Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
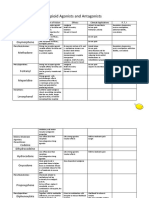
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Septic Shock TreatmentDocument22 pagesSeptic Shock TreatmentAdreiTheTripleA100% (1)
- Narcotics Controlled Drugs TableDocument4 pagesNarcotics Controlled Drugs TableDurgaNadellaPas encore d'évaluation
- Schedule of Controlled DrugsDocument1 pageSchedule of Controlled DrugsKaye AbordoPas encore d'évaluation
- Vicodin Drug Study Que Fransis A.Document3 pagesVicodin Drug Study Que Fransis A.Irene Grace BalcuevaPas encore d'évaluation
- Classification of Drugs and Their EffectsDocument3 pagesClassification of Drugs and Their EffectsshriPas encore d'évaluation
- Huruf ANDocument3 pagesHuruf ANAdreiTheTripleAPas encore d'évaluation
- Z and Z and A and B and C and D and e and FDocument124 pagesZ and Z and A and B and C and D and e and FAdreiTheTripleAPas encore d'évaluation
- Huruf AHDocument3 pagesHuruf AHAdreiTheTripleAPas encore d'évaluation
- Laporan Transaksi: No. Rekening Nama Produk Mata Uang Nomor CIFDocument2 pagesLaporan Transaksi: No. Rekening Nama Produk Mata Uang Nomor CIFAdreiTheTripleAPas encore d'évaluation
- Huruf AADocument3 pagesHuruf AAAdreiTheTripleAPas encore d'évaluation
- Huruf LDocument3 pagesHuruf LAdreiTheTripleAPas encore d'évaluation
- Huruf UDocument3 pagesHuruf UAdreiTheTripleAPas encore d'évaluation
- Huruf VDocument3 pagesHuruf VAdreiTheTripleAPas encore d'évaluation
- Huruf JDocument3 pagesHuruf JAdreiTheTripleAPas encore d'évaluation
- 2014 AHA/ACC Guideline for NSTE-ACS ManagementDocument151 pages2014 AHA/ACC Guideline for NSTE-ACS ManagementParadina WulandariPas encore d'évaluation
- Huruf RDocument3 pagesHuruf RAdreiTheTripleAPas encore d'évaluation
- Huruf TDocument3 pagesHuruf TAdreiTheTripleAPas encore d'évaluation
- Huruf GDocument3 pagesHuruf GAdreiTheTripleAPas encore d'évaluation
- GOLD Pocket Guide 2014 COPDDocument32 pagesGOLD Pocket Guide 2014 COPDNatalia CvPas encore d'évaluation
- Huruf ADocument3 pagesHuruf AAdreiTheTripleAPas encore d'évaluation
- Global Initiative For Chronic Obstructive Lung Disease. Update 2014Document102 pagesGlobal Initiative For Chronic Obstructive Lung Disease. Update 2014Guss LopezPas encore d'évaluation
- Myasthenia Gravis: Practice EssentialsDocument12 pagesMyasthenia Gravis: Practice EssentialsAdreiTheTripleA0% (1)
- Huruf eDocument3 pagesHuruf eAdreiTheTripleAPas encore d'évaluation
- Delusions of ParasitosisDocument5 pagesDelusions of ParasitosisAdreiTheTripleAPas encore d'évaluation
- Cutaneous Larva Migrans - Doctor - Patient - CoDocument5 pagesCutaneous Larva Migrans - Doctor - Patient - CoAdreiTheTripleAPas encore d'évaluation
- The Future of Diagnosis, Theraphy and ProphylaxisDocument11 pagesThe Future of Diagnosis, Theraphy and ProphylaxisAdreiTheTripleAPas encore d'évaluation
- Congenital NeviDocument6 pagesCongenital NeviAdreiTheTripleAPas encore d'évaluation
- Guillain Barre SyndromeDocument13 pagesGuillain Barre SyndromeAdreiTheTripleAPas encore d'évaluation
- Pa Pill EdemaDocument3 pagesPa Pill EdemaAdreiTheTripleAPas encore d'évaluation
- Choking - Infant Under 1 Year - MedlinePlus Medical Encyclopedia (Print Version)Document3 pagesChoking - Infant Under 1 Year - MedlinePlus Medical Encyclopedia (Print Version)AdreiTheTripleAPas encore d'évaluation
- Malignant MelanomaDocument12 pagesMalignant MelanomaAdreiTheTripleAPas encore d'évaluation
- Heimlich Maneuver - MedlinePlus Medical Encyclopedia (Print Version)Document2 pagesHeimlich Maneuver - MedlinePlus Medical Encyclopedia (Print Version)AdreiTheTripleAPas encore d'évaluation
- Distributive Shock PDFDocument8 pagesDistributive Shock PDFAdreiTheTripleAPas encore d'évaluation
- Analgesic & AntipyreticsDocument7 pagesAnalgesic & AntipyreticsRaymund RazonPas encore d'évaluation
- Oral Oxycodone For Acute Postoperative PainDocument20 pagesOral Oxycodone For Acute Postoperative PainArmi ZakaPas encore d'évaluation
- Suboxone Brochure LKDDocument2 pagesSuboxone Brochure LKDJohn McconnellPas encore d'évaluation
- Obat PatenDocument8 pagesObat PatenrismaPas encore d'évaluation
- FentanylDocument11 pagesFentanylJereel Hope BaconPas encore d'évaluation
- Etonitazene - An Opioid Selective For The Mu Receptor Types - Moolten MS, Fishman JB, Chen JC, Carlson KR - Life Sci 52 (1993) PL199-PL203Document5 pagesEtonitazene - An Opioid Selective For The Mu Receptor Types - Moolten MS, Fishman JB, Chen JC, Carlson KR - Life Sci 52 (1993) PL199-PL203muopioidreceptorPas encore d'évaluation
- Project Dawn Brochure0515Document2 pagesProject Dawn Brochure0515api-265745737Pas encore d'évaluation
- Latest List of Monitored Drugs in Ontario (2016)Document40 pagesLatest List of Monitored Drugs in Ontario (2016)roxiemannPas encore d'évaluation
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDocument10 pagesRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFMiftah JannahPas encore d'évaluation
- Fentanyl Fact SheetDocument2 pagesFentanyl Fact SheetSinclair Broadcast Group - EugenePas encore d'évaluation
- Opioid Conversion Chart 2020 1Document1 pageOpioid Conversion Chart 2020 1aengus42Pas encore d'évaluation
- ترجمه PDFDocument4 pagesترجمه PDFAshkan Abbasi0% (1)
- FORMULA PARACETAMOL ANALGESICOSDocument3 pagesFORMULA PARACETAMOL ANALGESICOSDanilo M MadanesPas encore d'évaluation
- Literature ReviewDocument3 pagesLiterature Reviewapi-609233193Pas encore d'évaluation
- 6.2 Opioid & Non-OpioidsDocument18 pages6.2 Opioid & Non-OpioidsAsem AlhazmiPas encore d'évaluation
- Opioid AnalgesicsDocument29 pagesOpioid AnalgesicsamonlisaPas encore d'évaluation
- T Wycross 1984Document6 pagesT Wycross 1984Ha HaPas encore d'évaluation
- Opioid Rotation Conversion Learning PackageDocument18 pagesOpioid Rotation Conversion Learning Packagepaul casillasPas encore d'évaluation
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDocument13 pagesRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFFarmasi Bunda WadungasriPas encore d'évaluation
- Atestat 1Document22 pagesAtestat 1RalucaxdPas encore d'évaluation
- Sudnaloxonesuboxone 8Document2 pagesSudnaloxonesuboxone 8api-665140662Pas encore d'évaluation
- Dangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFDocument11 pagesDangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFdesmond100% (1)
- 2019 Aiken County Accidental OverdosesDocument1 page2019 Aiken County Accidental OverdosesJeremy TurnagePas encore d'évaluation
- List of Schedule I Drugs (US) - Wikipedia, The Free EncyclopediaDocument7 pagesList of Schedule I Drugs (US) - Wikipedia, The Free EncyclopediaterterdgdfgdfgdfgfdgPas encore d'évaluation
- NaloxBox Press Event Agenda and News ReleaseDocument5 pagesNaloxBox Press Event Agenda and News ReleaseABC6/FOX28Pas encore d'évaluation