Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Sertifikat Seminar ABK BaiturahmahDocument1 pageSertifikat Seminar ABK BaiturahmahRizka Dwi Nur VitriaPas encore d'évaluation
- 989-511-02 (Polyclav)Document12 pages989-511-02 (Polyclav)Rizka Dwi Nur VitriaPas encore d'évaluation
- Ken Adn Sny MRZ Ing Saw Dys Sel Tam DWR San Cha MRZ Sny Saw Ing Adn Ken DWR Tam Cha San Sel Dys Ing Saw Ken Adn Sny MRZ San Cha Dys Sel Tam DWRDocument2 pagesKen Adn Sny MRZ Ing Saw Dys Sel Tam DWR San Cha MRZ Sny Saw Ing Adn Ken DWR Tam Cha San Sel Dys Ing Saw Ken Adn Sny MRZ San Cha Dys Sel Tam DWRRizka Dwi Nur VitriaPas encore d'évaluation
- Attachments For OverdenturesDocument88 pagesAttachments For OverdenturesRizka Dwi Nur VitriaPas encore d'évaluation
- Changes in Physical and Chemical Properties During The Production of Palm Sugar Syrup by Open Pan and Vacuum Evaporator PDFDocument9 pagesChanges in Physical and Chemical Properties During The Production of Palm Sugar Syrup by Open Pan and Vacuum Evaporator PDFRizka Dwi Nur VitriaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Conversion Disorder NotesDocument6 pagesConversion Disorder NotesFariha Zulfiqar AliPas encore d'évaluation
- Adhd PaperDocument3 pagesAdhd Paperapi-508146359Pas encore d'évaluation
- Neuromedicine Applications in US Warfare and Governance of The General Public PDFDocument14 pagesNeuromedicine Applications in US Warfare and Governance of The General Public PDFDarcy Keverian100% (1)
- Behaviorist PerspectiveDocument32 pagesBehaviorist Perspectivecarl diannePas encore d'évaluation
- Breathing To Treat Vagus NerveDocument13 pagesBreathing To Treat Vagus NerveImad Mukahhal100% (7)
- 03 2019 Amigdala e Área PrefrontalDocument23 pages03 2019 Amigdala e Área PrefrontalVitor JuniorPas encore d'évaluation
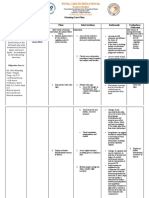
- Nursing Care Plan: by The Wife During InterviewDocument3 pagesNursing Care Plan: by The Wife During InterviewJayson SamontePas encore d'évaluation
- Otorrino ContinuumDocument220 pagesOtorrino ContinuumRafaelPas encore d'évaluation
- The Challenges and Stigma of Living With Antisocial Personality DisorderDocument5 pagesThe Challenges and Stigma of Living With Antisocial Personality DisorderVica ClaeysPas encore d'évaluation
- Efficacy of Erandamuladi Niruhabasti in Gridhasi A Case StudyDocument4 pagesEfficacy of Erandamuladi Niruhabasti in Gridhasi A Case StudyResearch ParkPas encore d'évaluation
- QOL Neck PainDocument16 pagesQOL Neck PainInstrukcije SeminariPas encore d'évaluation
- True False Not Given Practice Test PDFDocument3 pagesTrue False Not Given Practice Test PDFNgan TracKimPas encore d'évaluation
- ParkinsonDocument3 pagesParkinsonRJean TumalaPas encore d'évaluation
- Dichotic TestDocument91 pagesDichotic TestKUNNAMPALLIL GEJO JOHN0% (1)
- Understanding Bimotor AbilitiesDocument68 pagesUnderstanding Bimotor Abilitiesrce.ta453407Pas encore d'évaluation
- Introduction To Brain Anatomy: Wieslaw L. NowinskiDocument37 pagesIntroduction To Brain Anatomy: Wieslaw L. NowinskiAditya Rama DevaraPas encore d'évaluation
- Basavaraj-Colour Therapy PDFDocument144 pagesBasavaraj-Colour Therapy PDFTanuku Net86% (14)
- McKenzie LumbarDocument51 pagesMcKenzie LumbarRouqia HamedPas encore d'évaluation
- Artificial VisionDocument7 pagesArtificial Visionmahi07404Pas encore d'évaluation
- Craniotomy: Memdova, Monette A. Bsn-3B Llevado, Emielou A. Bsn-3BDocument26 pagesCraniotomy: Memdova, Monette A. Bsn-3B Llevado, Emielou A. Bsn-3BMonette Abalos MendovaPas encore d'évaluation
- Ophthal - OSCE Part 2Document24 pagesOphthal - OSCE Part 2Pitty Prarthana100% (1)
- Neurology. 58 (5) : 688-97 Review and Meta-Analysis". Stroke. 47 (5) : 1253-7Document2 pagesNeurology. 58 (5) : 688-97 Review and Meta-Analysis". Stroke. 47 (5) : 1253-7Marius FlaminzianuPas encore d'évaluation
- Study Questions Special SensesDocument37 pagesStudy Questions Special SensesSurajit Bhattacharjee93% (14)
- NCP SchizophreniaDocument7 pagesNCP SchizophreniaSteffi Raye Madrid50% (2)
- Feeding/Eating and Sleep-Wake Disorders: Alyson Morgan, MS3 Ross University School of MedicineDocument14 pagesFeeding/Eating and Sleep-Wake Disorders: Alyson Morgan, MS3 Ross University School of MedicineAly MorganPas encore d'évaluation
- Med Surg NervesDocument3 pagesMed Surg NervesZachary T HallPas encore d'évaluation
- Pre Gabal in Drug StudyDocument1 pagePre Gabal in Drug StudyHailMarieSBarcenasPas encore d'évaluation
- Presented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDocument78 pagesPresented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDorin PathakPas encore d'évaluation
- Amygdala Retraining JHH Sept 2010Document40 pagesAmygdala Retraining JHH Sept 2010OmmachinePas encore d'évaluation
- Pulsed Magnetic Therapy For Depression Pulsed Electromagnetic Field Therapy (PEMF / RTMS)Document22 pagesPulsed Magnetic Therapy For Depression Pulsed Electromagnetic Field Therapy (PEMF / RTMS)edcanalPas encore d'évaluation