Vous aimerez peut-être aussi
- NCLEX Questions - OB MATERNITY QUESTIONS PDFDocument17 pagesNCLEX Questions - OB MATERNITY QUESTIONS PDFAnneRaquelTalentoPas encore d'évaluation
- Flexor Tendon Protocols Ortheon MedDocument10 pagesFlexor Tendon Protocols Ortheon MedAzmi FarhadiPas encore d'évaluation
- Jin Gui Yao Lue Acupuncture PDFDocument2 pagesJin Gui Yao Lue Acupuncture PDFJiayiPas encore d'évaluation
- Postterm Pregnancy - UpToDateDocument16 pagesPostterm Pregnancy - UpToDateCarlos Jeiner Díaz SilvaPas encore d'évaluation
- Gravidity and Parity Definitions (Implications in Risk AssessmenDocument8 pagesGravidity and Parity Definitions (Implications in Risk AssessmenAbebe TadessePas encore d'évaluation
- Gravidity and Parity DefinitionsDocument3 pagesGravidity and Parity DefinitionsNur Fa'iqPas encore d'évaluation
- Del 153Document6 pagesDel 153Fan AccountPas encore d'évaluation
- Highrisk AssessmentDocument23 pagesHighrisk AssessmentHaripriya RadhikaPas encore d'évaluation
- SEMINAR On - Doc High RiskDocument21 pagesSEMINAR On - Doc High RiskDivya Grace100% (3)
- Obstetrics 2Document6 pagesObstetrics 2najmulPas encore d'évaluation
- Constitutional Macrosomia - A Case ReportDocument3 pagesConstitutional Macrosomia - A Case ReportIOSRjournalPas encore d'évaluation
- Postterm Pregnancy - UpToDateDocument17 pagesPostterm Pregnancy - UpToDateJosé Abraham Amaya DuartePas encore d'évaluation
- Edited Book 1Document501 pagesEdited Book 1mkm050923Pas encore d'évaluation
- Frequency of Preterm Labor and Its Factors in Patients Presenting To Secondary Care HospitalDocument6 pagesFrequency of Preterm Labor and Its Factors in Patients Presenting To Secondary Care HospitalJohn WickPas encore d'évaluation
- Multiple Pregnancy: OurceDocument7 pagesMultiple Pregnancy: OurceFamilia CieletPas encore d'évaluation
- Antenatal Assessment of Foetal Wellbeing.Document30 pagesAntenatal Assessment of Foetal Wellbeing.Kavya S MohanPas encore d'évaluation
- 2016 June Case StudyDocument8 pages2016 June Case StudyMarius Clifford BilledoPas encore d'évaluation
- Ultrasound in Obstet Gyne - 2013 - Khalil - Maternal Age and Adverse Pregnancy Outcome A Cohort StudyDocument10 pagesUltrasound in Obstet Gyne - 2013 - Khalil - Maternal Age and Adverse Pregnancy Outcome A Cohort StudyrimzeenafeeshaPas encore d'évaluation
- 10-Manejo de RPMDocument11 pages10-Manejo de RPMMelissa Garcia SandovalPas encore d'évaluation
- A Timely BirthDocument8 pagesA Timely BirthElmi MahlidaPas encore d'évaluation
- Bjo 12752Document9 pagesBjo 12752Topan AzzuriniPas encore d'évaluation
- Impact of Preeclampsia and Gestational Hypertension On Birth Weight by Gestational AgeDocument7 pagesImpact of Preeclampsia and Gestational Hypertension On Birth Weight by Gestational AgegeraldersPas encore d'évaluation
- Caesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort StudyDocument9 pagesCaesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort Studyluis albenis mendoza guerraPas encore d'évaluation
- DownloadDocument6 pagesDownloadKai GgPas encore d'évaluation
- Maternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018Document27 pagesMaternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018trongnguyen2232000Pas encore d'évaluation
- Elective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsDocument16 pagesElective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsErliana Damayanti100% (1)
- Case #1 SummaryDocument10 pagesCase #1 Summarygermanfutbol7100% (1)
- Teenage PregnancyDocument9 pagesTeenage PregnancyRexelle RamosPas encore d'évaluation
- App Acog 2012Document10 pagesApp Acog 2012jimedureyPas encore d'évaluation
- Clinical Case 4-PGI MendezDocument5 pagesClinical Case 4-PGI MendezJoher MendezPas encore d'évaluation
- Articulo 5Document6 pagesArticulo 5Monica ReyesPas encore d'évaluation
- Short Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationDocument6 pagesShort Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationManangioma ManPas encore d'évaluation
- Hadlock Ultrassonography in Obstetrics and Gynecology Cap 9 1994Document16 pagesHadlock Ultrassonography in Obstetrics and Gynecology Cap 9 1994Antonio Alfim Malanchini RibeiroPas encore d'évaluation
- Causes of Fetal DeathDocument3 pagesCauses of Fetal DeathRene Cordova InapanPas encore d'évaluation
- Epidemiology of Premature Rupture of Membranes: Factors in Pre-Term BirthsDocument11 pagesEpidemiology of Premature Rupture of Membranes: Factors in Pre-Term BirthsMaulidianaIndahPas encore d'évaluation
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 pagesExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJEPas encore d'évaluation
- Research ArticleDocument6 pagesResearch ArticleayubahriPas encore d'évaluation
- Impact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboDocument8 pagesImpact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboPramatama AndhikaPas encore d'évaluation
- Bjo0118 0578 PDFDocument11 pagesBjo0118 0578 PDFwe sagara dewiPas encore d'évaluation
- Safe Prevention of The Primary Cesarean Delivery - ACOGDocument16 pagesSafe Prevention of The Primary Cesarean Delivery - ACOGAryaPas encore d'évaluation
- Fetal DistressDocument5 pagesFetal DistressRonnie Portillo Cruz100% (1)
- O&GSpring2011 McDonnellDocument3 pagesO&GSpring2011 McDonnellmerizPas encore d'évaluation
- Case Write UpDocument5 pagesCase Write UpAisyah Hamdan100% (1)
- Konstantopoulos 2020Document14 pagesKonstantopoulos 2020Corey WoodsPas encore d'évaluation
- Maternal Obesity, Length of Gestation, Risk of Postdates Pregnancy and Spontaneous Onset of Labour at TermDocument6 pagesMaternal Obesity, Length of Gestation, Risk of Postdates Pregnancy and Spontaneous Onset of Labour at TermEdita Janet Yupanqui FlorianoPas encore d'évaluation
- ProblemDocument5 pagesProblemPrasad HewawasamPas encore d'évaluation
- Chorioamnionitis and Prognosis For Term Infants-13Document5 pagesChorioamnionitis and Prognosis For Term Infants-13ronny29Pas encore d'évaluation
- The Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyDocument3 pagesThe Correlation Between The Number of Vaginal Examinations During Active Labor and Febrile Morbidity, A Retrospective Cohort StudyKyla VillafrancaPas encore d'évaluation
- Vol93 No.6 661 5058Document6 pagesVol93 No.6 661 5058Titi Afrida SariPas encore d'évaluation
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDocument12 pagesCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalPas encore d'évaluation
- El Intervalo Intergenésico: Un Factor de Riesgo para Complicaciones Obstétricas y NeonatalesDocument5 pagesEl Intervalo Intergenésico: Un Factor de Riesgo para Complicaciones Obstétricas y NeonatalesFelix FernandezPas encore d'évaluation
- Frederiksen 2018Document7 pagesFrederiksen 2018WinniaTanelyPas encore d'évaluation
- 37004-Article Text-130842-2-10-20180629Document5 pages37004-Article Text-130842-2-10-20180629nishita biswasPas encore d'évaluation
- Herrera 2017Document9 pagesHerrera 2017Bianca Maria PricopPas encore d'évaluation
- Prenatal Care by Connie Sussan AustenDocument31 pagesPrenatal Care by Connie Sussan AustenNoraPas encore d'évaluation
- Acta Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsDocument5 pagesActa Obstet Gynecol Scand - 2011 - STJERNHOLM - Changed Indications For Cesarean SectionsAli QuwarahPas encore d'évaluation
- 2015 Sep Embarazo Múltiple - Vía Del Parto.Document13 pages2015 Sep Embarazo Múltiple - Vía Del Parto.Alexander Gonzalez BarturenPas encore d'évaluation
- Previous Abortions and Risk of Pre-Eclampsia: Reproductive HealthDocument8 pagesPrevious Abortions and Risk of Pre-Eclampsia: Reproductive HealthelvanPas encore d'évaluation
- Module 5 Induction and Augmentation of LaborDocument17 pagesModule 5 Induction and Augmentation of LaborZyrene RiveraPas encore d'évaluation
- Data Mining Approach in Preterm Birth Prediction: Jyothi ThomasDocument13 pagesData Mining Approach in Preterm Birth Prediction: Jyothi ThomasAnonymous Fs8SOuPas encore d'évaluation
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoPas encore d'évaluation
- Jurnal 10 PDFDocument8 pagesJurnal 10 PDFFirman MufidPas encore d'évaluation
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsD'EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsPas encore d'évaluation
- Hypothyroidism - in The ClinicDocument17 pagesHypothyroidism - in The ClinicCarlos PerezPas encore d'évaluation
- MED - en USDocument1 735 pagesMED - en USAndre GarciaPas encore d'évaluation
- Definiendio Enfermedad Renal Aguda 2021 NephronDocument4 pagesDefiniendio Enfermedad Renal Aguda 2021 NephronGabino Alexander Liviac CrisostomoPas encore d'évaluation
- Wikipedia Handbook of Biomedical InformaticsDocument802 pagesWikipedia Handbook of Biomedical InformaticsAndre Garcia100% (1)
- 2 RecordsDocument6 pages2 RecordsAndre GarciaPas encore d'évaluation
- Cvid Lancet 2008Document14 pagesCvid Lancet 2008Andre GarciaPas encore d'évaluation
- Serologic Testing in Connective Tissue DiseasesDocument4 pagesSerologic Testing in Connective Tissue DiseasesAndre GarciaPas encore d'évaluation
- Connective Tissue DZDocument1 pageConnective Tissue DZAndre GarciaPas encore d'évaluation
- Medical AbbreviationsDocument48 pagesMedical AbbreviationsVirginia Po100% (4)
- Rating Criteria: Prior To Woman'S Transfer To The DRDocument3 pagesRating Criteria: Prior To Woman'S Transfer To The DRPatricia Ann JaringPas encore d'évaluation
- Chapter 006Document42 pagesChapter 006api-263755297Pas encore d'évaluation
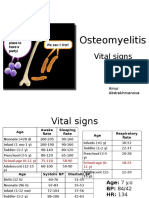
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaPas encore d'évaluation
- NW Centenary Pub PDFDocument28 pagesNW Centenary Pub PDFRazaCreciaLastrillaMenesesPas encore d'évaluation
- Rop Job Application With Availability Fillable For WebsiteDocument2 pagesRop Job Application With Availability Fillable For Websiteapi-315685418Pas encore d'évaluation
- EAU Guidelines On Urological Infections 2021Document74 pagesEAU Guidelines On Urological Infections 2021ioana teodorescuPas encore d'évaluation
- CME Examination DermatologyDocument25 pagesCME Examination DermatologylimeddyPas encore d'évaluation
- Tugas English of NursingDocument3 pagesTugas English of NursingSyahlu DamayantiiPas encore d'évaluation
- 0Document2 pages0cesar del rosarioPas encore d'évaluation
- GynegologicalDocument1 pageGynegologicaltristan_adviento32Pas encore d'évaluation
- General Anaesthesia: Adityadeb Ghosh B. Pharm Guru Nanak Institute of Pharmaceutical Science and Technology, Kolkata, INDocument19 pagesGeneral Anaesthesia: Adityadeb Ghosh B. Pharm Guru Nanak Institute of Pharmaceutical Science and Technology, Kolkata, INSunetraPas encore d'évaluation
- Full Download Leadership Roles and Management Functions in Nursing Theory and Application Marquis 8th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Leadership Roles and Management Functions in Nursing Theory and Application Marquis 8th Edition Test Bank PDF Full Chaptermichaelcollinsxmsfpytneg100% (19)
- Acupressure On Self-Reported Sleep Quality During Pregnancy: Journal of Acupuncture and Meridian StudiesDocument5 pagesAcupressure On Self-Reported Sleep Quality During Pregnancy: Journal of Acupuncture and Meridian StudiesSofia SagitaPas encore d'évaluation
- Journal SURGERY 2018Document3 pagesJournal SURGERY 2018Kit LaraPas encore d'évaluation
- Amy Dhillon Levine, DPM: Education & TrainingDocument3 pagesAmy Dhillon Levine, DPM: Education & TrainingapnipatPas encore d'évaluation
- Obstetric Coding Quality Error Trends - IPDocument36 pagesObstetric Coding Quality Error Trends - IPRavi NunavathPas encore d'évaluation
- PacuDocument93 pagesPacunorhafizahstoh89Pas encore d'évaluation
- NauseaDocument12 pagesNauseakazakom100% (2)
- The Open Ophthalmology JournalDocument5 pagesThe Open Ophthalmology JournalFenny Duma SariPas encore d'évaluation
- Postpartum HemorrhageDocument9 pagesPostpartum HemorrhageSilvya L. MandeyPas encore d'évaluation
- Fluid & Electrolytes Management (Nabil)Document78 pagesFluid & Electrolytes Management (Nabil)Ahmad Nabil Md RosliPas encore d'évaluation
- Space Requirements For 3 Major StructuresDocument13 pagesSpace Requirements For 3 Major StructuresKyle Darren CawalingPas encore d'évaluation
- HERNIORRHAPHYDocument2 pagesHERNIORRHAPHYSheldon Deypalubos Jr.Pas encore d'évaluation
- Carcinoma of The Breast: Nur ZulaikhaDocument12 pagesCarcinoma of The Breast: Nur ZulaikhaCahaya Al-HazeenillahPas encore d'évaluation
- Morgan Mikhails Clinical Anesthesiology 6Th Edition Edition John F Butterworth Full ChapterDocument67 pagesMorgan Mikhails Clinical Anesthesiology 6Th Edition Edition John F Butterworth Full Chaptermatthew.westerman975100% (12)
- MyLabSigma 160000165MA Ver. 03Document8 pagesMyLabSigma 160000165MA Ver. 03Waaiz AhmedPas encore d'évaluation