathioneDocument4 pagesGlutathionegeraldi23Pas encore d'évaluation
- MD 1 Section E2 Group 3 Biochem REVISEDDocument10 pagesMD 1 Section E2 Group 3 Biochem REVISEDParadoxistPas encore d'évaluation
- Critical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TDocument12 pagesCritical Reviews in Oncology / Hematology: F. Bozzetti, Z. Stanga TshangrilaPas encore d'évaluation
- New Mechanisms and The Anti-Inflammatory Role of Curcumin in Obesity and Obesity-Related Metabolic DiseasesDocument11 pagesNew Mechanisms and The Anti-Inflammatory Role of Curcumin in Obesity and Obesity-Related Metabolic DiseasessudirmanahdiPas encore d'évaluation
- Pediatric Ulcerative Colitis: Diagnosis and Management ChallengesDocument2 pagesPediatric Ulcerative Colitis: Diagnosis and Management ChallengesicoanamarePas encore d'évaluation
- Klek 2014Document24 pagesKlek 2014S Dian RPas encore d'évaluation
- Ulcerative Colitis in ChildrenDocument5 pagesUlcerative Colitis in ChildrentheservantPas encore d'évaluation
- Effects of Specific Nutrients On Immune Modulation in PatientsDocument7 pagesEffects of Specific Nutrients On Immune Modulation in Patientsusuario101122Pas encore d'évaluation
- Ketosis Suppression and AgeingDocument31 pagesKetosis Suppression and AgeingMr XPas encore d'évaluation
- Mitochondria Supplements PDFDocument9 pagesMitochondria Supplements PDFDownTheTheRabbitHole108Pas encore d'évaluation
- Coenzyme q10pdfDocument29 pagesCoenzyme q10pdfMyPSA PHCPas encore d'évaluation
- Nutrients 14 02469 v2Document21 pagesNutrients 14 02469 v2Roxana CristeaPas encore d'évaluation
- Vitamin K and Osteoporosis: Nutraceutical Profile (September 2009)Document12 pagesVitamin K and Osteoporosis: Nutraceutical Profile (September 2009)Dinda AprilianiPas encore d'évaluation
- Malnutrition Induced by Cancer and Oncology TreatmentDocument8 pagesMalnutrition Induced by Cancer and Oncology TreatmentSemira ČanićPas encore d'évaluation
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraPas encore d'évaluation
- Colitis UlcerativaDocument20 pagesColitis UlcerativaMargareth Vargas BéjarPas encore d'évaluation
- Indeterminate ColitisDocument26 pagesIndeterminate ColitisMarlisa YanuartiPas encore d'évaluation
- 467 788 1 SMDocument14 pages467 788 1 SMSelia ApriyaniPas encore d'évaluation
- Probiotics Improve Long Covid PDFDocument9 pagesProbiotics Improve Long Covid PDFSANTA HILDEGARDA DE BINGEN100% (1)
- Sunday O. Oyedemi - Godswill Nwaogu - Chika I. Chukwuma - Olaoluwa T. Adeyemi - Motlalepula G. Matsabisa - Shasank S. Swain - Olayinka A. AiyegoroDocument16 pagesSunday O. Oyedemi - Godswill Nwaogu - Chika I. Chukwuma - Olaoluwa T. Adeyemi - Motlalepula G. Matsabisa - Shasank S. Swain - Olayinka A. AiyegoroGiovanni OliveiraPas encore d'évaluation
- Coq 10 EnergyDocument2 pagesCoq 10 Energyapi-286138040Pas encore d'évaluation
- Celiac Disease FinalDocument7 pagesCeliac Disease FinalacholinePas encore d'évaluation
- Prison Camp LatheDocument6 pagesPrison Camp LatheChukwuRapPas encore d'évaluation
- FertDocument7 pagesFertBibi NiniPas encore d'évaluation
- DemoDocument4 pagesDemoAnonymous mKdAfWifPas encore d'évaluation
- Prison Camp LatheDocument6 pagesPrison Camp LatheChukwuRapPas encore d'évaluation
- Solidworks:: Lesson 1 - Basics and Modeling FundamentalsDocument48 pagesSolidworks:: Lesson 1 - Basics and Modeling FundamentalsmekoxxxPas encore d'évaluation
- Primena 3D Stampe U ObrazovanjuDocument4 pagesPrimena 3D Stampe U ObrazovanjuAnonymous mKdAfWifPas encore d'évaluation
- S.E Mechanical EngineeringDocument35 pagesS.E Mechanical EngineeringRahul KalathilPas encore d'évaluation
- Taper Basics PDFDocument3 pagesTaper Basics PDFAnonymous mKdAfWifPas encore d'évaluation
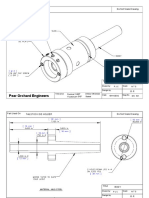
- Pear Orchard Engineers: Do Not Scale Drawing Part Used OnDocument4 pagesPear Orchard Engineers: Do Not Scale Drawing Part Used OnAnonymous mKdAfWifPas encore d'évaluation
- Home Shop Machinist's Gears GuideDocument8 pagesHome Shop Machinist's Gears Guidegaragepunkfan100% (1)
- En Metalwork General Metal WorkDocument90 pagesEn Metalwork General Metal WorkAnonymous mKdAfWifPas encore d'évaluation
- Owners Manual 4 The Human BodyDocument184 pagesOwners Manual 4 The Human BodyAnonymous mKdAfWifPas encore d'évaluation
- Three Wire MethodDocument4 pagesThree Wire MethodmaivizhiPas encore d'évaluation
- Machining Operations and Machine ToolsDocument18 pagesMachining Operations and Machine ToolsAnonymous mKdAfWifPas encore d'évaluation
- GearsDocument4 pagesGearsR@XPas encore d'évaluation
- Zadatak 1a Vitlo SkidDocument2 018 pagesZadatak 1a Vitlo SkidAnonymous mKdAfWifPas encore d'évaluation
- 01 MaterialsDocument6 pages01 MaterialsAnonymous mKdAfWifPas encore d'évaluation
- ZlatarstvoDocument1 pageZlatarstvokosinPas encore d'évaluation
- Casting Elwany FullDocument22 pagesCasting Elwany FullAnonymous mKdAfWifPas encore d'évaluation
- 08 Milling Full SlidesDocument35 pages08 Milling Full SlidesAnonymous mKdAfWifPas encore d'évaluation
- Testing Lathe For AccuracyDocument4 pagesTesting Lathe For AccuracyArnieTPas encore d'évaluation
- A Few Project Images: Tool Posts Lathe Cutting ToolsDocument4 pagesA Few Project Images: Tool Posts Lathe Cutting ToolsAnonymous mKdAfWifPas encore d'évaluation
- Workshop Practice Series - BooksDocument8 pagesWorkshop Practice Series - Bookscatapix100% (5)
- Machining Processes Used To Produce Round Shapes: Turning and Hole MakingDocument36 pagesMachining Processes Used To Produce Round Shapes: Turning and Hole MakingAnonymous mKdAfWif0% (1)
- 11-Turning Equations FullDocument21 pages11-Turning Equations FullmagzigioPas encore d'évaluation
- Atlas Cut-Off Tools PDFDocument2 pagesAtlas Cut-Off Tools PDFhugo@wideas.comPas encore d'évaluation
- Working Drawings-Full SlidesDocument14 pagesWorking Drawings-Full SlidesAnonymous mKdAfWifPas encore d'évaluation
- Machining Operations and Machine ToolsDocument18 pagesMachining Operations and Machine ToolsAnonymous mKdAfWifPas encore d'évaluation
- Prison Camp LatheDocument6 pagesPrison Camp LatheChukwuRapPas encore d'évaluation
- IC Learning Series 2012 - Metal Cutting Processes - TurningDocument15 pagesIC Learning Series 2012 - Metal Cutting Processes - TurningSorin FrentoniPas encore d'évaluation