Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- HydrotubationDocument4 pagesHydrotubationAna Di Jaya100% (1)
- Cotrimoxazole Profilaxis Hiv Who Guidlines PDFDocument68 pagesCotrimoxazole Profilaxis Hiv Who Guidlines PDFAna Di JayaPas encore d'évaluation
- 75178347Document5 pages75178347Ana Di JayaPas encore d'évaluation
- Renu GargDocument3 pagesRenu GargAna Di JayaPas encore d'évaluation
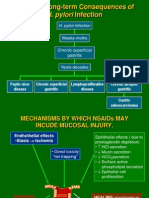
- 2 Pathogenesis TukakLambungDocument30 pages2 Pathogenesis TukakLambungAna Di JayaPas encore d'évaluation
- Hypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryDocument4 pagesHypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryAna Di JayaPas encore d'évaluation
- Journal of Medical Case ReportsDocument4 pagesJournal of Medical Case ReportsAna Di JayaPas encore d'évaluation
- HydrotubationDocument4 pagesHydrotubationAna Di Jaya100% (1)
- Leiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaDocument5 pagesLeiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaAna Di JayaPas encore d'évaluation
- Pengobatan Pada Tiap KomplikasiDocument6 pagesPengobatan Pada Tiap KomplikasiAna Di JayaPas encore d'évaluation
- A Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumDocument4 pagesA Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumAna Di JayaPas encore d'évaluation
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolPas encore d'évaluation
- Case Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaDocument4 pagesCase Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaAna Di JayaPas encore d'évaluation
- Efficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialDocument5 pagesEfficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialAna Di JayaPas encore d'évaluation
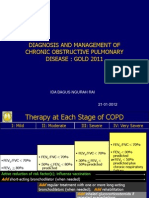
- Rountable Copd Jan 2012Document71 pagesRountable Copd Jan 2012Ana Di JayaPas encore d'évaluation
- Who Guidlines Pregnancy Woman 2010 PDFDocument117 pagesWho Guidlines Pregnancy Woman 2010 PDFAna Di JayaPas encore d'évaluation
- Case of A Woman With Cough and Lung Nodule PDFDocument9 pagesCase of A Woman With Cough and Lung Nodule PDFAna Di JayaPas encore d'évaluation
- Vol361and2topic04 PDFDocument6 pagesVol361and2topic04 PDFAna Di JayaPas encore d'évaluation
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDocument8 pagesCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaPas encore d'évaluation
- Case of A Woman With Obesity, DM An Hypertension PDFDocument10 pagesCase of A Woman With Obesity, DM An Hypertension PDFAna Di JayaPas encore d'évaluation
- The Early Prevention of Stroke Heart Attack Perki SMG 05Document38 pagesThe Early Prevention of Stroke Heart Attack Perki SMG 05Ana Di JayaPas encore d'évaluation
- Case of A Womenwith Acute Onset of Chest Pain PDFDocument9 pagesCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaPas encore d'évaluation
- Case of A Womenwith Acute Onset of Chest Pain PDFDocument9 pagesCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaPas encore d'évaluation
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDocument8 pagesCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaPas encore d'évaluation
- Case of Bladder Carcinoma PDFDocument9 pagesCase of Bladder Carcinoma PDFAna Di JayaPas encore d'évaluation
- Case of Impaired Renal Funtion PDFDocument1 pageCase of Impaired Renal Funtion PDFAna Di JayaPas encore d'évaluation
- Case of Boy With Slowing Growth, Delayed Puberty PDFDocument11 pagesCase of Boy With Slowing Growth, Delayed Puberty PDFAna Di JayaPas encore d'évaluation
- Case Report .Hepatic Failure PDFDocument4 pagesCase Report .Hepatic Failure PDFAna Di JayaPas encore d'évaluation
- Case of Bladder Carcinoma PDFDocument9 pagesCase of Bladder Carcinoma PDFAna Di JayaPas encore d'évaluation
- Fever With HemiplegiaDocument65 pagesFever With HemiplegiaMohit JainPas encore d'évaluation
- Diagnosis and Treatment of Viral Encephalitis: ReviewDocument10 pagesDiagnosis and Treatment of Viral Encephalitis: ReviewnataliaPas encore d'évaluation
- Chapter 32 - Viral Infections of The Nervous System and Prion DiseasesDocument46 pagesChapter 32 - Viral Infections of The Nervous System and Prion DiseasesUmar IslamiPas encore d'évaluation
- Asfa 2013Document140 pagesAsfa 2013bib22Pas encore d'évaluation
- UpToDate 2021 Overview of Cerebellar Ataxia in AdultsDocument55 pagesUpToDate 2021 Overview of Cerebellar Ataxia in AdultsPaloma GBPas encore d'évaluation
- 6M Case Report Postinfectious CerebellitisDocument14 pages6M Case Report Postinfectious CerebellitisGa B B OrlonganPas encore d'évaluation
- Newsletter v5n2Document92 pagesNewsletter v5n2Transverse Myelitis AssociationPas encore d'évaluation
- Acute Disseminated EncephalitisDocument16 pagesAcute Disseminated EncephalitisDedy SavradinataPas encore d'évaluation
- 1.international Concerns Regarding Gardasil and CervarixDocument38 pages1.international Concerns Regarding Gardasil and Cervarixjeff.aufderheide2634Pas encore d'évaluation
- EncephalitisDocument27 pagesEncephalitisHasRoni Fathurrahman100% (1)
- Internal Medicine II - NEUROLOGY CASESDocument33 pagesInternal Medicine II - NEUROLOGY CASESAhmad SobihPas encore d'évaluation
- Pathology of CNS: Eric M. Mirandilla MD, DPSPDocument71 pagesPathology of CNS: Eric M. Mirandilla MD, DPSPDhruva PatelPas encore d'évaluation
- Anatomy and Pathology of the Cerebellar PeduncleDocument9 pagesAnatomy and Pathology of the Cerebellar PeduncleJulius Dominique L. AnjaoPas encore d'évaluation
- MOG Antibody-Associated DiseasesDocument3 pagesMOG Antibody-Associated DiseasesYassmin ElNazerPas encore d'évaluation
- Quality of Life of Children and Adolescents With Multiple SclerosisDocument16 pagesQuality of Life of Children and Adolescents With Multiple SclerosisHPdHPas encore d'évaluation
- Acute Hemorrhagic Leukoencephalitis Hurst Disease Secondary To h1n1 in A Child A Story of Full Recovery From QatarDocument4 pagesAcute Hemorrhagic Leukoencephalitis Hurst Disease Secondary To h1n1 in A Child A Story of Full Recovery From Qataremilia candraPas encore d'évaluation
- Professor Yasser Metwally: Clinical PictureDocument14 pagesProfessor Yasser Metwally: Clinical PictureSabrin BadarnePas encore d'évaluation
- CNS Notes: By: Dr. Abdullah NouhDocument40 pagesCNS Notes: By: Dr. Abdullah NouhHythem HashimPas encore d'évaluation
- CP - Acute Onset ParaparesisDocument47 pagesCP - Acute Onset ParaparesisParag DashatwarPas encore d'évaluation
- Neuromyelitis Optica Spectrum Disorders - UpToDateDocument28 pagesNeuromyelitis Optica Spectrum Disorders - UpToDateRoxana StanciuPas encore d'évaluation
- Acquired Demyelinating SyndromesDocument13 pagesAcquired Demyelinating SyndromesfbonillaPas encore d'évaluation
- 107 Studies On VaccineDocument65 pages107 Studies On VaccineiRepair Gold Coast100% (1)
- Wasp StingDocument3 pagesWasp StingShruthi KyPas encore d'évaluation
- Acute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportDocument4 pagesAcute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportIJAR JOURNALPas encore d'évaluation
- Transverse Myelitis Pathogenesis, Diagnosis and Treatment PDFDocument17 pagesTransverse Myelitis Pathogenesis, Diagnosis and Treatment PDFIndira DeviPas encore d'évaluation
- Demyelinating DiseasesDocument76 pagesDemyelinating Diseasesapi-3743483100% (1)
- Pediatric Demyelinating Diseases of The Central Nervous System and Their MimicsDocument338 pagesPediatric Demyelinating Diseases of The Central Nervous System and Their MimicsVu Hoang100% (1)
- A Case Report of Obsessive-Compulsive DisorderDocument6 pagesA Case Report of Obsessive-Compulsive DisorderfonsoalPas encore d'évaluation
- Ivig Neurology GuidelineDocument74 pagesIvig Neurology GuidelineAnjilina NicePas encore d'évaluation
- Transverse MyelitisDocument10 pagesTransverse MyelitisEmily EresumaPas encore d'évaluation