Académique Documents
Professionnel Documents
Culture Documents
Aproximacion Eyaculación Precoz
Transféré par
Diana Pardo ReyDescription originale:
Titre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Aproximacion Eyaculación Precoz
Transféré par
Diana Pardo ReyDroits d'auteur :
Formats disponibles
0022-5347/02/1686-2359/0 THE JOURNAL OF UROLOGY Copyright 2002 by AMERICAN UROLOGICAL ASSOCIATION, INC.
DOI: 10.1097/01.ju.0000035599.35887.8f
Vol. 168, 2359 2367, December 2002 Printed in U.S.A.
Review Article
THE NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
MARCEL D. WALDINGER
From the Department of Psychiatry and Neurosexology, Leyenburg Hospital, The Hague and Department of Psychopharmacology, Rudolf Magnus Institute for Neurosciences, Faculty of Pharmaceutical Sciences, Utrecht University, Utrecht, The Netherlands
ABSTRACT
Purpose: Data showing the neurobiological background of rapid ejaculation was reviewed. In addition, new hypotheses to integrate clinical symptomatology, psychopharmacotherapy and psychotherapy of rapid ejaculation with brain function are provided. Materials and Methods: A computerized MEDLINE search, and manual bibliographic review of cross-references and neurobiological animal studies were performed. These reports were analyzed, summarized and compared with the studies performed by the author. Results: The literature on premature ejaculation published between 1887 and 2001 was reviewed. It appeared that the various psychological hypotheses and psychotherapies have not adequately been investigated. In contrast, psychopharmacological treatment studies, animal research data and stopwatch assessments in men with rapid (premature) ejaculation indicate that lifelong rapid ejaculation is a neurobiological phenomenon related to central serotonergic neurotransmission and likely influenced by hereditary factors. Conclusions: Basic and clinical psychopharmacological studies suggest that premature ejaculation is a not a psychological disturbance but a neurobiological phenomenon.
KEY WORDS: penis, ejaculation, serotonin, serotonin uptake inhibitors, sex disorders
Since the 1990s various psychopharmacological studies have shown that serotonergic antidepressants may effectively delay ejaculation in men with lifelong premature ejaculation. These results and animal data make it likely that premature ejaculation is not a psychological disorder but a neurobiological phenomenon. The consequences for understanding premature ejaculation and its treatment are discussed.
HISTORY
We can distinguish 4 periods in the course of the last century1 and 2 partly contrasting approaches, namely a somatic (urological or physiological) and a psychological (psychoanalytic or behavioristic) approach.2 The current era is that of the neurobiological approach, characterized by evidenced based animal and human psychopharmacological research, and antidepressant treatment as the first choice with psychotherapy only in cases of serious coping problems.1
CHRONOLOGICAL CLASSIFICATION
The first period (1887 to 1917): rapid ejaculation. In 1887 Gross described what was presumably the first case of rapid ejaculation in the medical literature.3 In 1901 a report of von Krafft-Ebing followed that referred to abnormally rapid ejaculation but did not yet use the word praecox or premature.4 The second period (1917 to 1950): neurosis and psychosomatic disorder. In 1917 Abraham described the syndrome of rapid ejaculation, which he called ejaculatio praecox.5 During the early decades of the 20th century premature ejaculation was viewed as a neurosis related to unconscious conflicts, especially in psychoanalytic theory.5, 6 Treatment consisted of classic psychoanalysis. The somatic approach was primarily urological, which focused on local anatomical causes, such
as hyperesthesia of the glans penis or a foreskin frenulum that was too short, and on changes in the posterior section of the urethra, particularly at the verumontanum. Advocated treatment included prescription of an anesthetizing ointment to incision of the frenulum or total destruction of the verumontanum by electrocautery. In 1943 Schapiro argued that premature ejaculation is a psychosomatic disturbance caused by the combination of a psychologically overanxious constitution and an inferior ejaculatory apparatus as a point of least resistance for emotional pressure.7 Schapiro described 2 types of premature ejaculation, namely type B, representing a continuously present tendency to ejaculate rapidly from the first act of intercourse, and type A, which led to erectile dysfunction. Many years later the 2 types became distinguished as the primary (lifelong) and secondary (acquired) forms of premature ejaculation, respectively.8 The third period (1950 to 1990): learned behavior. In the third period premature ejaculation was considered to be learned behavior. Rapid ejaculation associated with initial rapid intercourse led to habituation and created performance anxiety. Support for this behavioristic view was sought in physiological experiments, in which the phenomenon of anxiety was emphasized. Although behavioral therapy was still predominantly present in the literature, increasingly more publications focused on psychoactive drugs as a treatment. The third period (1990 to present): neurobiology and genetics. The introduction of clomipramine and selective serotonin re-uptake inhibitors (SSRIs) meant a dramatic change in treatment for premature ejaculation. The efficacy of these drugs in delaying ejaculation combined with the low side effect profile made them first choice agents for premature ejaculation on a daily as well as an on-demand basis.9 At the same time animal and sexual psychopharmacological human
2359
2360
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
studies10 attributed a serotonergic genesis1113 and possible genetic etiology14 to the neurobiological view of premature ejaculation.
CLASSIFICATION ACCORDING TO THE PSYCHOLOGICAL OR MEDICAL APPROACH
The psychological approach. According to the classic psychological view premature ejaculation is considered a psychosexual disorder with a psychogenic etiology and pathogenesis that must be treated with psychotherapy.15 Initially unconscious conflicts toward women were considered the core issue. However, since the article of Semans about the stopstart method,16 and particularly that of Masters and Johnson about the squeeze technique17 the pathogenesis was believed to be learned because initial intercourse was assumed to have been achieved hurriedly. In the psychological approach pathogenetic biological mechanisms remained unclear. Although a rapid ejaculation reflex was mentioned there was no information on the location of the neuronal circuitry of that particular reflex.16 Also, increased sensitivity of the glans penis was suggested. However, penile vibratory studies provided conflicting data on primary pathogenetic penile hypersensitivity.18 20 Not only the squeeze technique, but also all sorts of psychotherapy, including thought stopping,21, 22 Gestalt therapy,23 transactional analysis,24 group therapy25, 26 and bibliotherapy,27 have been suggested as treatment. Unfortunately the effectiveness of these therapies was only suggested in case reports but was never investigated in well designed controlled studies. However, of all of these treatments the squeeze method is said to give rise to short-term effectiveness. In 2 studies that were not well designed its initial effectiveness was confirmed but they also showed that the ejaculatory control initially attained was virtually lost after a 3-year followup.28, 29 Definition of Premature Ejaculation: In the psychological approach consensus on a definition of premature ejaculation has never been reached due to conflicting ideas on the essence of the syndrome. Masters and Johnson,17 and Kaplan30 suggested qualitative descriptions, for example female partner satisfaction or male voluntary control. Masters and Johnson defined premature ejaculation as male inability to inhibit ejaculation long enough for the partner to reach orgasm in 50% of intercourse episodes.17 It is important to realize that based on their definition they claimed that the squeeze method was highly effective treatment. However, it is obvious that their definition in terms of partner response is inadequate because it implies that any male partner of females who has difficulty in reaching orgasm could be labeled a premature ejaculator and also females should achieve orgasm on 50% of intercourse episodes. Another way to define premature ejaculation is by quantitative measures such as the duration of ejaculatory latency or the number of thrusts before ejaculation. Definitions according to the time before ejaculation varied from 1 to 7 minutes after vaginal intromission.31 40 These cutoff points (1 to 7 minutes) were not derived by objective measurements but were subjectively chosen by the various investigators. Premature ejaculation was a matter of many minutes and cases of ejaculation within seconds were considered serious. Equally subjective cutoff points were proposed for the number of thrusts as a criterion for premature ejaculation, namely ejaculation within 8 to 15 thrusts.41 43 Methodology of Psychological Studies: During the many years in which the psychological approach prevailed, the proposed psychological hypotheses and psychotherapeutic treatments were not proved in any proper scientific study.12, 44 For example, Masters and Johnson argued that premature ejaculation was conditioned by experiencing first sexual intercourse in a rapid way, such as by hurried con-
tacts in the back seats of a car or in places where detection was possible and by consequent performance anxiety.45 However, evidenced based data for this assumption has never been reported. Briefly, until today no evidenced based psychological study has been available in the literature. Therefore, scientific knowledge about the fundamentals of the psychological approach remain to be elucidated. It is rather peculiar that despite some available studies of the poor response of psychological treatment and insufficient study methodology37, 46 50 the principles of the psychological approach have never been altered and subsequently tested. The methodological insufficiencies are serious. For example, no objective and accurate measures or clear definitions of ejaculation time, the number of thrusts or satisfaction have been used. Men were only asked about ejaculation latency without any quantifying method. Furthermore, retrospective information was used instead of prospective baseline measurements of each coitus. Behavioral treatments were compared neither with nonbehavioral treatment nor with random nonsense psychological treatment. Moreover, assessments were only made in men, whereas information from females about partner ejaculation time was completely neglected. The medical approach. Pharmacotherapy: Since the 1940s, case reports have occasionally been published about various drugs with efficacy for delaying ejaculation. Physicians attempted to decrease penile sensation and delay ejaculation by applying local anesthetics to the glans penis.7, 5154 Others tried to influence the peripheral sympathetic nervous system by prescribing sympatholytic drugs, such as the 1 and 2adrenergic blocker phenoxybenzamine5557 or the selective 1-adrenergic blockers alfuzosin and terazosin.58 In the 1960s case reports described the ejaculation delaying effects of some neuroleptics. Thioridazine59 62 and chlorprothixene63 delayed ejaculation by blocking central dopamine receptors. In the same period case reports of the delaying effects of nonselective, irreversible monoamine oxidase inhibitors, for example isocarboxazid64 and phenelzine,65 were published. However, the use of these various drugs was often contraindicated by their disturbing and sometimes quite serious side effects. In 1973 Eaton reported the first study of clomipramine as effective treatment for premature ejaculation.49 Later case reports and double-blind studies43, 6674 repeatedly demonstrated the effectiveness of clomipramine at low daily doses for delaying ejaculation. In 1993 Segraves et al reported the first double-blind placebo controlled study showing that 25 to 50 mg. clomipramine can even be ingested on an on-demand basis approximately 6 hours before coitus.43 On-demand treatment was replicated in later studies.73 Unfortunately similar to psychological studies, the majority of these initial pharmacological studies were designed without a precise definition of premature ejaculation and with a poor methodology for quantifying the effects of treatment. The efficacy of clomipramine was recognized by some sexologists but never reached an international consensus.75 SSRIs: In 1994 Waldinger et al reported the first placebo controlled study of 40 mg. paroxetine daily for successfully treating premature ejaculation.76 The efficacy of paroxetine at daily doses of 20 to 40 mg. was replicated in independent studies at a regular daily dose77 82 and in an on-demand regimen.83 In addition, the efficacy of other SSR inhibitors, such as 50 to 200 mg. sertraline daily74, 78, 79, 84 86 and 20 mg. fluoxetine daily,78, 87 89 has been reported for delaying ejaculation. There have only been 2 parallel group doseresponse studies. Clomipramine at 25 and 50 mg. daily,71 and paroxetine at 20 and 40 mg. daily77 showed a trend, although it was not statistically significant, toward further ejaculation delay when the dose was doubled. In contrast to the insufficient methodology in psychological studies and initial psychopharmacological studies, the well
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
2361
described methodology of psychopharmacological studies in recent years is underlined. In last decade major methodological improvements were developed. For example, in 1994 Waldinger et al operationally defined premature ejaculation and introduced the intravaginal ejaculation latency time parameter, defined as the time between the start of intravaginal intromission and the start of intravaginal ejaculation, as an operational measure of ejaculation time.76 In the same study we also used the medical interview of the female partner as a comparative means for spouse estimation of ejaculation time. The stopwatch, which was originally introduced in 1973 as an accurate tool to measure ejaculation time,90 was prudently reintroduced in 1995 by Althof et al.72 In 1998 we introduced the baseline measurement of intravaginal ejaculation latency time at each intercourse in a standard period of 4 weeks with a stopwatch handled by the female partner.78 Differential Efficacy of SSRIs for Delaying Ejaculation: Using intravaginal ejaculation latency time, a stopwatch and 4-week baseline assessment at each intercourse comparative placebo controlled studies showed a difference for delaying ejaculation in various SSRIs at equivalent doses. It was noted that 20 mg. paroxetine daily and 20 mg. fluoxetine daily resulted in strong delays, 50 mg. sertraline daily resulted in moderate delay but 100 mg. fluvoxamine daily and 20 mg. citalopram daily caused only mild to moderate delay. The mild delay of fluvoxamine compared with paroxetine was replicated in a placebo controlled male rat study using a chronic administration treatment model,91 whereas after acute treatment such a significant difference was not observed.92 Because explanations in terms of transporter occupancy, pharmacokinetics, metabolism or active metabolites could be discarded, no adequate explanation can yet be offered to explain these differential actions. However, it was speculated that each SSRI enhances the amount of serotonin, that is 5-hydroxytryptamine (5-HT), differentially and each SSRI may also act differentially at different places in the central nervous system, thereby, stimulating postsynaptic 5-HT receptors differentially.11, 12, 93 Moreover, the different modes of action of SSRIs should further be explained by the evaluation of other mechanisms that are potentially involved in the mechanism of ejaculation. A likely candidate could be the neuropeptide oxytocin, which has shown to be involved in human orgasm.81 In a recent animal study the ejaculation delay induced by fluoxetine was reversed by the administration of oxytocin.94 This finding suggests that fluoxetine induced delayed ejaculation is related to inhibited oxytocin release. In another study it was observed that oxytocinergic neurons contain serotonergic receptors.95 In addition, in male and female human orgasms oxytocin is released just before and during orgasm.96, 97 Therefore, we suggest that the differential effects of SSR inhibitors and other antidepressants on ejaculation may be related to postsynaptic 5-HT receptors, which have differential influence on central oxytocinergic neurons intimately involved in the ejaculation process.81 Further studies are needed to investigate the presumed and intriguing role of oxytocin in antidepressant induced delayed ejaculation.
ANIMAL STUDIES
nists it became evident that the role of 5-HT2C receptors in ejaculation seems rather crucial. In addition to 5-HT2C receptors, a second subclass of 5-HT2 receptors, that is 5-HT2A receptors, has also been investigated but until now its role in ejaculation has not been identified.79 For example, in regard to the 5-HT2C receptor male rat studies with d-lysergic acid diethylamide and quipazine, which are nonselective 5-HT2C agonists, suggest that stimulating 5-HT2C receptors delays ejaculation.98 However, 2,5-dimethoxy-4-iodophenyl-2aminopropane, which equally stimulates 5-HT2A and 5-HT2C receptors, also increases ejaculation latency,99 whereas the selective 5-HT2A receptor agonist 2,5-dimethoxy-4-methylamphetamine does not have this effect.98 Male rat studies have also shown the involvement of another serotonin subtype receptor, namely the 5-HT1A receptor, in the ejaculation process. Activation of postsynaptic 5-HT1A receptors by the selective 5-HT1A receptor agonist 8-hydroxy-2-(di-n-propylaminotetralin) in male rats resulted in shorter ejaculation latency.98 Based on 5-HT2C and 5-HT1A receptor interaction data in animals Waldinger et al formulated the hypothesis that in premature ejaculation in humans there is hyposensitivity of the 5-HT2C and/or hypersensitivity of the 5-HT1A receptor.100 The hypothesis that activation of postsynaptic 5-HT receptors delays ejaculation was supported by 4 stopwatch studies in humans with different SSRIs.78 81 However, in these studies it was not obvious whether similar receptor subtypes, that is 5-HT2C and 5-HT1A receptors, are also involved in human ejaculation since SSRI treatment activates many different postsynaptic subtype receptors.11 To find an answer 2 human studies with the 5-HT2C blocking antidepressants nefazodone and mirtazapine were performed.79, 81 In a comparative double-blind placebo controlled study with the 5HT2C/5-HT2A receptor antagonist and 400 mg. daily of the 5-HT/noradrenaline re-uptake inhibitor nefazodone, nefazodone and placebo did not exert any ejaculation delay in contrast to a significant delay after 20 mg. paroxetine daily and 50 mg. sertraline daily.79 In a similar study the 5-HT2C/5-HT3 receptor antagonist, and noradrenergic and specific serotonergic antidepressant mirtazapine did not induce ejaculation delay compared with the significant delay resulting from 20 mg. paroxetine daily.81 It should be emphasized that in these studies in men with premature ejaculation neither antidepressant delayed ejaculation, while for 5-HT2C antagonism shorter ejaculation latency was expected. Therefore, further research is encouraged to elucidate still undiscovered pharmacological mechanisms underlying the ejaculatory process. Since to our knowledge the role of 5-HT2A and 5-HT3 receptors in ejaculation has not yet been identified in male rats or humans, the lack of ejaculation delay associated with these 5-HT2C receptor blocking drugs suggests that the 5-HT2C receptor is specifically involved in human ejaculation and indirectly supports our hypothesis of 5-HT2C receptor hypofunction in men with premature ejaculation. However, the exact identification of the specific 5-HT receptor subtypes involved in premature ejaculation is only possible by administering subtype selective 5-HT2C or 5-HT1A receptor ligands. Unfortunately these agents are not yet available for human use.
NEUROANATOMY
In contrast to the prevailing psychological approach to premature ejaculation, neuroscientists were already investigating the role of central serotonin and dopamine neurotransmission in ejaculation in the 1970s. However, the intriguing findings of basic neurosciences were hardly integrated with clinical practice in those years. What we have learned to date in animal studies is that serotonin 5-HT receptors are involved in the ejaculatory process. In addition, using highly selective 5-HT receptor agonists and antago-
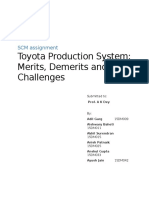
Most knowledge of the functional neuroanatomy of ejaculation is derived from male rat studies. In regard to male rat copulatory behavior one must distinguish among the brain, brainstem and spinal cord regions that become activated before and after ejaculation, when sensory information returns from the genitals (fig. 1). The medial preoptic area in the rostral hypothalamus and nucleus paragigantocellularis in the ventral medulla101, 102 are suggested to have impor-
2362
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
FIG. 1. Central nervous system areas involved before, during and after ejaculation. Somatosensory fibers reach sensory cortex. Efferent pathways run from hypothalamus down to sacral spinal cord and genitals. After ejaculation information is returned from genitals to various areas in cerebrum. MEApd, posterodorsal medial amygdala. BNSTpm, posteromedial bed nucleus of stria terminalis. MPOA, medial preoptic area. SPFp, medial parvicellular subparafascicular nucleus of thalamus. nPGi, nucleus paragigantocellularis.
tant roles in the process leading toward ejaculation. Electrical stimulation of the medial preoptic area promotes ejaculation.103 It is hypothesized that ejaculation is tonically inhibited by serotonergic pathways descending from the nucleus paragigantocellularis to the lumbosacral motor nuclei. The current hypothesis is that the nucleus paragigantocellularis is inhibited by inhibitory stimuli from the medial preoptic area. Disinhibition of the nucleus paragigantocellularis is supposed to lead to ejaculation. The discovery of serotonergic neurons in the nucleus paragigantocellularis and the well-known ejaculation delay induced by serotonergic antidepressants suggests an action of the SSRIs inhibitors on the nucleus paragigantocellularis. However, to our knowledge the precise location in the central nervous system on which SSRIs inhibitors act to inhibit ejaculation has yet not been identified. On the other hand, brain areas activated as a result of 1 or more ejaculations have been observed in several mammals.104 Using expression of the immediate early gene c-fos as a marker for neural activity in male rats Coolen et al detected distinct ejaculation related neural activation in several brain regions after ejaculation, namely the posteromedial bed nucleus of the stria terminalis, a lateral subarea of the posterodorsal medial amygdala, and the medial parvicellular subparafascicular nucleus of the thalamus.105107 All available evidence suggests that ascending fibers from the spinal cord, which signal ejaculation, activate the medial parvicellular subparafascicular nucleus and the other brain areas mentioned. Since it has been shown that this cluster of activated neurons are extensively interconnected, mostly reciprocally,107 a complete brain circuit related to ejaculation seems to be involved. The functional significance of this ejaculation subcircuit is still poorly understood but it may well be that these areas have a role in satiety and, thus, in mediating the post-ejaculatory interval. These and many other animal studies have clearly shown the existence of a neural circuitry for ejaculation in mammals. This neural circuitry is partly elucidated but still
poorly understood. Interestingly a neurophysiological study showed shorter latencies and greater amplitudes of somatosensory evoked potentials from the glans penis in men with lifelong premature ejaculation compared with matched normal controls.108 This series and those of sacral evoked potential41, 42, 109 suggest that men with premature ejaculation have greater cortical representation of sensory stimuli from the glans penis than normal controls. However, such a larger somatosensory cortical representation has not yet been identified. Brain imaging, for example positron emission tomography, is required in humans to unravel the neural substrate, particularly the cortical substrate, of the ejaculatory process in men. Imaging may contribute to better understanding of which part of the circuitry is disturbed in premature ejaculation.
EMPIRICAL OPERATIONAL DEFINITION OF PREMATURE EJACULATION
The American Psychiatric Association defines premature ejaculation as persistent or recurrent ejaculation with minimal sexual stimulation before, upon, or shortly after penetration and before the person wishes it.110 Until recently any scientific basis for the DSM-IV definition was lacking. For instance, the meaning of persistent, recurrent, minimal and shortly after is vague and certainly needs further qualification. Therefore, our group introduced a stopwatch method to determine an empirically operational definition in a study including 110 consecutively enrolled men with lifelong premature ejaculation.111 In this study the visibility of stopwatch assessments by female partners as well as the outcome was studied after instructing the couples to use a stopwatch at home during each coitus for 4 weeks (fig. 2). This method was accepted and well performed by all couples included in this study. Of these men 90% ejaculated within 1 minute of intromission, including 80% who ejaculated within 30 seconds. The age of the men and duration of the relationship were not correlated with ejaculation time. According to
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
2363
these data we have shown that ejaculation time can be monitored with a stopwatch. In cases of premature ejaculation it empirically appeared that ejaculation time was less than 1 minute in more than 90% of episodes of sexual intercourse independent of age and the duration of relationship in those men who complained of lifelong premature ejaculation. Thus, assessment by stopwatch revealed that premature ejaculation is a matter of seconds and not minutes.2, 111 To our knowledge that study is the first stopwatch study in a white Western European cohort. From a clinical point of view other patient populations with complaints of rapid ejaculation should be investigated in regard to cultural differences and associated behavior. For example, do men in other countries or cultures consider that they ejaculate prematurely when they ejaculate within 4 minutes?
PREVALENCE
relatives about ejaculation latency. These 14 men reported a total of 11 first degree male relatives with information available for direct personal interview. In fact, 10 relatives fulfilled our strict defined criterion of an ejaculation time of 1 minute or less. In this small select group of men the calculated risk of having a first relative with premature ejaculation was 91% (CI 59 to 99). Therefore, the odds of family occurrence is much higher than the suggested population prevalence rate of 4% to 39%. Moreover, the high odds ratio indicates a familiar occurrence of the syndrome far higher than of chance alone. Based on this preliminary observation the influence of genetics formerly noted by Schapiro7 gains substantial credibility.
BIOLOGICAL VARIATION OF EJACULATION LATENCY TIME
Premature ejaculation is said to be the most frequent male sexual disorder.15 The prevalence in the general population is estimated to be 4% to 39%.112116 These prevalence studies applied various frequently nonvalidated definitions and methodologies of premature ejaculation. However, it should be emphasized that normative data on ejaculation latency time obtained by the stopwatch method in the general male population are mandatory to really establish the prevalence of lifelong premature ejaculation, defined as an ejaculation time of less than 1 minute in men with complaints of rapid ejaculation. Obviously an accurate definition of premature ejaculation is necessary not only for clinical diagnosis and treatment, but also for comparing data from different studies117 and performing epidemiological studies.
FAMILIAL OCCURRENCE OF PREMATURE EJACULATION
In 1943 Schapiro noted that men with premature ejaculation seemed to have family members with similar complaints.7 Remarkably to our knowledge this interesting observation has never been cited. To investigate the potential familial occurrence of premature ejaculation we routinely asked 237 consecutively enrolled men with premature ejaculation about the family occurrence of similar complaints.14 Due to embarrassment only 14 men consented to ask male
According to the classic psychological view premature ejaculation has always been considered a behavioral aberration, that is a specific disorder caused by psychological factors with the potential for cure. However, there is no scientific evidence to support this view. On the other hand, the development of objective ejaculation time assessment methods (intravaginal ejaculation latency time and stopwatch)76 81 and pharmacological knowledge about the action of effective drugs are the cornerstones of an upcoming neurobiological approach.12 Recently Waldinger et al postulated the biological variability of intravaginal ejaculation latency time in men, ranging from extremely rapid through normal or average to slow ejaculation.12, 93 However, due to a lack of epidemiological (stopwatch) research the distribution of the mean and range values of normal ejaculation latency time in the whole male human population is not yet known.12 The assumption of population based variability of ejaculation time implies that rapid ejaculation should be considered a biological phenomenon rather than a behavioral aberration. This biological phenomenon is most probably differently appreciated among individuals, populations and cultures. There are men and women who cope well with rapid ejaculation and do not consider it a major problem. However, in other men and their sexual partners rapid ejaculation may become a psychological or emotional problem. This problem may become so severe that psychotherapeutic intervention
FIG. 2. Intravaginal ejaculation latency time (IELT) measured with stopwatch in 110 men with lifelong premature ejaculation, of whom 90% ejaculated within 1 minute after vaginal penetration, including 80% within 30 seconds. Reprinted with permission.111
2364
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
may become beneficial to support the man or couple in coping with premature ejaculation. Therefore, psychology is a secondary problem rather than the primary cause of premature ejaculation.
EJACULATION THRESHOLD HYPOTHESIS
To understand the suggested biological variation of intravaginal ejaculation latency time in relation to the serotonergic system, delaying effects of SSRIs and suggested genetics Waldinger and Olivier have proposed the existence of an intravaginal ejaculation latency time threshold.12 When there is a low threshold set point men can only sustain low sexual arousal before ejaculation. Whatever these men do or fantasize during intercourse any control of ejaculation remains marginal and they ejaculate easily even when they are not fully aroused. The assumption that men with premature ejaculation ejaculate at lower levels of sexual arousal was demonstrated by Spiess et al in a study comparing 10 men with premature ejaculation (ejaculation at less than 2 minutes) and 14 controls (ejaculation at more than 3 minutes) by physiological (penis circumference) and self-report measures of sexual arousal.32 The low threshold is assumed to be associated with low 5-HT neurotransmission and probably hypofunction of the 5-HT2C receptor, as mentioned. When there is a higher set point men experience more control over ejaculation time. They can sustain more sexual arousal before ejaculating. In these men 5-HT neurotransmission varies around a normal or average level and 5-HT2C receptor functions normally. To our knowledge the mean and range values of the set points considered normal or average are not known. When there is a high or very high set point, men may experience difficulty in ejaculating or cannot achieve ejaculation even when fully aroused sexually. At a high set point 5-HT neurotransmission is supposed to be increased and/or 5-HT2C receptor sensitivity is enhanced. According to this threshold hypothesis it appears that the level of 5-HT2C receptor activation determines the set point and associated ejaculation latency time in an individual. In men with premature ejaculation or any man on serotonergic antidepressants SSRIs and clomipramine activate 5-HT2C receptor and, therefore, change the set point to a higher level, leading to a delay in ejaculation. The effects of SSRIs on the set point appear to be individually determined since some men respond with an intense delay, while others only experience slight delay at the same dose of the drug. Moreover, cessation of treatment results in uniform resetting of the set point within 3 to 5 days to the lower, individually determined reference level, which is assumed to be genetically determined. It is speculated that the threshold is mediated by serotonin neurotransmission and 5-HT receptors in the brainstem93 or spinal cord and may consist of serotonergic fibers that inhibit neurons that convey somatosensory information from the genitals. It is suggested that SSRIs enhance the inhibitory effects of these serotonergic neurons. However, the cerebral cortex may also mediate inhibitory impulses but currently this finding has not been reported. In addition to the suggested SSRI induced increased inhibition of sensory input, SSRIs may also delay ejaculation by interfering with spinal cord motoneurons of peripheral neurons that inhibit the internal genitals. Further studies are needed to unravel this important and intriguing question.
COURSE OF RAPIDITY
throughout their lifetime the speed of ejaculation had remained as rapid as at the first sexual contacts in puberty and adolescence, 23% reported that it had even become gradually more rapid with aging and only 1% reported that it had become slower.111 According to these data it is questionable whether the fixed rapidity and even paradoxical shortening of ejaculation latency time with aging should be considered part of the pathogenetic process of premature ejaculation. We think of the phenomenon of rapid ejaculation as a biological variation and its paradoxical or fixed course through life as pathological. Chronic premature ejaculation appears to be the clinical syndrome of primary (lifelong) premature ejaculation. To date there is no real cure for lifelong premature ejaculation. Drugs may alleviate symptoms but only while they are being administered.
PREMATURE EJACULATION AND ERECTILE DYSFUNCTION
It is generally believed that aging delays ejaculation. This assumption may be true in men with a normal or average ejaculation time but to our knowledge it has never been investigated in men with premature ejaculation. In a stopwatch study of 110 consecutively enrolled men 18 to 65 years old with lifelong premature ejaculation 76% reported that
Some men with premature ejaculation may express their complaint as an erectile disorder since penile detumescence after ejaculation occurs rapidly. On the other hand, erectile dysfunction may be superimposed on lifelong existing premature ejaculation due to the efforts of these men to minimize sexual excitement or to general causes of erectile dysfunction. One may wonder whether premature ejaculation is associated with an increased neurobiological risk for erectile dysfunction. To our knowledge there is no evidence for such an associated risk to date. To study such risk longitudinal prospective studies in men with premature ejaculation and matched controls are necessary but they have not yet been performed. It must be emphasized that the majority of men with lifelong premature ejaculation do not suffer from concomitant erectile difficulties. Most of these men do not seek help due to rapid ejaculation. However, since some men start to seek help after they have erectile difficulties, it may bias the population with premature ejaculation that presents to a urology clinic. In our studies we recruited men with premature ejaculation by advertisement. Of the respondents 75% had never sought help for premature ejaculation, mostly due to embarrassment, and 95% did not have erectile difficulties.111 In contrast, many of these men reported rapid achievement of erection. In 1943 Schapiro called this phenomenon erectio praecox7 but this term has never been quoted or referred to in the literature. It may be speculated that aside from its relationship to the central serotonergic system premature ejaculation is also related to increased oxytocin production. A speculated increase in oxytocin release may be related to ejaculatio praecox with erectio praecox. Animal studies show that oxytocin stimulates ejaculation118, 119 and is a potent inducer of penile erection.120 SSRIs are well known for delaying ejaculation and to a lesser extent for inducing erectile difficulties and the loss of sexual desire. The precise mechanism by which SSRIs interfere with erectile function is not clear. The various SSRI treatment studies of premature ejaculation are characterized by a low incidence of erectile difficulties. However, in clinical practice SSRI treatment may give rise to complaints of slightly decreased rigidity of the erect penis. The proved effectiveness of SSRIs for serotonergic related disorders, such as depression, anxiety disorders, obsessivecompulsive disorder and increased impulsivity, may raise the question whether men with premature ejaculation are at risk for these disorders. Our studies using a clinical interview and the Symptom Check List with 90 items have repeatedly and clearly indicated that men with lifelong premature ejaculation are generally mentally and physically healthy, as healthy as the average individual in the age matched general nonpsychiatric male population.
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION
BEHAVIORAL THERAPY AND THE NEUROBIOLOGICAL APPROACH
2365
Controversy over the most appropriate therapeutic approach is nourished by the confusing use of surrogate and clinically relevant end points when interpreting treatment results. For example, surrogate end points such as thrusting with multiple stops must be distinguished from clinically relevant ongoing successful thrusting. In contrast to the beneficial clinical effects of pharmacotherapy, clinical effects as a result of behavioral therapy still lack well designed investigation. Further behavioral studies of the squeeze technique with baseline and prospective stopwatch and intravaginal ejaculation latency time assessment are imperative. The first choice of treatment for premature ejaculation is psychopharmacotherapy. It should be underlined that couples should be briefly informed about current knowledge on the neurobiological approach to premature ejaculation. On the other hand, psychotherapy is only indicated in men or couples who cannot cope with or cannot accept rapid ejaculation.1 In contrast to the classic psychological view, the purpose of psychodynamic or cognitive psychotherapy is not to learn how to delay ejaculation, but rather how to cope with rapid ejaculation.1
CONCLUSIONS
Neurobiological research in the last decade has shown that the classic psychological view of lifelong premature ejaculation is no longer tenable. In contrast to the behavioristic view, the neurobiological approach has gained support because of clinical and preclinical based evidence. According to the latter view premature ejaculation should be considered part of normally distributed ejaculation latency time in the general male population independent of the natural course of aging induced ejaculation delay. Paradoxically ejaculation latency remains similar or even becomes more rapid with aging. Rapid ejaculation seems to be related to disturbed or maladaptive 5-HT2C receptor properties in specific brain areas that can be restored by serotonergic agents. Cognitive and emotional influences certainly interact with ejaculation but psychological disturbances must be considered a secondary reaction. Based on various methodologically well designed studies psychopharmacotherapy should be acknowledged as primary treatment.121 A brief education on the new neurobiological knowledge should accompany the prescription of drugs. Although paroxetine and clomipramine are highly efficacious for delaying ejaculation, further development of more rapidly acting drugs would certainly benefit modern patient care. Drs. Dave H. Schweitzer and Berend Olivier reviewed the manuscript.
REFERENCES
1. Waldinger, M. D.: Klaar is Kees: Een Nieuwe Visie op Vroegtijdige Zaadlozing. Amsterdam: Uitgeverij de Arbeiderspers, 1999 2. Waldinger, M. D.: When Seconds Count. Selective Serotonin Reuptake Inhibitors and Ejaculation. Thesis, Utrecht, The Netherlands, chapt. 1, p. 11, 1997 3. Gross, S.: Practical Treatise on Impotence and Sterility. Edinburgh: Y. J. Pentland, 1887 4. von Krafft-Ebing, R. F.: Psychopathia Sexualis, 11th ed. Stuttgart: Publishing Hause Enke, 1901 5. Abraham, K.: Ueber Ejaculatio Praecox. Zeitschr Aerztl Psychoanal, 4: 171, 1917 6. Stekel, W.: Impotence in the Male. New York: Liveright Publishing, vol. 2, 1927 7. Schapiro, B.: Premature ejaculation: a review of 1130 cases. J Urol, 50: 374, 1943 8. Godpodinoff, M. L.: Premature ejaculation: clinical subgroups and etiology. J Sex Marital Ther, 15: 130, 1989 9. Waldinger, M. D.: Use of psychoactive agents in the treatment of sexual dysfunction CNS Drugs, 6: 204, 1996
10. Waldinger, M. D. and Hengeveld, M. W.: Neuroseksuologie en seksuele psychofarmacologie. Tijdschr Psychiatr, 8: 585, 2000 11. Olivier, B., van Oorschot, R. and Waldinger, M. D.: Serotonin, serotonergic receptors, selective serotonin reuptake inhibitors and sexual behaviour. Int Clin Psychopharmacol, suppl., 13: s9, 1998 12. Waldinger, M. D. and Olivier, B.: Selective serotonin reuptake inhibitors (SSRIs) and sexual side effects: differences in delaying ejaculation. In: Fluvoxamine: Established and Emerging Roles in Psychiatric Disorders. Advances in Preclinical and Clinical Psychiatry. Edited by E. Sacchetti and P. Spano. Milan: Excerpta Medica, vol. 1, pp. 117130, 2000 13. Waldinger, M. D. and Olivier, B.: Hersenonderzoek en farmacologie: serotonine, seks en agressie. In: Het Brein Belicht: Opstellen over Niet-Aangeboren Hersenletsel. Edited by M. H. J. Wolters-Schweitzer and C. L. Beuger. Utrecht: Uitgeverij Lemma, pp. 55 63, 2001 14. Waldinger, M. D., Rietschel, M., Nothen, M. M., Hengeveld, M. W. and Olivier, B.: Familial occurrence of primary premature ejaculation. Psychiatr Genet, 8: 37, 1998 15. St. Lawrence, J. S. and Madakasira, S.: Evaluation and treatment of premature ejaculation: a critical review. Int J Psychiatr Med, 22: 77, 1992 16. Semans, J. H.: Premature ejaculation: new approach. South Med J, 49: 353, 1956 17. Masters, W. H., Johnson, V. E.: Human Sexual Inadequacy. Boston: Little, Brown & Co., 1970 18. Rowland, D. L., Haensel, S. M., Blom, J. H. M. and Slob, A. K.: Penile sensitivity in men with premature ejaculation and erectile dysfunction. J Sex Marital Ther, 19: 189, 1993 19. Xin, Z. C., Chung, W. S., Choi, Y. D., Seong, D. H., Choi, Y. J. and Choi, H. K.: Penile sensitivity in patients with primary premature ejaculation. J Urol, 156: 979, 1996 20. Paick, J. S., Jeong, H. and Park, M. S.: Penile sensitivity in men with premature ejaculation. Int J Impot Res, 10: 247, 1998 21. Ince, L.: Behavior modification of sexual disorders. Am J Psychother, 17: 446, 1973 22. Wish, P.: The use of imagery-based techniques in the treatment of sexual dysfunction. Couns Psychol, 5: 52, 1975 23. Mosher, D. L.: Awareness in Gestalt sex therapy. J Sex Marital Ther, 5: 41, 1979 24. Waltzlawick, P., Weakland, J. H. and Fisch, R.: Change: Principles of Problem Formation and Problem Resolution. New York: Norton Publishing, 1974 25. Zeiss, R. A., Christensen, A. and Levine, A. G.: Treatment for premature ejaculation through male-only groups. J Sex Marital Ther, 4: 139, 1978 26. Kaplan, H. S., Kohl, R. N., Pomeroy, W. B., Offit, A. K. and Hogan, B.: Group treatment of premature ejaculation. Arch Sex Behav, 3: 443, 1974 27. Lowe, C. J. and Mikulas, W. L.: Use of written material in learning self control of premature ejaculation. Psychol Rep, 37: 295, 1975 28. De Amicis, L. A., Goldberg, D. C., LoPiccolo, J., Friedman, J. and Davies, L.: Clinical follow-up of couples treated for sexual dysfunction. Arch Sex Behav, 14: 467, 1985 29. Hawton, K. and Catalan, J.: Prognostic factors in sex therapy. Behav Res Ther, 24: 377, 1986 30. Kaplan, H. S.: The New Sex Therapy: Active Treatment of Sexual Dysfunctions. New York: Brunner/Mazel, 1974 31. Cooper, A. J. and Magnus, R. V.: A clinical trial of the beta blocker propranolol in premature ejaculation. J Psychosom Res, 28: 331, 1984 32. Spiess, W. F., Geer, J. H. and ODonohue, W. T.: Premature ejaculation: investigation of factors in ejaculatory latency. J Abnorm Psychol, 93: 242, 1984 33. Strassberg, D. S., Mahoney, J. M., Schaugaard, M. and Hale, V. E.: The role of anxiety in premature ejaculation: a psychophysiological model. Arch Sex Behav, 19: 251, 1990 34. Obler, M.: Systematic desensitisation in sexual disorders. J Behav Ther Exp Psychiatr, 4: 93, 1973 35. Strassberg, D. S., Kelly, M. P., Carroll, C. and Kircher, J. C.: The psychophysiological nature of premature ejaculation. Arch Sex Behav, 16: 327, 1987 36. LoPiccolo, J.: Direct treatment of sexual dysfunction in the couple. In: Handbook of Sexology: Selected Syndromes and Therapy. Edited by J. Money and H. Musaph. New York:
2366
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION suppl., 8: 53, 1980 67. Porto, R.: Essai en double aveugle de la clomipramine dans le jaculation prematuree. Med Hygiene, 39: 1249, 1981 68. Girgis, S. M., El-Haggen, S. and El-Hermouzy, S.: A doubleblind trial of clomipramine in premature ejaculation. Andrologia, 14: 364, 1982 69. Klug, B.: Clomipramine in premature ejaculation. Med J Aust, 141: 71, 1984 70. Assalian, P.: Clomipramine in the treatment of premature ejaculation. J Sex Res, 24: 213, 1988 71. Althof, S. E.: Pharmacologic treatment of rapid ejaculation. Psychiatr Clin North Am, 18: 85, 1995 72. Althof, S. E., Levine, S. B., Corty, E. W., Risen, C. B., Stern, E. B. and Kurit, D. M.: A double-blind crossover trial of clomipramine for rapid ejaculation in 15 couples. J Clin Psychiatry, 56: 402, 1995 73. Haensel, S. M., Rowland, D. L., Kallan, K. T. H. K. and Slob, A. K.: Clomipramine and sexual function in men with premature ejaculation and controls. J Urol, 156: 1310, 1996 74. Kim, S. C. and Seo, K. K.: Efficacy and safety of fluoxetine, sertraline and clomipramine in patients with premature ejaculation: a double-blind, placebo controlled study. J Urol, 159: 425, 1998 75. Assalian, P.: Premature ejaculation: is it really psychogenic? J Sex Educ Ther, 20: 1, 1994 76. Waldinger, M. D., Hengeveld, M. W. and Zwinderman, A. H.: Paroxetine treatment of premature ejaculation: a doubleblind, randomized, placebo-controlled study. Am J Psychiatry, 151: 1377, 1994 77. Waldinger, M. D., Hengeveld, M. W. and Zwinderman, A. H.: Ejaculation-retarding properties of paroxetine in patients with primary premature ejaculation: a double- blind, randomized, dose-response study. Br J Urol, 79: 592, 1997 78. Waldinger, M. D., Hengeveld, M. W., Zwinderman, A. H. and Olivier, B.: Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine and sertraline. J Clin Psychopharmacol, 18: 274, 1998 79. Waldinger, M. D., Zwinderman, A. H. and Olivier, B.: Antidepressants and ejaculation: a double-blind, randomized, placebo-controlled, fixed-dose study with paroxetine, sertraline, and nefazodone. J Clin Psychopharmacol, 21: 293, 2001 80. Waldinger, M. D., Zwinderman, A. H. and Olivier, B.: SSRIs and ejaculation: a double-blind, randomized, fixed-dose study with paroxetine and citalopram. J Clin Psychopharmacol, 21: 556, 2001 81. Waldinger, M. D., Zwinderman, A. H. and Olivier, B.: Antidepressants and ejaculation: a double-blind, randomised, fixed-dose study with mirtazapine and paroxetine. In: New Research Program of 2001 Annual Meeting of American Psychiatric Association, New Orleans, Louisianna, May 5-10, nr. 715, p. 52, 2001 82. Ludovico, G. M., Corvace, A., Pagliarulo, G., Cirillo-Marucco, E. and Marano, A. and Pagliarulo, A.: Paroxetine in the treatment of premature ejaculation. Br J Urol, 77: 881, 1996 83. McMahon, C. G. and Touma, K.: Treatment of premature ejaculation with paroxetine hydrochloride as needed: 2 singleblind placebo controlled crossover studies. J Urol, 161: 1826, 1999 84. Mendels, J., Camera, A. and Sikes, C.: Sertraline treatment for premature ejaculation. J. Clin Psychopharmacol, 15: 341, 1995 85. McMahon, C. G.: Treatment of premature ejaculation with sertraline hydrochloride: a single-blind placebo controlled crossover study. J Urol, 159: 1935, 1998 86. Kim, S. W. and Paick, J. S.: Short-term analysis of the effects of as needed use of sertraline at 5 PM for the treatment of premature ejaculation. Urology, 54: 544, 1999 and Yilmiz, Y.: 87. Kara, H., Aydin, S., Ag argu n, M. Y., Odaba s, O. The efficacy of fluoxetine in the treatment of premature ejaculation: a double-blind, placebo controlled study. J Urol, 156: 1631, 1996 88. Lee, H. S., Song, D. H., Kim, C. H. and Choi, H. K.: An open clinical trial of fluoxetine in the treatment of premature ejaculation. J Clin Psychopharmacol, 16: 379, 1996 89. Haensel, S. M., Klem, T. M., Hop, W. C. and Slob, A. K.: Fluoxetine and premature ejaculation: a double-blind, cross-
Elsevier, vol. 5, pp. 12271244, 1978 37. Kilmann, P. R. and Auerbach, R.: Treatments of premature ejaculation and psychogenic impotence: a critical review of the literature. Arch Sex Behav, 8: 81, 1979 38. Trudel, G. and Proulx, S.: Treatment of premature ejaculation by bibliotherapy: an experimental study. Sex Marital Ther, 2: 163, 1987 39. Zeiss, R. A., Christensen, A. and Levine, A. G.: Treatment for premature ejaculation through male-only groups. J Sex Marital Ther, 4: 139, 1978 40. Schover, L. R., Friedman, J. M., Weiler, S. J., Heiman, J. R. and LoPiccolo, J.: Multiaxial problem-oriented system for sexual dysfunctions: an alternative to DSM-III. Arch Gen Psychiatr, 39: 614, 1982 41. Fanciullaci, F., Colpi, G. M., Beretta, G. and Zanollo, A.: Cortical evoked potentials in subjects with true premature ejaculation. Andrologia, 20: 326, 1988 42. Colpi, G. M., Fanciullaci, F., Beretta, G., Negri, L. and Zanollo, A.: Evoked sacral potentials in subjects with true premature ejaculation. Andrologia, 18: 583, 1986 43. Segraves, R. T., Saran, A., Segraves, K. and Maguire, E.: Clomipramine versus placebo in the treatment of premature ejaculation: a pilot study. J Sex Marital Ther, 19: 198, 1993 44. Waldinger, M. D.: The psychopharmacotherapy of premature ejaculation In: The 8th World Meeting on Impotence Research. Amsterdam, The Netherlands, August, 24 28, 1998. Edited by E. Meuleman, G. Lycklama a Nijeholt and D. van der Schueren. New York: Brunner/Routledge, pp. 99 102, 1998 45. Masters, W. H. and Johnson, V. E.: Human Sexual Response. Boston: Little, Brown & Co., 1966 46. Johnson, J.: Prognosis of disorders of sexual potency in the male. J Psychosom Res, 9: 195, 1965 47. Tuthill, J. F.: Impotence. Lancet, 1: 124, 1955 48. Cooper, A. J.: A factual study of male potency disorders. Br J Psychiatr, 114: 719, 1968 49. Eaton, H.: Clomipramine in the treatment of premature ejaculation. J Int Med Res, 1: 432, 1973 50. Adams, V.: Sex therapies in perspective. Psychol Today, August 1980 51. Aycock, L.: The medical management of premature ejaculation. J Urol, 62: 361, 1949 52. Damrau, F.: Premature ejaculation: use of ethyl aminobenzoate to prolong coitus. J Urol, 89: 936, 1963 53. Xin, Z. C., Seong, D. H. and Choi, H. K.: A double blind clinical trial on SS-cream on premature ejaculation. Int J Impotence Res, suppl., 6: D73, 1994 54. Berkovitch, M., Keresteci, A. G. and Koren, G.: Efficacy of prilocaine-lidocaine cream in the treatment of premature ejaculation. J Urol, 154: 1360, 1995 55. Shilon, M., Paz, G. F. and Hommonai, Z. T.: The use of phenoxybenzamine treatment in premature ejaculation. Fertil Steril, 42: 659, 1984 56. Hommonai, Z. T., Shilon, M. and Paz, G. F.: Phenoxybenzamine: an effective male contraceptive pill. Contraception, 29: 479, 1984 57. Beretta, G., Chelo, E., Fanciullacci, F. and Zanolla, A.: Effect of an alpha-blocking agent (phenoxybenzamine) in the management of premature ejaculation. Acta Eur Fertil, 17: 43, 1986 58. Cavallini, G.: Alpha-1 blockade pharmacotherapy in primitive psychogenic premature ejaculation resistant to psychotherapy. Eur Urol, 28: 126, 1995 59. Singh, H.: A case of inhibition of ejaculation as a side effect of Mellaril. Am J Psychiatry, 117: 1041, 1961 60. Freyhan, F. A.: Loss of ejaculation during mellaril treatment. Am J Psychiatry, 118: 171, 1961 61. Heller, J.: Another case of inhibition of ejaculation as a side effect of mellaril. Am J Psychiatry, 118: 173, 1961 62. Mellgren, A.: Treatment of ejaculatio praecox with thioridazine. Psychother Psychosom, 15: 454, 1967 63. Ditman, K. S.: Inhibition of ejaculation by chlorprothixene. Am J Psychiatry, 120: 1004, 1964 64. Bennett, D.: Treatment of ejaculatio praecox with monoamine oxidase inhibitors (letter to the editor). Lancet, 2: 1309, 1961 65. Rapp, M. S.: Two cases of ejaculatory impairment related to phenelzine. Am J Psychiatry, 136: 1200, 1979 66. Goodman, R. E.: An assessment of clomipramine (anafranil) in the treatment of premature ejaculation. J Int Med Res,
NEUROBIOLOGICAL APPROACH TO PREMATURE EJACULATION over, placebo-controlled study. J Clin Psychopharmacol, 18: 72, 1998 Tanner, B. A.: Two case reports on the modification of the ejaculatory response with the squeeze technique. Psychother Theory Res Pract, 10: 297, 1973 Waldinger, M. D., van De Plas, A., Pattij, T., Oorschot, R. V., Coolen, L. M., Veening, J. G. et al: The selective serotonin re-take inhibitors fluvoxamine and paroxetine differ in sexual inhibitory effects after chronic treatment. Psychopharmacology, 160: 283, 2002 Mos, J., Mollet, I., Tolboom, J. T., Waldinger, M. D. and Olivier, B.: A comparison of the effects of different serotonin reuptake blockers on sexual behaviour of the male rat. Eur Neuropsychopharmacol, 9: 123, 1999 Waldinger, M. D. and Olivier, B.: Selective serotonin reuptake inhibitor-induced sexual dysfunction: clinical and research considerations. Int Clin Psychopharmacol, suppl., 13: S27, 1998 Cantor, J. M., Binik, Y. M. and Pfaus, J. G.: Chronic fluoxetine inhibits sexual behavior in the male rat: reversal with oxytocin. Psychopharmacology, 144: 355, 1999 Li, Q., Levy, A. D., Cabrera, T. M., Brownfield, M. S., Battaglia, G. and van de Kar, L. D.: Long-term fluoxetine, but not desipramine, inhibits the ACTH and oxytocin responses to the 5-HT1A agonist, 8-OH-DPAT, in male rats. Brain Res, 630: 148, 1993 Carmichael, M. S., Humbert, R., Dixen, J., Palmisano, G., Greenleaf, W. and Davidson, J. M.: Plasma oxytocin increases in the human sexual response. J Clin Endocrinol Metab, 64: 27, 1987 Murphy, M. R., Seckl, J. R., Burton, S., Checkley, S. A. and Lightman, S. L.: Changes in oxytocin and vasopressin secretion during sexual activity in men. J Clin Endocrinol Metab, 65: 738, 1987 Ahlenius, S., Larsson, K., Svensson, L., Hjorth, S., Carlsson, A., Lindberg, P. et al: Effects of a new type of 5-HT receptor agonist on male rat sexual behaviour. Pharmacol Biochem Behav, 15: 785, 1981 Foreman, M. M., Hall, J. L. and Love, R. L.: The role of the 5-HT2 receptor in the regulation of sexual performance of male rats. Life Sci, 45: 1263, 1989 Waldinger, M. D., Berendsen, H. H. G., Blok, B. F., Olivier, B. and Holstege, G.: Premature ejaculation and serotinergic antidepressants-induced delayed ejaculation: the involvement of the serotonergic system. Behav Brain Res, 92: 111, 1998 Marson, L. and McKenna, K. E.: The identification of a brainstem site controlling spinal sexual reflexes in male rats. Brain Res, 515: 303, 1990 Yells, D. P., Prendergast, M. A., Hendricks, S. E. and Nakamura, M.: Fluoxetine-induced inhibition of male rat copulatory behavior: modification by lesions of the nucleus paragigantocellularis. Pharmacol Biochem Behav, 49: 121, 1994 MacLean, P. D.: Brain mechanisms of primal sexual functions and related behavior. In: Sexual Behavior: Pharmacology and Biochemistry. Edited by M. Sandler and G. L. Gessa. New York: Raven Press, 1975 Veening, J. G. and Coolen, L. M.: Neural activation following
2367
90. 91.
105. 106.
92.
107.
93.
108. 109. 110. 111.
94. 95.
96.
112. 113. 114. 115. 116. 117. 118. 119.
97.
98.
99. 100.
101. 102.
120. 121.
103.
104.
sexual behavior in the male and female rat brain. Behav Brain Res, 92: 181, 1998 Coolen, L. M., Peters, H. J. and Veening, J. G.: Fos immunoreactivity in the rat brain following consummatory elements of sexual behavior: a sex comparison. Brain Res, 738: 67, 1996 Coolen, L. M., Olivier, B., Peters, H. J. and Veening, J. G.: Demonstration of ejaculation-induced neural activity in the male rat brain using 5-HT1A agonist 8-OH-DPAT. Physiol Behav, 62: 881, 1997 Coolen, L. M., Peters, H. J. and Veening, J. G.: Anatomical interrelationships of the medial preoptic area and other brain regions activated following male sexual behavior: a combined fos and tract-tracing study. J Comp Neurol, 397: 421, 1998 Xin, Z. C., Choi, Y. D., Rha, K. H. and Choi, H. K.: Somatosensory evoked potentials in patients with primary premature ejaculation. J Urol, 158: 451, 1997 Opsomer, R. J., Guerit, J. M., Wese, F. X. and Van Cangh, P. J.: Pudendal cortical somatosensory evoked potentials. J Urol, 135: 1216, 1986 Diagnostic and Statistical Manual of Mental Disorders, DSM-IV, 4th ed. Washington, D. C.: American Psychiatric Association, 1994 Waldinger, M. D., Hengeveld, M. W., Zwinderman, A. H. and Olivier, B.: An empirical operationalization study of DSM-IV diagnostic criteria for premature ejaculation. Int J Psychiatr Clin Pract, 2: 287, 1998 Reading, A. and Wiest, W.: An analysis of self-reported sexual behavior in a sample of normal males. Arch Sex Behav, 13: 69, 1984 Nathan, S. G.: The epidemiology of the DSM-III psychosexual dysfunctions. J Sex Marital Ther, 12: 267, 1986 Spector, K. R. and Boyle, M.: The prevalence and perceived aetiology of male sexual problems in a non-clinical sample. Br J Med Psychol, 59: 351, 1986 Spector, I. P. and Carey, M. P.: Incidence and prevalence of the sexual dysfunctions: a critical review of the empirical literature. Arch Sex Behav, 19: 389, 1990 Grenier, G. and Byers, E. S.: The relationships among ejaculatory control, ejaculatory latency, and attempts to prolong heterosexual intercourse. Arch Sex Behav, 26: 27, 1997 Grenier, G. and Byers, E. S.: Rapid ejaculation: a review of conceptual, etiological, and treatment issues. Arch Sex Behav, 24: 447, 1995 Stoneham, M. D., Everitt, B. J., Hansen, S., Lightman, S. L. and Todd, K.: Oxytocin and sexual behaviour in the male rat and rabbit. J Endocrinol, 107: 97, 1985 Argiolas, A., Collu, M., DAquila, P., Gessa, G. L., Melis, M. R. and Serra, G.: Apomorphine stimulation of male copulatory behavior is prevented by the oxytocin antagonist d(CH2)5Tyr(Me)-Orn8-Vasotocin in rats. Pharmacol Biochem Behav, 33: 81, 1989 Argiolas, A., Melis, M. R. and Gessa, G. L.: Oxytocin: an extremely potent inducer of penile erection and yawning in male rats. Eur J Pharmacol, 130: 265, 1986 Waldinger, M. D.: Rapid ejaculation. In: Handbook of Clinical Sexuality for Mental Health Professionals. Edited by S. B. Levine, C. B. Risen and S. E. Althof. Unpublished data
Vous aimerez peut-être aussi
- Assessment of Hematuria, Review Article Medical Clinics of North America, Volume 95, Issue 1, January 2011Document7 pagesAssessment of Hematuria, Review Article Medical Clinics of North America, Volume 95, Issue 1, January 2011Diana Pardo ReyPas encore d'évaluation
- 09 Prostate Cancer LRDocument154 pages09 Prostate Cancer LRDiana Pardo ReyPas encore d'évaluation
- 1 Eua Guidelines Urolitiasis 2013Document100 pages1 Eua Guidelines Urolitiasis 2013Diana Pardo ReyPas encore d'évaluation
- (2011) Palliative Care in Urology SURG - Clin.n.amDocument16 pages(2011) Palliative Care in Urology SURG - Clin.n.amDiana Pardo ReyPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- SadasdDocument3 pagesSadasdrotsacreijav666666Pas encore d'évaluation
- Basic ChineseDocument7 pagesBasic ChineseDaniyal AliPas encore d'évaluation
- Unit 4 Study GuideDocument4 pagesUnit 4 Study GuideVanshika GuptaPas encore d'évaluation
- Coupled Electrophysiological, Hemodynamic, and Cerebrospinal Fluid Oscillations in Human SleepDocument5 pagesCoupled Electrophysiological, Hemodynamic, and Cerebrospinal Fluid Oscillations in Human Sleepbeatles guyPas encore d'évaluation
- Toyota Production System: Merits, Demerits and Challenges: SCM AssignmentDocument15 pagesToyota Production System: Merits, Demerits and Challenges: SCM AssignmentNeerAj NidrePas encore d'évaluation
- The Speak English Gym Differentiation and Innovations.Document2 pagesThe Speak English Gym Differentiation and Innovations.surnam63Pas encore d'évaluation
- Cindy Juarez ResumeDocument2 pagesCindy Juarez ResumeCindy Juárez-ChozaPas encore d'évaluation
- Anger Management For Substance Abuse and Mental Health ClientsDocument19 pagesAnger Management For Substance Abuse and Mental Health ClientsBijoyPas encore d'évaluation
- Tic Poster FinalDocument1 pageTic Poster Finalapi-337168518Pas encore d'évaluation
- Chapter 14 HciDocument5 pagesChapter 14 HciSweetMikanPas encore d'évaluation
- Non-Motivated Functions of ArtDocument3 pagesNon-Motivated Functions of ArtJamee Bruha100% (2)
- Zuberbu - 2005 - The Phylogenetic Roots of Language Evidence From Primate Communication and CognitionDocument5 pagesZuberbu - 2005 - The Phylogenetic Roots of Language Evidence From Primate Communication and CognitionJohnPas encore d'évaluation
- Marketing Analytics Benchmark ReportDocument10 pagesMarketing Analytics Benchmark ReportDemand MetricPas encore d'évaluation
- 1460-Article Text-4690-1-10-20240222Document10 pages1460-Article Text-4690-1-10-20240222saladagapepitoirene06Pas encore d'évaluation
- Rizal's Concept On Nation BuildingDocument12 pagesRizal's Concept On Nation BuildingJerome ChuaPas encore d'évaluation
- Discuss Pride and Prejudice As Jane Austen's World On Two Inches of IvoryDocument4 pagesDiscuss Pride and Prejudice As Jane Austen's World On Two Inches of IvoryFaisal JahangeerPas encore d'évaluation
- April Exam Takers CommentsDocument3 pagesApril Exam Takers CommentsAhmed EbrahimPas encore d'évaluation
- Briana BagdassianDocument2 pagesBriana BagdassianJames BridgesPas encore d'évaluation
- As Man ThinkethDocument18 pagesAs Man ThinkethKulvir RickPas encore d'évaluation
- This Study Resource Was: Organizational Behaviour Case StudiesDocument9 pagesThis Study Resource Was: Organizational Behaviour Case StudiesVaibhavi JainPas encore d'évaluation
- The Nine Enneagram Type Descriptions ExplainedDocument32 pagesThe Nine Enneagram Type Descriptions Explained7ThorHimmelPas encore d'évaluation
- Communciation Models-HandoutsDocument2 pagesCommunciation Models-HandoutsMarla Joy LucernaPas encore d'évaluation
- Registration Fee Rs.500/-: PatronDocument2 pagesRegistration Fee Rs.500/-: PatronnathxeroxPas encore d'évaluation
- Canayon, S. MoviereviewDocument3 pagesCanayon, S. MoviereviewJohn Mark Gallano CanayonPas encore d'évaluation
- LP Grade 7Document1 pageLP Grade 7ayatolla ayatollaTM100% (1)
- Resumen ManagementDocument12 pagesResumen ManagementKarinaPas encore d'évaluation
- Religious Television Viewing and Impact On Political BehaviorDocument5 pagesReligious Television Viewing and Impact On Political Behaviorbatyala vaniPas encore d'évaluation
- 80957667-Dissertation MSC DFSMDocument98 pages80957667-Dissertation MSC DFSMSanjay JamwalPas encore d'évaluation
- Caseworker Test GuideDocument9 pagesCaseworker Test GuideemigrenycPas encore d'évaluation
- Training Manual (R. Adjetey)Document26 pagesTraining Manual (R. Adjetey)jeremiah yanneyPas encore d'évaluation