Vous aimerez peut-être aussi
- Sample Chapter of Maternal-Neonatal Care Made Incredibly Easy! 1st UK EditionDocument74 pagesSample Chapter of Maternal-Neonatal Care Made Incredibly Easy! 1st UK EditionLippincott Williams and Wilkins- EuropePas encore d'évaluation
- 13 LinensDocument8 pages13 LinensKhaleed Dela RamaPas encore d'évaluation
- Complete Urinalysis: A. Physical Characteristics of UrineDocument8 pagesComplete Urinalysis: A. Physical Characteristics of UrineKryza Dale Bunado BaticanPas encore d'évaluation
- Maternal QuestionsDocument7 pagesMaternal Questionsjhae_darilayPas encore d'évaluation
- Labor&DeliveryDocument8 pagesLabor&Deliverytomrey1533Pas encore d'évaluation
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlPas encore d'évaluation
- Nursing ProcessDocument62 pagesNursing ProcessplethoraldorkPas encore d'évaluation
- Assessing Community Health Needs in San Isidro East, PhilippinesDocument14 pagesAssessing Community Health Needs in San Isidro East, PhilippinesSarah Agudo FernandezPas encore d'évaluation
- Antepartum Notes Maternal and Child NursingDocument12 pagesAntepartum Notes Maternal and Child NursingJoana Rose FantonialPas encore d'évaluation
- What is an NCPDocument38 pagesWhat is an NCPSARAH DIANA ROSE S. MANALILI100% (1)
- CasestudyutiDocument21 pagesCasestudyutidael_05Pas encore d'évaluation
- Determine Gestational Age Using LMP and UltrasoundDocument18 pagesDetermine Gestational Age Using LMP and UltrasoundMomshie Felaih Binasoy Dela Cruz100% (1)
- IMCI - Chart BookletDocument39 pagesIMCI - Chart BookletJason MirasolPas encore d'évaluation
- Case Scenario For Different Groups PDFDocument8 pagesCase Scenario For Different Groups PDFWallen Jey VelascoPas encore d'évaluation
- Nursing ProcessDocument8 pagesNursing ProcessGhadeer Hijazeen100% (1)
- Antenatal Care: Physiological Changes in PregnancyDocument2 pagesAntenatal Care: Physiological Changes in PregnancyAlexander Ennes100% (1)
- Chapter 001Document8 pagesChapter 001Lisa SzyszkaPas encore d'évaluation
- Chapter 18 Thermal Injuries (Student Copy)Document31 pagesChapter 18 Thermal Injuries (Student Copy)api-287615830Pas encore d'évaluation
- Prenatal AssessmentDocument2 pagesPrenatal AssessmentPrincess Pilove GawongnaPas encore d'évaluation
- Nursing Care of a Family With an Ill ChildDocument17 pagesNursing Care of a Family With an Ill ChildtinaPas encore d'évaluation
- Nursing ProcessDocument131 pagesNursing ProcessYochabel BorjePas encore d'évaluation
- Skin Integrity and Wound CareDocument25 pagesSkin Integrity and Wound CareMarcus, RN89% (9)
- Health Education PlanDocument10 pagesHealth Education PlanJulienne Sanchez-SalazarPas encore d'évaluation
- OB/GYN For EMS ProvidersDocument94 pagesOB/GYN For EMS ProvidersPaulhotvw67100% (6)
- Licensed Practical Nurse, LPN, Nurse Tech, Nurse Aide, Nursing ADocument4 pagesLicensed Practical Nurse, LPN, Nurse Tech, Nurse Aide, Nursing Aapi-121395809Pas encore d'évaluation
- Heat and Cold Therapy Guidelines for Safe ApplicationDocument3 pagesHeat and Cold Therapy Guidelines for Safe ApplicationCamille Monique CortesPas encore d'évaluation
- Postpartum Complications FinalDocument30 pagesPostpartum Complications Finaljacquelinearah100% (1)
- Nursing ProceduresDocument51 pagesNursing ProceduresLouella Mae CoraldePas encore d'évaluation
- Chain of InfectionDocument13 pagesChain of InfectionPrince Jhessie L. AbellaPas encore d'évaluation
- Nursing Jurisprudence and Professional AdjustmentDocument31 pagesNursing Jurisprudence and Professional Adjustmentrtishaii18Pas encore d'évaluation
- Community Health Nursing Case Study of Purok 4-A LuboganDocument84 pagesCommunity Health Nursing Case Study of Purok 4-A LuboganFan XiaoPas encore d'évaluation
- Elder Abuse and NelgectDocument10 pagesElder Abuse and Nelgectنادر القحطانيPas encore d'évaluation
- PAGASA Flood & Earthquake Alert Systems PhilippinesDocument18 pagesPAGASA Flood & Earthquake Alert Systems PhilippinesBokPas encore d'évaluation
- Asepsis and Infection ControlDocument6 pagesAsepsis and Infection ControlgilissaPas encore d'évaluation
- Republic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNDocument167 pagesRepublic Act No. 9173: The Philippine Nursing Act O F 2 0 0 2 Presented By: Judith Leano RNJohnasse Sebastian NavalPas encore d'évaluation
- Introduction To Nursing TheoryDocument44 pagesIntroduction To Nursing TheoryVia SongcalPas encore d'évaluation
- Asthma in PregnancyDocument18 pagesAsthma in Pregnancyms khan0% (1)
- NCMA113 SL RUBRICS Administering Blood TransfusionDocument2 pagesNCMA113 SL RUBRICS Administering Blood TransfusionJoy Ann BasisPas encore d'évaluation
- Exam 1 Study Guide Module Nursing Art ScienceDocument33 pagesExam 1 Study Guide Module Nursing Art Scienceitschloeb100% (1)
- Heart and Blood VesselsDocument16 pagesHeart and Blood Vesselsdlneisha61Pas encore d'évaluation
- The Nursing Role in Reproductive and Sexual Health: Learning OutcomesDocument11 pagesThe Nursing Role in Reproductive and Sexual Health: Learning OutcomesEric GanzanPas encore d'évaluation
- Assessing Childbearing WomenDocument27 pagesAssessing Childbearing WomenJoan Diana100% (1)
- Case Studies Chapter 5Document5 pagesCase Studies Chapter 5Len Abo Ashes100% (1)
- TCB ChecklistDocument3 pagesTCB ChecklistStephanie LiauPas encore d'évaluation
- Checkist For NCM 100 (Skills)Document35 pagesCheckist For NCM 100 (Skills)RazelAnneValinoPas encore d'évaluation
- Introduction to Chronic Kidney DiseaseDocument17 pagesIntroduction to Chronic Kidney DiseaseUlLfa Chii MuetmuethzPas encore d'évaluation
- Case 76Document3 pagesCase 76Yelrebmik OdranrebPas encore d'évaluation
- CHN PRELIM Quiz 1 (2011)Document5 pagesCHN PRELIM Quiz 1 (2011)Amiel Francisco ReyesPas encore d'évaluation
- Chapters 10 To 13Document46 pagesChapters 10 To 13VanessaMUellerPas encore d'évaluation
- Issue Analysis Paper Cultural Competence in Nursing ApplebachDocument18 pagesIssue Analysis Paper Cultural Competence in Nursing Applebachapi-283260051Pas encore d'évaluation
- Decent Work Country Profile PHILIPPINESDocument118 pagesDecent Work Country Profile PHILIPPINESi_am_alvinPas encore d'évaluation
- Review On Peripheral IV FluidsDocument37 pagesReview On Peripheral IV FluidsWoot RootPas encore d'évaluation
- Stages of Labor Nursing ConsiderationsDocument5 pagesStages of Labor Nursing Considerationsneleh gray100% (2)
- Notes On The Complications During The Labor and Delivery ProcessDocument7 pagesNotes On The Complications During The Labor and Delivery ProcessjyzzadPas encore d'évaluation
- Individual Aging Vs Population AgingDocument78 pagesIndividual Aging Vs Population AgingAnonymous iG0DCOf0% (2)
- CopdDocument18 pagesCopdHidy SatorrePas encore d'évaluation
- Incontinence Case StudyDocument26 pagesIncontinence Case StudyRose AnnPas encore d'évaluation
- Assess Eyes, Ears, Nose, Mouth ExamDocument42 pagesAssess Eyes, Ears, Nose, Mouth ExamFranz Earl Niño AlbesaPas encore d'évaluation
- (CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesDocument194 pages(CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesBianca Watanabe - RatillaPas encore d'évaluation
- Acute Myocardial Infarction (AMI) Signs, Diagnosis, TreatmentDocument10 pagesAcute Myocardial Infarction (AMI) Signs, Diagnosis, TreatmentBianca Watanabe - RatillaPas encore d'évaluation
- Hepatitis B QuizDocument2 pagesHepatitis B QuizBianca Watanabe - RatillaPas encore d'évaluation
- CPG Hepatitis BDocument17 pagesCPG Hepatitis BBianca Watanabe - RatillaPas encore d'évaluation
- Liver Pathophysiology and Schematic Diagram BGFJNDocument1 pageLiver Pathophysiology and Schematic Diagram BGFJNKate Mylhen Espenido EnerlanPas encore d'évaluation
- Nag2019 PDFDocument288 pagesNag2019 PDFmashupPas encore d'évaluation
- (CPG) 2021 Clinical Practice Guidelines On The Management of Hepatitis B in The Philippines - Full ManuscriptDocument84 pages(CPG) 2021 Clinical Practice Guidelines On The Management of Hepatitis B in The Philippines - Full ManuscriptKai ChuaPas encore d'évaluation
- (CPG) Philippine Guidelines On Periodic Health Examination: Pediatric ImmunizationDocument171 pages(CPG) Philippine Guidelines On Periodic Health Examination: Pediatric ImmunizationBianca Watanabe - RatillaPas encore d'évaluation
- (CPG) Philippine Guidelines On Periodic Health Examination: Lifestyle AdviceDocument107 pages(CPG) Philippine Guidelines On Periodic Health Examination: Lifestyle AdviceBianca Watanabe - RatillaPas encore d'évaluation
- PNF EmlDocument63 pagesPNF EmlRosaleo Tolibas100% (1)
- Copd ImDocument28 pagesCopd ImBianca Watanabe - RatillaPas encore d'évaluation
- Delivery of Prenatal Health Education and Pregnancy Out ComesDocument9 pagesDelivery of Prenatal Health Education and Pregnancy Out ComesBianca Watanabe - Ratilla0% (1)
- GINA 2021 Guidelines for Asthma Diagnosis and TreatmentDocument24 pagesGINA 2021 Guidelines for Asthma Diagnosis and TreatmentBianca Watanabe - RatillaPas encore d'évaluation
- Title: National and Local Health Situation Venue: Barangay Molocboloc, Alubijid, Misamis Oriental Date: July 16, 2019Document3 pagesTitle: National and Local Health Situation Venue: Barangay Molocboloc, Alubijid, Misamis Oriental Date: July 16, 2019Bianca Watanabe - RatillaPas encore d'évaluation
- Membrane Theory of Aging and Hayflick Limit TheoryDocument12 pagesMembrane Theory of Aging and Hayflick Limit TheoryBianca Watanabe - RatillaPas encore d'évaluation
- Vital Signs Monitoring SheetDocument3 pagesVital Signs Monitoring SheetBianca Watanabe - RatillaPas encore d'évaluation
- Drug StudyDocument2 pagesDrug StudyBianca Watanabe - RatillaPas encore d'évaluation
- Pathophysiology of Blighted OvumDocument4 pagesPathophysiology of Blighted OvumBianca Watanabe - Ratilla100% (2)
- Drug Study - Paracetamol (Calpol)Document1 pageDrug Study - Paracetamol (Calpol)Bianca Watanabe - RatillaPas encore d'évaluation
- Teaching Learning GuideDocument1 pageTeaching Learning GuideBianca Watanabe - RatillaPas encore d'évaluation
- Doctor's Orders: Hypertension ManagementDocument3 pagesDoctor's Orders: Hypertension ManagementBianca Watanabe - RatillaPas encore d'évaluation
- NCP Risk For Imbalanced NutritionDocument2 pagesNCP Risk For Imbalanced NutritionBianca Watanabe - Ratilla63% (8)
- Lactational Amenorrhea MethodDocument9 pagesLactational Amenorrhea MethodBianca Watanabe - Ratilla100% (1)
- ProteinDocument16 pagesProteinGwen Cua50% (2)
- ProteinDocument16 pagesProteinGwen Cua50% (2)
- Anna and The KingDocument5 pagesAnna and The KingBianca Watanabe - RatillaPas encore d'évaluation
- EE114-1 Homework 2: Building Electrical SystemsDocument2 pagesEE114-1 Homework 2: Building Electrical SystemsGuiaSanchezPas encore d'évaluation
- Fabm2 q2 Module 4 TaxationDocument17 pagesFabm2 q2 Module 4 TaxationLady HaraPas encore d'évaluation
- Machine Tools Cutting FluidsDocument133 pagesMachine Tools Cutting FluidsDamodara MadhukarPas encore d'évaluation
- Impression Techniques in Complete Denture Patients: A ReviewDocument6 pagesImpression Techniques in Complete Denture Patients: A ReviewRoja AllampallyPas encore d'évaluation
- Irc SP 65-2005 PDFDocument32 pagesIrc SP 65-2005 PDFAjay Kumar JainPas encore d'évaluation
- Skype Sex - Date of Birth - Nationality: Curriculum VitaeDocument4 pagesSkype Sex - Date of Birth - Nationality: Curriculum VitaeSasa DjurasPas encore d'évaluation
- 37 Operational Emergency and Abnormal ProceduresDocument40 pages37 Operational Emergency and Abnormal ProceduresLucian Florin ZamfirPas encore d'évaluation
- 1 s2.0 S0959652619316804 MainDocument11 pages1 s2.0 S0959652619316804 MainEmma RouyrePas encore d'évaluation
- Product Data: T T 13 SEER Single - Packaged Heat Pump R (R - 410A) RefrigerantDocument36 pagesProduct Data: T T 13 SEER Single - Packaged Heat Pump R (R - 410A) RefrigerantJesus CantuPas encore d'évaluation
- Wei Et Al 2016Document7 pagesWei Et Al 2016Aline HunoPas encore d'évaluation
- 2019 BioscienceJDocument14 pages2019 BioscienceJPatrícia Lima D'AbadiaPas encore d'évaluation
- Textile Finishing Different Types of Mechanical Finishes For TextilesDocument3 pagesTextile Finishing Different Types of Mechanical Finishes For TextilesMohammed Atiqul Hoque ChowdhuryPas encore d'évaluation
- An Improved Ant Colony Algorithm and Its ApplicatiDocument10 pagesAn Improved Ant Colony Algorithm and Its ApplicatiI n T e R e Y ePas encore d'évaluation
- List of DEA SoftwareDocument12 pagesList of DEA SoftwareRohit MishraPas encore d'évaluation
- Differentiation: Vehicle Network SolutionsDocument1 pageDifferentiation: Vehicle Network SolutionsДрагиша Небитни ТрифуновићPas encore d'évaluation
- Service: Audi A6 1998Document256 pagesService: Audi A6 1998Kovács EndrePas encore d'évaluation
- Ericsson 3G Chapter 5 (Service Integrity) - WCDMA RAN OptDocument61 pagesEricsson 3G Chapter 5 (Service Integrity) - WCDMA RAN OptMehmet Can KahramanPas encore d'évaluation
- Network Theory - BASICS - : By: Mr. Vinod SalunkheDocument17 pagesNetwork Theory - BASICS - : By: Mr. Vinod Salunkhevinod SALUNKHEPas encore d'évaluation
- VISCOSITY CLASSIFICATION GUIDE FOR INDUSTRIAL LUBRICANTSDocument8 pagesVISCOSITY CLASSIFICATION GUIDE FOR INDUSTRIAL LUBRICANTSFrancisco TipanPas encore d'évaluation
- Cats - CopioniDocument64 pagesCats - CopioniINES ALIPRANDIPas encore d'évaluation
- O-L English - Model Paper - Colombo ZoneDocument6 pagesO-L English - Model Paper - Colombo ZoneJAYANI JAYAWARDHANA100% (4)
- Audi A3 Quick Reference Guide: Adjusting Front SeatsDocument4 pagesAudi A3 Quick Reference Guide: Adjusting Front SeatsgordonjairoPas encore d'évaluation
- FRABA - Absolute - Encoder / PLC - 1 (CPU 314C-2 PN/DP) / Program BlocksDocument3 pagesFRABA - Absolute - Encoder / PLC - 1 (CPU 314C-2 PN/DP) / Program BlocksAhmed YacoubPas encore d'évaluation
- 2.5L ENGINE Chevy Tracker 1999Document580 pages2.5L ENGINE Chevy Tracker 1999andres german romeroPas encore d'évaluation
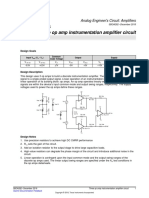
- Opamp TIDocument5 pagesOpamp TIAmogh Gajaré100% (1)
- MP & MC Module-4Document72 pagesMP & MC Module-4jeezPas encore d'évaluation
- Checklist For Mold RemediationDocument2 pagesChecklist For Mold Remediation631052Pas encore d'évaluation
- Rivalry and Central PlanningDocument109 pagesRivalry and Central PlanningElias GarciaPas encore d'évaluation
- Chapter 1Document2 pagesChapter 1Nor-man KusainPas encore d'évaluation
- Pic Attack1Document13 pagesPic Attack1celiaescaPas encore d'évaluation