Vous aimerez peut-être aussi
- Coronary Artery DiseaseDocument9 pagesCoronary Artery DiseaseMariquita Buenafe100% (1)
- Activity Intolerance NCPDocument7 pagesActivity Intolerance NCPMariquita BuenafePas encore d'évaluation
- Medical Health Examination FormDocument4 pagesMedical Health Examination FormAldwin Bagtas0% (1)
- Surgery QuestionsDocument19 pagesSurgery QuestionsdocaliPas encore d'évaluation
- Uterine Prolaps1Document6 pagesUterine Prolaps1Ginsha GeorgePas encore d'évaluation
- Focus ChartingDocument3 pagesFocus ChartingMan GatuankoPas encore d'évaluation
- CPR SeminarDocument76 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (3)
- Drug StudyDocument11 pagesDrug StudyJohn Lucas100% (2)
- CardiomegalyDocument91 pagesCardiomegalyMariquita Buenafe100% (1)
- NCP RHDocument3 pagesNCP RHMariquita Buenafe57% (7)
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- Nursing Care Plan For Syphilis Nursing NotesDocument4 pagesNursing Care Plan For Syphilis Nursing Notesblaire100% (1)
- Drug Study (Misoprostol)Document3 pagesDrug Study (Misoprostol)Danica NuevaexcijaPas encore d'évaluation
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarPas encore d'évaluation
- DextroseDocument1 pageDextroseAdrianne BazoPas encore d'évaluation
- Kanski'S: Clinical OphthalmologyDocument504 pagesKanski'S: Clinical OphthalmologyMohin hossain100% (1)
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDocument6 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Drug Study On MAGNESIUM SULFATEDocument6 pagesDrug Study On MAGNESIUM SULFATEshadow gonzalezPas encore d'évaluation
- Module2 Day2 MetaparadigmDocument39 pagesModule2 Day2 MetaparadigmRon OpulenciaPas encore d'évaluation
- Methods of Contraception or Family PlanningDocument2 pagesMethods of Contraception or Family PlanningAngel EsperePas encore d'évaluation
- Generic NameDocument6 pagesGeneric NameKimsha ConcepcionPas encore d'évaluation
- Maternity and Newborn MedicationsDocument38 pagesMaternity and Newborn MedicationsJaypee Fabros EdraPas encore d'évaluation
- Drug Study ON Cabergolin EDocument4 pagesDrug Study ON Cabergolin ESimran SimzPas encore d'évaluation
- AntaraDocument13 pagesAntaraDeepti KukretiPas encore d'évaluation
- Levonorgestrel: Mechanism of ActionDocument6 pagesLevonorgestrel: Mechanism of ActionAdditi SatyalPas encore d'évaluation
- INDOMETACINDocument5 pagesINDOMETACINteslimolakunlerajiPas encore d'évaluation
- PethidineDocument9 pagesPethidineAnonymous VZtcCECtPas encore d'évaluation
- Intra NatalDocument1 pageIntra NatalIche Dela Cruz100% (1)
- Methyldopa, Losartan K, Ascorbic AcidDocument4 pagesMethyldopa, Losartan K, Ascorbic AcidRico Mae ValenciaPas encore d'évaluation
- Methylergonovine MaleateDocument2 pagesMethylergonovine MaleateRitamariaPas encore d'évaluation
- Obat ObgynDocument8 pagesObat ObgynMuhammad Naqiuddin JalaluddinPas encore d'évaluation
- Drug Study On METHERGINEDocument4 pagesDrug Study On METHERGINEshadow gonzalezPas encore d'évaluation
- Betnesol InjectionDocument7 pagesBetnesol Injectionhiral mistryPas encore d'évaluation
- CeftriaxoneDocument5 pagesCeftriaxoneCastillo MikaellaPas encore d'évaluation
- Oligohydramnios - Etiology, Diagnosis, and Management - UpToDateDocument23 pagesOligohydramnios - Etiology, Diagnosis, and Management - UpToDateJUAN FRANCISCO OSORIO PENALOZAPas encore d'évaluation
- Prazosin Tablet (Prazosin)Document6 pagesPrazosin Tablet (Prazosin)Chenta Bulan MerinduPas encore d'évaluation
- Labetalol Hydro ChlorideDocument3 pagesLabetalol Hydro Chlorideapi-3797941100% (1)
- Beractant: Drug Class Therapeutic ActionsDocument4 pagesBeractant: Drug Class Therapeutic ActionsPrincess BartolomePas encore d'évaluation
- UTERINE PROLAPSE - Case ReportDocument3 pagesUTERINE PROLAPSE - Case ReportIOSRjournalPas encore d'évaluation
- Roxipan (Oxytocin) - Drug StudyDocument4 pagesRoxipan (Oxytocin) - Drug StudyIzza DeloriaPas encore d'évaluation
- MethergineDocument3 pagesMethergineJohn AlanoPas encore d'évaluation
- MetherginDocument2 pagesMetherginOtan Cuison100% (1)
- Magnesium SulfateDocument2 pagesMagnesium SulfateGwyn Rosales100% (1)
- A Study To Assess The Knowledge of Primi Gravida Mother Regarding Importance Colostrum at Selected Hospital Bagalkot Karnataka, IndiaDocument10 pagesA Study To Assess The Knowledge of Primi Gravida Mother Regarding Importance Colostrum at Selected Hospital Bagalkot Karnataka, IndiaInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785Pas encore d'évaluation
- Nahco3 Vancomycin AmlodipineDocument3 pagesNahco3 Vancomycin AmlodipineShan Dave TupasPas encore d'évaluation
- Generic Name:: ClassificationsDocument4 pagesGeneric Name:: ClassificationsbillyktoubattsPas encore d'évaluation
- Generic Name:: Norgestimate and Ethinyl EstradiolDocument5 pagesGeneric Name:: Norgestimate and Ethinyl EstradiolJay VillasotoPas encore d'évaluation
- PrimaquineDocument3 pagesPrimaquineVijayakumar NsPas encore d'évaluation
- Drug Study ObDocument6 pagesDrug Study Obednaria100% (1)
- Stugeron® TabletsDocument3 pagesStugeron® TabletsmahgadPas encore d'évaluation
- Cefoperazone and SulbactumDocument3 pagesCefoperazone and Sulbactumiloveit52252Pas encore d'évaluation
- NCP Fever 1Document11 pagesNCP Fever 1Deepak VermaPas encore d'évaluation
- Carboprost TromethamineDocument2 pagesCarboprost TromethamineDeathDefying DonutPas encore d'évaluation
- TerminologyDocument38 pagesTerminologypandem soniyaPas encore d'évaluation
- CELINDocument9 pagesCELINaikoestrellaPas encore d'évaluation
- Drug Presentation On AminophyllineDocument10 pagesDrug Presentation On Aminophyllineelisha immanuelPas encore d'évaluation
- A Case Study On MastitisDocument15 pagesA Case Study On MastitisAnil Sigdel100% (3)
- Case StudyDocument19 pagesCase Studywella goPas encore d'évaluation
- ParacetamolDocument2 pagesParacetamolBlesyl Sison Mabano100% (1)
- Magnesium Sulfate Drug StudyDocument3 pagesMagnesium Sulfate Drug StudyMonica Lyka BancalePas encore d'évaluation
- Albendazol PDFDocument8 pagesAlbendazol PDFDANIBATAPas encore d'évaluation
- Drug Study - CefotaximeDocument5 pagesDrug Study - CefotaximeAngel laurestaPas encore d'évaluation
- Drug StudyDocument21 pagesDrug StudyRemedios Bandong100% (1)
- Drug StudyDocument32 pagesDrug StudyKeepItSecretPas encore d'évaluation
- Amniotic Fluid EmbolismDocument19 pagesAmniotic Fluid EmbolismStar Alvarez100% (1)
- Vii. Drug Study Drug Mechanism of ActionDocument7 pagesVii. Drug Study Drug Mechanism of ActionRifa'atul MahmudahPas encore d'évaluation
- UNIT XIII Drugs Affecting The Reproductive SystemDocument90 pagesUNIT XIII Drugs Affecting The Reproductive Systemrichardmd2100% (1)
- Estradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)Document12 pagesEstradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)ddandan_2Pas encore d'évaluation
- Prostin E2 Vaginal Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document5 pagesProstin E2 Vaginal Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)NousheenPas encore d'évaluation
- UrinalysisDocument5 pagesUrinalysisMariquita BuenafePas encore d'évaluation
- Effects of Aging in The Cardiovascular SystemDocument6 pagesEffects of Aging in The Cardiovascular SystemMariquita BuenafePas encore d'évaluation
- Journal in PediatricsDocument7 pagesJournal in PediatricsMariquita BuenafePas encore d'évaluation
- Pedia Drugs ImagesDocument1 pagePedia Drugs ImagesMariquita BuenafePas encore d'évaluation
- CHN - Drug StudyDocument1 pageCHN - Drug StudyMariquita BuenafePas encore d'évaluation
- Acute PancreatitisDocument20 pagesAcute PancreatitisMariquita BuenafePas encore d'évaluation
- Journal in Anemia and BTDocument19 pagesJournal in Anemia and BTMariquita BuenafePas encore d'évaluation
- Hemolytic Disease of The Fetus and Newborn JournalDocument10 pagesHemolytic Disease of The Fetus and Newborn JournalMariquita BuenafePas encore d'évaluation
- Pathophysiology of Erythroblastosis Fetalis - RH IsoimmunizationDocument1 pagePathophysiology of Erythroblastosis Fetalis - RH IsoimmunizationRalph Delos SantosPas encore d'évaluation
- DR DrugsDocument2 pagesDR DrugsMariquita BuenafePas encore d'évaluation
- Drugs Study For Surgery WardDocument4 pagesDrugs Study For Surgery WardMariquita BuenafePas encore d'évaluation
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafePas encore d'évaluation
- DengueDocument5 pagesDengueMariquita BuenafePas encore d'évaluation
- Cardio Drug StudyDocument8 pagesCardio Drug StudyMariquita BuenafePas encore d'évaluation
- DR DrugsDocument2 pagesDR DrugsMariquita BuenafePas encore d'évaluation
- Cardio Drug StudyDocument8 pagesCardio Drug StudyMariquita BuenafePas encore d'évaluation
- Cardio Drug StudyDocument8 pagesCardio Drug StudyMariquita BuenafePas encore d'évaluation
- Pediatric Nursing FinalDocument35 pagesPediatric Nursing FinalMariquita BuenafePas encore d'évaluation
- Coronary Artery DiseaseDocument38 pagesCoronary Artery DiseaseMariquita BuenafePas encore d'évaluation
- PromDocument14 pagesPromMariquita BuenafePas encore d'évaluation
- Diagnosis and Management in Peripheral Artery Disease EditedDocument5 pagesDiagnosis and Management in Peripheral Artery Disease Editedwahyu suparnoPas encore d'évaluation
- Drug Study NCMHDocument5 pagesDrug Study NCMHnhycePas encore d'évaluation
- Nelson EmbriologiDocument88 pagesNelson Embriologisheryn pujionoPas encore d'évaluation
- InotroposDocument4 pagesInotroposjuan camiloPas encore d'évaluation
- Chapter 9 KeyDocument17 pagesChapter 9 KeySrinu WestPas encore d'évaluation
- Moderator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhDocument119 pagesModerator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhMunish DograPas encore d'évaluation
- Care of The Post-Thrombectomy Patient: Topical ReviewDocument7 pagesCare of The Post-Thrombectomy Patient: Topical ReviewBasilio BabarPas encore d'évaluation
- Hepatorenal Syndrome: Pathophysiology, Diagnosis, and ManagementDocument21 pagesHepatorenal Syndrome: Pathophysiology, Diagnosis, and Managementkonas patklinPas encore d'évaluation
- Top 10 Takeaways Clinicians - UpdatedDocument1 pageTop 10 Takeaways Clinicians - UpdatedBea Barbara CarrascalPas encore d'évaluation
- Vascular Supply To The BrainDocument38 pagesVascular Supply To The BrainGhea Putri HendrianiPas encore d'évaluation
- Amlodipine ReadingDocument12 pagesAmlodipine Readingines pachecoPas encore d'évaluation
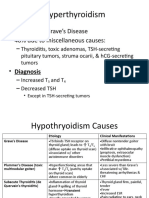
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.Pas encore d'évaluation
- 2 Patient Assessment Pocket DentistryDocument1 page2 Patient Assessment Pocket DentistryVictor FanPas encore d'évaluation
- Review Notes For Diabetes MellitusDocument8 pagesReview Notes For Diabetes MellitusEditha LucasPas encore d'évaluation
- Circulatory SystemDocument18 pagesCirculatory SystemgorgeouslypoisonedPas encore d'évaluation
- ZOOL30040 Practical HandoutDocument10 pagesZOOL30040 Practical Handoutannabelledarcy247Pas encore d'évaluation
- Heat Stroke in Dogs Literature ReviewDocument11 pagesHeat Stroke in Dogs Literature ReviewGuillermo MuzasPas encore d'évaluation
- College of Nursing: Pharmacology Drug StudyDocument1 pageCollege of Nursing: Pharmacology Drug StudyChristine Pialan SalimbagatPas encore d'évaluation
- 11 Anti-Coagulants & FibrinolyticsDocument52 pages11 Anti-Coagulants & FibrinolyticsUmmuShefaPas encore d'évaluation
- Path Pancreas McqsDocument4 pagesPath Pancreas McqsUu UuPas encore d'évaluation
- Endothelial Dysfunction in Diabetic Erectile DysfunctionDocument11 pagesEndothelial Dysfunction in Diabetic Erectile DysfunctionILham SyahPas encore d'évaluation
- CPG Management of StrokeDocument51 pagesCPG Management of Strokeapalaginih0% (1)
- Aldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Document72 pagesAldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Parvathy R NairPas encore d'évaluation
- Ayuno Intermitente Test 2Document16 pagesAyuno Intermitente Test 2Denisse San MartínPas encore d'évaluation
- SBIL - Health QuestionnaireDocument2 pagesSBIL - Health QuestionnaireKrishna GBPas encore d'évaluation