REVIEWS
IMAJ VOL 14 july 2012
The Link between Polycystic Ovarian Syndrome and Type 2 Diabetes: Preventive and Therapeutic Approach in Israel
Daniela Jakubowicz MD1, Julio Wainstein MD1 and Roy Homburg MD2
1 2
Diabetes Unit, Wolfson Medical Center, Holon, and Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel Department of Obstetrics and Gynecology, Barzilai Medical Center, Ashkelon, Israel
KEy WoRDS: polycystic ovarian syndrome (PCOS), type 2 diabetes, insulin resistance, hyperinsulinemia, hyperandrogenism
IMAJ 2012; 14: 442-447
P crinopathy, affecting 6%10% of women of reproductive
olycystic ovarian syndrome is the most common endo-
age [1]. It is the major cause of female anovulatory infertility and affects women across their lifespan. It is characterized by disturbed ovarian function, usually manifests as oligomenorrhea or amenorrhea, infertility and enlarged polycystic ovaries, and is associated with clinical and/or biochemical evidence of hyperandrogenism [2]. Endocrine abnormalities may include increased free testosterone levels, low sex hormone binding globulin, and high luteinizing hormone/ follicle-stimulating hormone ratio [2,3]. PCOS was originally thought to affect solely women of child-bearing age because of the presence of infertility. However, current evidence has shown that insulin resistance and the compensatory hyperinsulinemia is a central feature of PCOS [4,5]. Women with PCOS have a high incidence of insulin resistance [4], which is accompanied by compensatory hyperinsulinemia and therefore presents an increased risk for type 2 diabetes [4-6]. In vitro and in vivo studies have shown that in women with PCOS the sensitivity of glucose metabolism to insulin is subnormal and modest hyperinsulinemia prevails [3]. Insulin resistance affects approximately 6580% of women with PCOS and appears to play an important pathogenic role in the hyperandrogenism of both obese and lean women with PCOS [5]. The recognition that the disorder is associated with insulin resistance has provided insight not only into the pathogenesis of PCOS but also into its related short and long-term complications, with significant risk for the development of obesity, metabolic syndrome, impaired glucose tolerance, type 2 diabetes, dyslipidemia, hypertension and atherosclerosis [3,5,6].
1
PCOS = polycystic ovarian syndrome
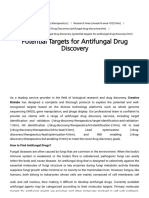
PAThophySIoLoGy of INSULIN RESISTANCE IN PCOS Specific abnormalities of insulin metabolism identified in women with PCOS include impaired suppression of hepatic gluconeogenesis and abnormalities in insulin receptor signaling that adversely affect the insulin-mediated glucose transport into the muscles, being reduced by 3540% in PCOS women independent of obesity [3,5,7]. Pancreatic -cell dysfunction with an increased basal secretion of insulin and inadequate postprandial response has also been described in PCOS women even when, as a result of weight loss, an improvement in glucose tolerance was observed [6]. Adipose tissue, stored mainly in the abdominal fat in PCOS women, has an aberrant morphology and produces less adiponectin than matched controls. This may further aggravate the insulin resistance. Furthermore, activity of the enzyme lipoprotein lipase is low, which can also affect fat metabolism [8]. In PCOS, the insulin receptor defect adversely affects the insulin-mediated glucose transport into the muscles [3,7]. As a result, the glucose in blood remains elevated for a longer time and further stimulates pancreatic beta cells, which in order to improve muscular glucose uptake increase their secretion of insulin in a compensatory manner [3] [Figure 1]. This compensatory hyperinsulinemia of PCOS directly stimulates testosterone production by ovarian thecal cells, promoting the hyperandrogenic state [9] that is responsible for hirsutism, acne, alopecia, higher waist to hip ratio, and the detrimental effects on follicular growth, leading to the anovulatory state, menstrual disturbances and the microcystic appearance of the ovaries that characterize this syndrome [3,5,9]. Insulin stimulates the ovarian production of androgen by activating its homologous receptor [9] in the ovaries of PCOS women that appear to remain sensitive to insulin, or perhaps hypersensitive to it, even when classic target tissues such as muscle and fat manifest resistance to insulin action [10]. In addition, hyperinsulinemia inhibits the hepatic production of sex hormone binding globulin [5], further increasing circulating free testosterone levels. Finally, insulin impedes ovulation, either by directly affecting follicular development, or by indirectly increasing intraovarian androgen levels or altering gonadotropin secretion [5].
442
IMAJ VOL 14 july 2012
REVIEWS
Figure 1. In PCOS the compensatory hyperinsulinemia in response to insulin receptor The molecular mechanism of insulin resistance in PCOS defect in the muscles directly stimulates testosterone production by ovarian thecal is controversial. However, several studies have shown that cells, promoting the hyperandrogenic state (original Illustration of the rst author, insulin resistance in PCOS is due to post-binding defects in appearing as a poster presentation) signal transduction and that there are multiple defects in insulin action in PCOS that affect metabolism [7,11,12]. Insulin action is initiated when insulin binds to the insulin receptors-1 and 2. Insulin binding induces autophosphorylation of the insulin receptors on specific tyrosine residues and increases the intrinsic kinase activity of its -subunit. One pathway proceeds through IRS-1 and IRS-2 and depends on activation of phosphatidylinositol 3-kinase to mediate the insulin actions on glucose metabolism, antilipolysis and protein synthesis. Another pathway proceeds through binding of tyrosinephosphorylated IRS-1 and IRS-2, leading via p21Ras and Raf-1 to activation of the mitogen-activated protein kinase isoforms of extracellular signal-regulated kinase ERK-1 and 2, thus mediating mitogenic and other gene-regulatory actions of and IRS-1 Ser312 phosphorylation in PCOS women result in insulin. ERK-1 and 2 are members of a family of serine/threoameliorated insulin resistance [12]. nine kinases, including p38 MAPK and c-Jun NH2-terminal Furthermore, MAPK activity that is constitutively kinase, that play important roles in cellular proliferation, difincreased in the skeletal muscle of women with PCOS implies ferentiation, apoptosis as well as inflammation [13]. that ERK-1 and 2 or ERK-regulated kinases are responsible Previous studies have demonstrated that in PCOS there is for the increased Ser312 phosphorylation of IRS-1 [14]. also a post-binding defect in insulin signaling in adipocyte and These observations provide strong support for the hypothdecreased activity of PI3 -kinase in muscle biopsies during esis that increased Ser312 phosphorylation is an important mechanism for insulin resistance in PCOS. euglycemic hyperinsulinemic clamps. It was suggested that the It was previously reported that obese women have lower impaired action of insulin on glycogen synthesis in cultured levels of insulin receptor, IRS and PI3-kinase than non-obese skin fibroblasts from POCS women is associated with constituwomen [16]; however, a recent study showed that the levels tively increased insulin receptor -subunit serine phosphoryof activated ERK-1 and 2, Ser312lation and decreased insulin receptor In PCOS, the compensatory phosphorylated IRS-1, tyrosinetyrosine kinase activity [7,11,12]. hyperinsulinemia directly phosphorylated IRS-1, IR -subunit, It was also thought that the decreased IRS-1 tyrosine phosphorylation and stimulates ovarian testosterone PI3-kinase and GLUT-4 were similar increased IRS-1 Ser312 phosphorylain both obese and non-obese PCOS production promoting the tion seen in women with PCOS may be women and lower than in controls, hyperandrogenic state the initial defect in insulin resistance in suggesting that non-obese and obese PCOS [11,14]. Increased IRS-1 Ser312 phosphorylation would PCOS women have a similar risk of developing insulin resisinhibit insulin receptor tyrosine kinase activity and prevent tance or type 2 diabetes [12]. The decrease of compensatory the signal propagation that underlies many biological effects of hyperinsulinemia in PCOS via a reduction in IRS-1 Ser312 insulin, leading to decreased activation of the signaling pathphosphorylation may therefore be an effective tool for reducway. Evidence for this hypothesis comes from the observed ing the risk of type 2 diabetes in women with PCOS. reversal of impaired insulin receptor signaling by serine kinase Clinical studies have shown that lowering circulating insuinhibitors in human fibroblasts from women with PCOS [15]. lin levels resulted in reduction of serum testosterone levels It was reported that ERK-1 and 2 are responsible for and increased frequency of ovulation and fertility in PCOS constitutive phosphorylation of IRS-1 Ser312 in women women. Those trials include the inhibition of insulin release with PCOS, and that Ser312 phosphorylation of IRS-1 is with diazoxide [17] and improvement of insulin sensitivity constitutively increased in cultured skeletal muscle cells with diet-induced weight loss [18] by administration of metfrom PCOS women [14], but the mechanism by which ERK-1 formin, which resulted in decreases in ovarian 17,20-lyase and 2 regulates IRS-1 Ser312 phosphorylation is unknown. activity and ovarian secretion of androgens [19,20], and of Nevertheless, it was found that decreased ERK1/2 activation other insulin sensitizers, i.e., rosiglitazone [10]. In women with the syndrome, long-term treatment with metformin
2 3 5 4 6
IRS = insulin receptor substrate MAPK = mitogen-activated protein kinase PI = phosphatidylinositol
MAPK = mitogen-activated protein kinase IR = insulin receptor
443
REVIEWS
IMAJ VOL 14 july 2012
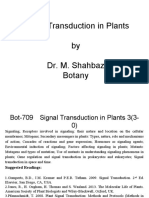
Figure 2. Prevalence rates of impaired glucose tolerance in PCOS is 3040% and the prevalence of type 2 diabetes 510%, which is substantially higher than found in a major population-based study (Second National Health and Nutrition Survey) of U.S. women of similar age and BMI (7.8% IGT and 1.0% type 2 diabetes). Original picture, based on Legro at al., 1999 [4].
30-50% 30% 20% 10% 7.8% 1.0%
PCOS Normal
IGT
Type 2 Diabetes
PCOS women the prevalence of IGT is 3050%, and that of type 2 diabetes 510%. In addition, the conversion from IGT to type 2 diabetes is increased [4,23]. A recent study showed that PCOS women have twofold higher odds for subsequent development of type 2 diabetes: 23.1% in PCOS woman versus 13.1% in non-PCOS women [25]. Women with PCOS and normal glucose tolerance at baseline have a 16% conversion rate per year to type 2 diabetes. Thus by the age of 30 years, 3050% of obese PCOS women develop IGT or overt type 2 diabetes. This is a three to sevenfold greater risk than in an age-comparable population [23]. More recently a systematic review and meta-analysis [26] show that women with PCOS have an elevated prevalence of IGT, type 2 diabetes and metabolic syndrome in both BMI and non-BMI-matched studies.
8
ShoULD WoMEN WITh PCOS RECEIVE METfoRMIN ThERApy? resulted in increased ovulation, improved menstrual cyclicity, and reduced serum androgen levels [9,19,20]. Metformin, a biguanide, is the most widely used drug for the treatment of type 2 diabetes worldwide. Its primary action is to inhibit hepatic glucose production, but it also increases the PCOS AND METAboLIC SyNDRoME sensitivity of peripheral tissues to insulin [27]. The increase in insulin sensitivity, which contributes to the efficacy of The prevalence of the metabolic syndrome is two to threefold metformin in the treatment of diabetes, has also been shown higher among women with PCOS compared to normal women in non-diabetic women with PCOS [24]. matched for age and body mass index, while 20% of women with With regard to diabetes, two major randomized clinical PCOS under 20 years old have the metabolic syndrome [21]. trials the Indian Diabetes Prevention Programme (IDPPA ccording to the National Cholesterol Education 1) [28] and the U.S. Diabetes Program Adult Treatment Panel Prevention Program (DPP) [29] III (NCEP-ATP III), the prevaObese PCOS and non-obese lence of metabolic syndrome has PCOS women are at high risk of have shown that the use of metformin decreases the relative risk been reported to be between 33% metabolic syndrome and type 2 for progression to type 2 diabetes and 46% in women with PCOS, diabetes (by 26% and 31%, respectively) compared to 6% in normal women among patients with IGT at baseline. Furthermore, after the aged 2029 years and 15% in women aged 3039 [21,22] discontinuation of metformin in the U.S. Diabetes Prevention Furthermore, the metabolic syndrome is present in 80% of Program , diabetes developed in fewer subjects than would PCOS women who are also obese. Hence, the prevalence of the metabolic syndrome is two to threefold higher in women have been expected [30] with PCOS compared to age- and BMI -matched non-PCOS In an uncontrolled retrospective study of 50 women with the polycystic ovary syndrome treated with metformin for controls, regardless of BMI [4,6,22]. an average of 43 months at an academic medical center, there was no progression to type 2 diabetes even though 11 women RISk foR TypE 2 DIAbETES IN PCOS WoMEN (22.0%) had IGT at baseline [31]. The annual conversion rate from normal glucose tolerance to impaired glucose tolerThe prevalence of type 2 diabetes is tenfold higher among ance was only 1.4%, as compared to 1619% reported in the young women with PCOS than among normal women, and literature [4,6] for women with PCOS who were not taking impaired glucose tolerance or overt type 2 diabetes develops metformin. Metformin may actually retard progression to by the age of 30 years in 3050% of obese women with PCOS glucose intolerance in affected women [31]. [4,6,22,23] [Figure 2] Furthermore, lifestyle intervention together with the use Insulin resistance in PCOS appears to be responsible for of metformin can prevent IGT progression to type 2 diabetes this predisposition to develop type 2 diabetes [24]. In fact, in
9 7
BMI = body mass index
IGT = impaired glucose tolerance
444
IMAJ VOL 14 july 2012
REVIEWS
and reduce the risk of cardiovascular events in patients with PCOS, strengthening the argument for early detection of IGT, especially in this group of women who are at high risk of type 2 diabetes [25]. Metformin may decrease circulating androgen levels and improve menstrual cyclicity, and is of benefit in improving clinical pregnancy and ovulation rates as well as addressing the traditional goals of glucose metabolism in long-term treatment. However, there is no evidence that metformin improves live birth rates, whether used alone or in combination with clomiphene or when compared with clomiphene. Therefore, the use of metformin in improving reproductive outcomes in women with PCOS appears to be limited [32]
ignored due to a failure in making the connection between PCOS and diabetes type 2 and the opportunity for true preventive medicine is missed. Gynecologists tend naturally to concentrate on the gynecologic symptoms of irregular periods and infertility, whereas diabetologists often fail to make the connection between the two conditions. In addition, dermatologists encountering adolescents with hirsutism or persistent acne will sometimes treat symptomatically with medication that may further worsen the insulin resistance [35] without recognizing that they have PCOS and another opportunity to prevent diabetes in later life is missed. In view of the long-term consequences associated with insulin resistance and impaired glucose tolerance related to the development of type 2 diabetes and subsequently cardiovascular disease, it is crucial PREVALENCE of DIAbETES IN ISRAEL that young girls with this disorder be diagnosed and treated. PCOS often manifests around the time of menarche Diabetes is one of the most frequent chronic diseases in the as irregular and often lengthy menstrual cycles [36]. modern word and is associated with striking comorbidities and Unfortunately, PCOS is often unrecognized and undiagnosed serious health implications for patients, health care systems, at this time because most adolescents do not have regular and society. In Israel as in other countries, the prevalence menstrual cycles [37]. In adolescent girls with irregular of diabetes has risen over the last few decades, reaching a menstrual cycles for more than 2 years after menarche, it is prevalence of 6.4% in adults over 18 years old, with an annual highly likely that the underlying cause is not physiological increase of 0.2%. The prevalence of diabetes increases with but PCOS. This is especially true if age, reaching 15% among people aged 3040, while among those aged 65 or In Israel, the incidence of type the irregular periods are accompaabove the prevalence is 25% [33]. 2 diabetes is markedly high and nied by persistent acne or hirsutism. In Israel, with an estimated is a leading cause of morbidity, Although the prescribed treatment for irregular menstrual cycles is population of 7 million, there are more than 490,000 diabetics. Recent particularly in those over age 40 oral contraceptive pills, particularly those containing progestins with epidemiological evaluation also anti-androgenic actions if the diagnosis of PCOS has been reported that there are an additional 200,000 diabetics who correctly made, this treatment will have no effect on the have the disease but were not diagnosed [34]. Since diabetes potential for developing diabetes. decreases life expectancy and is a health-threatening condiWomen with PCOS are often diagnosed at a much later tion, all measures to prevent the development of diabetes are stage, usually when they seek treatment for infertility. of pivotal importance, especially in those groups with a high Again, the treatment for infertility in this case will be the predisposition like PCOS. primary concern of the gynecologist, while any thoughts of the future consequences of PCOS and the metabolic synCUES IN ThE pREVENTIoN of TypE 2 DIAbETES IN PCOS drome are disregarded. WoMEN IN ISRAEL Two main factors must be considered regarding PCOS women. The first involves cyclic control of irregular menIn Israel, the incidence of type 2 diabetes is markedly high struation cycles, fertility, acne and hirsutism and other and is a leading cause of morbidity, particularly in those over hyperandrogenic symptoms. The second involves avoidance age 40. As described above, there is a strong association of of the long-term sequelae that are associated with obesity, PCOS, the metabolic syndrome and type 2 diabetes [6,23]. insulin resistance, glucose intolerance, subsequent dyslipWhen considering the prevention of such a debilitating idemia, hypertension, and type 2 diabetes, all known to be condition as diabetes, it should be remembered that PCOS significant risk factors for the development of cardiovascuwill almost invariably express itself soon after menarche. lar disease [37]. Because of the connection between insulin When the diagnosis of PCOS is made, this should serve as resistance and PCOS, it is recommended that all adolescents a beacon flashing a warning signal that diabetes may well suspected of having the disorder be screened by fasting blood be encountered later in life and that its prevention should glucose levels. If fasting blood glucose levels are elevated, the be considered when PCOS is initially diagnosed. However, next step is to order a 2 hour 75 g oral glucose tolerance test in Israel, it would seem that these warning signals are often
445
REVIEWS
IMAJ VOL 14 july 2012
to confirm glucose intolerance or type 2 diabetes [38]. In fact, most authorities recommend the OGTT as a screening test in all obese adolescent females. Whereas the testing for insulin resistance by the gold standard of the insulin clamp is not recommended because of the time-consuming nature of the test and the expense [36], HOMA-IR (homeostasis model assessment-estimated insulin resistance) may give a much simpler indication of the presence of insulin resistance. However, the OGTT is probably the test of choice for pragmatic diagnosis. The most cost-effective predictor for insulin resistance and cardiovascular risk is probably a waist circumference of > 88 cm [21]. If the adolescent is found through laboratory testing to have glucose intolerance or type 2 diabetes, testing should probably be repeated at yearly intervals. Since disturbances in glucose metabolism can cause lipid abnormalities, particularly increased total cholesterol, decreased high density lipoprotein and increased low density lipoprotein, it is recommended that lipid assays be performed as well. Determining baseline lipid levels is also important because many of the treatments, specifically combined oral contraceptive pills, can also alter these values and may impact on the therapeutic management of PCOS women. As for the actual prevention of diabetes in the woman with PCOS, lifestyle changes, diet and exercise under expert supervision, especially for those who are obese, is the treatment of choice. As mentioned above, metformin may also be used in the long term but more evidence on the efficiency of this treatment is still required. With long-term metformin there should also be awareness that homocysteine levels may increase and that multivitamin therapy may be necessary to control the levels [39]. A revealing study from the Diabetes Prevention research group [40] showed that lifestyle changes reduced the cumulative incidence of diabetes by 58% compared to 31% with metformin. In conclusion, the purpose of this article is to increase the awareness of physicians, whether gynecologists, fertility experts, diabetologists, endocrinologists or others, of the strong link between PCOS, insulin resistance, metabolic syndrome, and the incidence of diabetes. It is hoped that this increased awareness will bring about a concerted effort in Israel to reduce the incidence of diabetes.
1 0
on the definition and diagnosis of polycystic ovarian syndrome. Hum Reprod 2002; 17 (10): 2495-9. 3. Dunaif A. Insulin resistance and the polycystic ovary syndrome: mechanism and implications for pathogenesis. Endocr Rev 1997; 18: 774-800. 4. Legro RS, Kunselman AR, Dodson WC, Dunaif A. Prevalence and predictors of risk for type 2 diabetes mellitus and impaired glucose tolerance in polycystic ovary syndrome: a prospective, controlled study in 254 affected women. J Clin Endocrinol Metab 1999; 84: 165-9. 5. Nestler JE. Role of hyperinsulinemia in the pathogenesis of the polycystic ovary syndrome, and its clinical implications. Semin Reprod Endocrinol 1997; 15: 11122. 6. Ehrmann DA, Barnes RB, Rosenfield RL, Cavaghan MK, Imperial J. Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome. Diabetes Care 1999; 22: 141-6. 7. Ciaraldi TP, el-Roeiy A, Madar Z, Reichart D, Olefsky JM, Yen SS. Cellular mechanisms of insulin resistance in polycystic ovarian syndrome. J Clin Endocrinol Metab 1992; 75 (2): 577-83. 8. Manners-Holm L, Leonhardt H, Kullberg J. Adipose tissue has aberrant morphology and function in PCOS: enlarged adipocytes and low serum adiponectin, but not circulating sex steroids, are strongly associated with insulin resistance. J Clin Endocrinol Metab 2011; 96 (2): E304-11. 9. Nestler JE, Jakubowicz DJ, de Vargas AF, Brik C, Quintero N, Medina F. Insulin stimulates testosterone biosynthesis by human thecal cells from women with polycystic ovary syndrome by activating its own receptor and using inositolglycan mediators as the signal transduction system. J Clin Endocrinol Metab 1998; 83: 2001-5. 10. Baillargeon JP, Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Nestler JE. Effects of metformin and rosiglitazone, alone and in combination, in nonobese women with polycystic ovary syndrome and normal indices of insulin sensitivity. Fertil Steril 2004; 82: 893-902. 11. Dunaif A, Wu X, Lee A, Diamanti-Kandarakis E. Defects in insulin receptor signaling in vivo in the polycystic ovary syndrome (PCOS). Am J Physiol Endocrinol Metab 2001; 281: (2): E392-9. 12. Seow KM, Juan CC, Hsu YP, Hwang JL, Huang LW, Ho LT Amelioration of insulin resistance in women with PCOS via reduced insulin receptor substrate-1 Ser312 phosphorylation following laparoscopic ovarian electrocautery. Hum Reprod 2007; 22 (4): 1003-10. 13. Virkamaki A, Ueki K, Kahn CR. Proteinprotein interaction in insulin signaling and the molecular mechanisms of insulin resistance. J Clin Invest 1999; 103: 931-43. 14. Corbould A, Zhao H, Mirzoeva S, Aird F, Dunaif A. Enhanced mitogenic signaling in skeletal muscle of women with polycystic ovary syndrome. Diabetes 2006; 55: 751-9. 15. Li M, Youngren JF, Duanif A, et al. Decreased insulin receptor (IR) autophosphorylation in fibroblasts from patients with PCOS: effects of serine kinase inhibitors and IR activators. J Clin Endocrinol Metab 2002; 87: 4088-93. 16. Goodyear LJ, Giorgino F, Sherman LA, Carey J, Smith RJ, Dohm GL. Insulin receptor phosphorylation, insulin receptor substrate-1 phosphorylation, and phosphatidylinositol 3-kinase activity are decreased in intact skeletal muscle strips from obese subjects. J Clin Invest 1995; 95: 2195-204. 17. Nestler JE, Barlascini CO, Matt DW, et al. Suppression of serum insulin by diazoxide reduces serum testosterone levels in obese women with polycystic ovary syndrome. J Clin Endocrinol Metab 1989; 68: 1027-32. 18. Jakubowicz DJ, Nestler JE.17 alpha-Hydroxyprogesterone responses to leuprolide and serum androgens in obese women with and without polycystic ovary syndrome offer dietary weight loss. J Clin Endocrinol Metab 1997; 82 (2): 556-60. 19. Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med 1996; 335: 617-23. 20. Cheang KI, Sharma ST, Nestler JE. Is metformin a primary ovulatory agent in patients with polycystic ovary syndrome? Gynecol Endocrinol 2006; 22: 595-604. 21. Apridonidze T, Essah PA, Iuorno MJ, Nestler JE. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2005; 90: 1929-35. 22. Ehrmann DA, Liljenquist DR, Kasza K, Azziz R, Legro RS, Ghazzi MN. Prevalence and predictors of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2006; 91: 48-53.
Corresponding author:
Dr. D. Jakubowicz Diabetes Unit, Wolfson Medical Center, Holon 58100, Israel email: daniela.jak@gmail.com
References
1. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 1998; 83: 3078-82. 2. Homburg R. What is polycystic ovarian syndrome? A proposal for a consensus OGTT = oral glucose tolerance test
446
IMAJ VOL 14 july 2012
REVIEWS
23. Legro RS, Gnatuk CL, Kunselman AR, Dunaif A. Changes in glucose tolerance over time in women with polycystic ovary syndrome: a controlled study. J Clin Endocrinol Metab 2005; 90: 3236-42. 24. Sharma ST, Nestler JE. Prevention of diabetes and cardiovascular disease in women with PCOS: treatment with insulin sensitizers. Best Pract Res Clin Endocrinol Metab 2006; 20: 245-60. 25. Wang ET, Calderon-Margalit R, Cedars MI, et al. Polycystic ovary syndrome and risk for long-term diabetes and dyslipidemia. Obstet Gynecol 2011; 117 (1): 6-13. 26. Moran LJ, Misso ML, Wild RA, Norman RJ. Impaired glucose tolerance, type 2 diabetes and metabolic syndrome in polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update 2010; 16 (4): 347-63. 27. Bailey CJ, Turner RC. Metformin. N Engl J Med 1996; 334: 574-9. 28. Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006; 49: 289-97. 29. Diabetes Prevention Program (Diabetes Prevention Program Research Group). Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346: 393-403. 30. Diabetes Prevention Program Research Group. Effects of withdrawal from metformin on the development of diabetes in the Diabetes Prevention Program. Diabetes Care 2003; 26: 977-80. 31. Sharma ST, Wickham EP III, Nestler JE. Changes in glucose tolerance with metformin treatment in polycystic ovary syndrome: a retrospective analysis. Endocr Pract 2007; 13: 373-9. 32. Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-sensitising drugs
(metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev 2010; 20 (1): CD003053. 33. Porath A., Rabinowitz G,Raskin SegalA, Weitzman R, Ben Said S. Quality Indicators for Community Health Care in Israel 20032007 Public Report (2008) http://132.72.100.18/HealthReports/Download/public_report_ English_2005-2007.pdf, Accessed 8 August 2008 34. Wilf-Miron R, Peled R, Yaari E, et al. Disparities in diabetes care: role of the patients socio-demographic characteristics. BMC Public Health2010;10: 729. 35. Diamanti-Kandarakis E, Baillargeon JP, Iuorno MJ, Jakubowicz DJ, Nestler JE. A modern medical quandary: polycystic ovary syndrome, insulin resistance, and oral contraceptive pills. J Clin Endocrinol Metab 2003; 88: 1927-32. 36. Richardson, M. Current perspectives in polycystic ovary syndrome. Am Fam Phys 2003; 68 (4): 697. 37. Sheehan M. Polycystic ovarian syndrome: diagnosis and management. Clin Med Res 2004; 2 (1): 13-27. 38. Meisler J. Toward optimal health: the experts discuss polycystic ovary syndrome. J Womens Health Gend Based Med 2002; 11 (7): 579-84. 39. Palomba S, Falbo A, Giallauria F, et al. Effects of metformin with or without supplementation with folate on homocysteine levels and vascular endothelium of women with polycystic ovary syndrome. Diabetes Care 2010; 33 (2): 246-51. 40. Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346 (6): 393-403.
Capsule Aspirin helps to control metabolism, polarity, autophagy, and the restraint of cell proliferation
The protein kinase AMPK (adenosine monophosphateactivated protein kinase) directly monitors cellular energy stores as reected by changes in cellular concentrations of AMP, adenosine diphosphate (ADP), and adenosine triphosphate (ATP). Through phosphorylation of its targets, it helps to control metabolism, polarity, autophagy, and the restraint of cell proliferation. Activation of AMPK is also proposed to be benecial for the treatment of diseases, including cancer and diabetes. Hawley et al. report that AMPK can be activated by high concentrations of salicylate, a compound derived from the very commonly used drug aspirin. In mice, salicylate promoted fatty acid and carbohydrate metabolism in an AMPK-dependent fashion
Science 2012; 336: 918
Eitan Israeli
Capsule Cancer cells need more glycine
To better characterize metabolic properties of cancer cells, Jain et al. systematically measured the concentrations of hundreds of metabolites in cell culture medium in which 60 different cancer cell lines were growing. The fastest growing cancer cells tended to consume glycine, whereas more slowly growing cells excreted some glycine. The rapidly growing cancer cells appeared to need glycine for synthesis of purine nucleotides required for continued synthesis of DNA. Interfering with glycine metabolism slowed growth of the rapidly proliferating cancer cells. Thus, an increased dependence on glycine by rapidly growing cancer cells could potentially provide a target for therapeutic intervention.
Science 2012; 336: 1040
Eitan Israeli
447
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Lab Report 2Document12 pagesLab Report 2api-462451258Pas encore d'évaluation
- Abstract Book Leish World Congress 5Document1 116 pagesAbstract Book Leish World Congress 5libremdPas encore d'évaluation
- Skin Beauty InjectionsDocument12 pagesSkin Beauty Injectionst3kla100% (1)
- Aesthetic DermalDocument52 pagesAesthetic Dermalt3klaPas encore d'évaluation
- The Individualized Component Face Lift PRS March 2009 PDFDocument14 pagesThe Individualized Component Face Lift PRS March 2009 PDFt3klaPas encore d'évaluation
- Botox AdvancesDocument27 pagesBotox Advancest3kla100% (1)
- Adverse Effects of Fillers and TheirDocument16 pagesAdverse Effects of Fillers and Theirt3klaPas encore d'évaluation
- Walls Ancient Near EastDocument0 pageWalls Ancient Near Eastt3klaPas encore d'évaluation
- A Few Remarks Concerning The Clay Stamp Seals From The Gumelniţa CultureDocument17 pagesA Few Remarks Concerning The Clay Stamp Seals From The Gumelniţa Culturet3klaPas encore d'évaluation
- 00012Document11 pages00012t3klaPas encore d'évaluation
- Slavs AdriaticDocument0 pageSlavs Adriatict3klaPas encore d'évaluation
- (Daniel Foxvog) Introduction To Sumerian GrammarDocument170 pages(Daniel Foxvog) Introduction To Sumerian GrammarAshley WatsonPas encore d'évaluation
- N.N. Tasić - Neolitska Kvadratura KrugaDocument193 pagesN.N. Tasić - Neolitska Kvadratura Krugat3kla100% (5)
- Herrero-About The Distribution of Metal Objects in Prepalatial CreteDocument23 pagesHerrero-About The Distribution of Metal Objects in Prepalatial Cretet3klaPas encore d'évaluation
- Signal TransductionDocument33 pagesSignal TransductiongilmeanualexmihaiPas encore d'évaluation
- 004 Sensors and EffectorsDocument96 pages004 Sensors and EffectorsstarykPas encore d'évaluation
- Potential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334Document6 pagesPotential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334DicksonPas encore d'évaluation
- Seminar IDocument43 pagesSeminar Ikasahun AmarePas encore d'évaluation
- Bilirubin Toxicity: January 2012Document31 pagesBilirubin Toxicity: January 2012Muhammad HabiburrahmanPas encore d'évaluation
- Tissue Renewal, Regeneration and RepairDocument50 pagesTissue Renewal, Regeneration and RepairNurul AfiahPas encore d'évaluation
- E CadherinDocument8 pagesE Cadherinprism1702Pas encore d'évaluation
- Rapid Actions of Steroid Receptors in Cellular Signaling PathwaysDocument12 pagesRapid Actions of Steroid Receptors in Cellular Signaling PathwaysJulio SantanaPas encore d'évaluation
- Long COVID A Cytokine-Based Model For The Pathophysiology oDocument47 pagesLong COVID A Cytokine-Based Model For The Pathophysiology oIchlasul MadriddistaPas encore d'évaluation
- MAPK Signaling PathwayDocument2 pagesMAPK Signaling PathwaysgybleePas encore d'évaluation
- The Mechanisms of Muscle Hypertrophy and Their.40Document16 pagesThe Mechanisms of Muscle Hypertrophy and Their.40Sebastián EscuderoPas encore d'évaluation
- Signal Transduction in Prokaryotes and Eukaryotes-FinalDocument66 pagesSignal Transduction in Prokaryotes and Eukaryotes-FinalAsif gill0% (1)
- Genomic Analysis of MAP Kinase Cascades In: Arabidopsis Defense ResponsesDocument13 pagesGenomic Analysis of MAP Kinase Cascades In: Arabidopsis Defense ResponsesMelvin PrasadPas encore d'évaluation
- Structure Activity Relationships of Phenylalkylamines As Agonist Ligands For 5 HT2ADocument11 pagesStructure Activity Relationships of Phenylalkylamines As Agonist Ligands For 5 HT2ALUCAS OYANEDERPas encore d'évaluation
- Biochemistry and Biophysics Reports: Ayman M. El-Makakey, Radwa M. El-Sharaby, Mohammed H. Hassan, Alaa BalbaaDocument6 pagesBiochemistry and Biophysics Reports: Ayman M. El-Makakey, Radwa M. El-Sharaby, Mohammed H. Hassan, Alaa BalbaanepretipPas encore d'évaluation
- Immunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewDocument8 pagesImmunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewAlonso Ornelas GonzalezPas encore d'évaluation
- British Journal of Nutrition (2008), 99, E-Suppl.Document50 pagesBritish Journal of Nutrition (2008), 99, E-Suppl.nihadtoussounPas encore d'évaluation
- ATEROESCLEROSISDocument228 pagesATEROESCLEROSISTenazPas encore d'évaluation
- BS327 Module Handbook 2021-22Document8 pagesBS327 Module Handbook 2021-22Lois AlexanderPas encore d'évaluation
- (RSC Drug Discovery Series, 26) Jeremy I Levin - Stefan Laufer - Anti-Inflammatory Drug Discovery (2012, Royal Society of Chemistry)Document545 pages(RSC Drug Discovery Series, 26) Jeremy I Levin - Stefan Laufer - Anti-Inflammatory Drug Discovery (2012, Royal Society of Chemistry)Cosmina GeorgianaPas encore d'évaluation
- Melanin SynthesisDocument6 pagesMelanin SynthesisAlaa KubiasyPas encore d'évaluation
- TANTUM VERDE Benzydamin PDFDocument32 pagesTANTUM VERDE Benzydamin PDFAri KurniasariPas encore d'évaluation
- Protein Kinase Inhibition By: - 3 Fatty AcidsDocument9 pagesProtein Kinase Inhibition By: - 3 Fatty AcidsStepss StepsPas encore d'évaluation
- The Mechanisms of Muscle Hypertrophy SchoenfeldDocument26 pagesThe Mechanisms of Muscle Hypertrophy SchoenfeldFloren Martil Guijarro100% (1)
- Advanced Glycation End Products (AGEs) and Other Adducts in Aging-Related Diseases and Alcohol-Mediated Tissue InjuryDocument21 pagesAdvanced Glycation End Products (AGEs) and Other Adducts in Aging-Related Diseases and Alcohol-Mediated Tissue Injurysorin.morosan64Pas encore d'évaluation
- ArticoleDocument9 pagesArticolealinavsPas encore d'évaluation
- Osteocrin Ameliorates Adriamycin Nephropathy Via p38 Mitogen-Activated Protein Kinase InhibitionDocument15 pagesOsteocrin Ameliorates Adriamycin Nephropathy Via p38 Mitogen-Activated Protein Kinase InhibitionRuth Esperanza RodriguezPas encore d'évaluation
- The Key Role of Uric Acid inDocument10 pagesThe Key Role of Uric Acid intinatobingPas encore d'évaluation