Académique Documents
Professionnel Documents
Culture Documents
Diastolic Function
Transféré par
Krishna RathodCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Diastolic Function
Transféré par
Krishna RathodDroits d'auteur :
Formats disponibles
Chapter
Diastolic function: physiology, methods and clinical significance
Background of the present thesis
rom a physiological point of view the heart is an integrated muscle-pump system. The term diastole is interpreted as a division, notch, or separation between two contraction-relaxation cycles (Brutsaert 1984). In this interpretation its meaning is restricted to the passive properties of the heart (Gillebert 1994). Diastole of the left ventricle starts when active relaxation has been completed and includes the diastasis and the atrial contraction phase (Figure 2.1). In the English medical literature diastole has however come to mean "the dilatation or period of dilatation of the heart, especially that of the ventricles, coinciding with the interval between the second and first heart sounds" (Brutsaert 1984). In this interpretation it is that part of the cardiac cycle which starts with the isovolumetric relaxation phase and ends with cessation of mitral inflow (Arrighi 1995). In the present thesis the latter, clinical definition of diastole will be used. Ebstein extensively discusses the history of views on diastole in 1904 (Ebstein 1904). Mackenzie devides the heartcycle in a presphygmic period with rising ventricular pressure between closure of the atrio-ventricular valves and opening of the aortic valves, a sphygmic or pulse period with opened aortic valves, and a postsphygmic period after aortic valve closure and before atrio-ventricular valve opening where ventricular pressure is falling (Mackenzie 1914). Wiggers suddevided the cardiac cycle into smaller phases (Wiggers 1921). In his view, diastole is preceded by protodiastole, the period between end of ventricular contraction and closure of the semilunar valves. The period of diastole then begins with closure of the semilunar valves and isometric relaxation. After opening of the atrio-ventricular valves a period of diastolic inflow begins. In case of a sufficiently long diastolic interval a period of diastasis is recognised in addition. Wiggers subdevided the period of auricular systole in a period in which auricular contracction exerts effect on ventricular filling or ventricular tension, and a period of auricular filling by venous return from the pulmonary circulation (Wiggers 1921). In 1978 new interest arose on relaxation and diastole, since symptoms of cardiac disease could be succesfully related to pathophysiology of diastole (Meijler
Chapter 2
S
IC EJECTION IR RFP
SUCTION
D
DIASTASIS
PASSIVE FILLING
CLINICAL DEFINITION
ATRIAL CONT R
MUSCLEPUMP
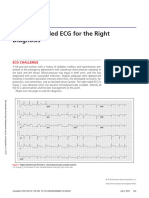
FIGURE 2.1. Definition of diastole according to the analogy between isolated cardiac muscle and intact left ventricular function. Time traces of force (f) and length (l) of an afterloaded twitch with physiologic relaxation sequence are synchronized with left ventricular pressure (P) and volume (V). In one heart cycle systole (S) and diastole (D) alternate. Systole is the period of contraction and relaxation. Diastole is the period between two contraction-relaxation cycles (Gillebert 1994). In the clinical definition diastole starts with the isovolumetric relaxation (IR) phase, includes the rapid filling phase (RFP), the period of diastasis, and the atrial contraction phase, and ends before the isovolumetric contraction (IC) phase, (Brutsaert 1984).
and Brutsaert 1978). Heart failure can be defined as "the pathophysiological state in which an abnormality of cardiac function is responsible for failure of the heart to pump blood at a rate commensurate with the requirements of the metabolising tissues, or to do so only from an elevated filling pressure" (Braunwald 1992). As a consequence, in diastolic failure increased resistance to ventricular filling leads to elevated ventricular filling pressures or inadequate cardiac output. Accordingly, an increase in pulmonary wedge pressure may lead to symptoms of congestion. It is clear that within this definition many cardiac diseases may result eventually in diastolic failure, including reduced systolic performance, pericardial and valvular disease (Table 2.1). The main causes of diastolic failure can be divided into relaxation abnormalities, decreased compliance and inappropriately high heart rates (Brutsaert 1993). All three causes can contribute separately to diastolic failure, but in many conditions they act together.
Diastolic function: focus on the present thesis
DIASTOLIC PHASES The four phases into which diastole is divided (isovolumic relaxation, rapid filling, diastasis and atrial systole) will be discussed briefly (Figure 2.1). Relaxation of the heart is a dynamic process of isovolumic relaxation and early rapid filling. Rapid filling still continues after relaxation has been completed. A relatively small volume portion is shifted into the left ventricle during diastasis. In the atrial contraction phase intraventricular blood volume increases again. Isovolumic relaxation. Relaxation is a catecholamine dependent energy consuming process in which large portions of adenosine triphosphate (ATP) are used. The dissociation of actin-myosin crossbridges results from an allosteric action of ATP, i.e. a reaction of ATP with a site at the myosin head other than the binding site of actin causing the actomyosin rigor complex to dissociate (Figueredo 1993, Apstein 1994). This process is called the "plasticising effect" of ATP. Further relaxation is assured by rapid resequestration of cytosolic calcium in the sarcoplasmic reticulum by sarcoplasmic reticulum calcium ATPase, which is activated by phosphorylation of phospholamban, a regulatory subunit of the calcium pump of the sarcoplasmic reticulum. The affinity of the calcium receptor site on the troponin-tropomyosin complex for calcium is decreased by phosphorylation, thereby increasing the rate of dissociation of calcium from troponin C and enhancing relaxation (Morgan 1991). This process of relaxation starts in late systole and ends in mid-diastole, causing the intraventricular pressure to decline (Brutsaert 1984). Left ventricular pressure first falls below the pressure in the aortic root, which causes the aortic valve to close. Pressure continues to decline until below left atrial pressure, so that the mitral valve will open, and rapid filling begins. The decline of pressure in time approximates an exponential curve, but in the non-filling heart the left ventricular pressure frequently reaches a negative asymptote due to elastic recoil (Yellin 1986, Yellin 1994). The rate of myocardial relaxation is influenced by several independent factors in the intact heart (Brutsaert 1980, Brutsaert 1984): (1) Pre- and afterload, (2) inactivation (which itself is influenced by neurohumoral factors, the coronary circulation, and the use of drugs), and (3) regional nonuniformity (of load and inactivation). Furthermore, impaired relaxation, whether incomplete or slow, must be discerned conceptually from prolonged systolic contraction, which is a physiologic and compensatory situation merely leading to delayed or retarded relaxation (Brutsaert 1993). In prolonged contraction, which can be seen in acute and chronic systolic pressure or volume loading, the early phase of hypertrophy and increased contractility, an upward shift of the diastolic part of the pressure-volume relation which is seen in impaired relaxation, is not observed.
Chapter 2
TABLE 2.1. Summary of conditions in which left ventricular diastolic dysfunction may be involved, their pathophysiology and mechanisms (Vasan 1996, Grossman 1991). Mechanism Hypertension relaxation Pathophysiology chamber compliance Coronary artery disease - Myocardial ischemia relaxation chamber compliance - Myocardial infarction relaxation chamber compliance Valvular heart disease - Aortic stenosis - Mitral stenosis - Aortic regurgitation relaxation chamber compliance relaxation chamber compliance - Mitral regurgitation Hypertrophic cardiomyopathy idem relaxation chamber compliance Restrictive cardiomyopathy chamber compliance Constrictive pericarditis Dilating cardiomyopathy end-diastolic chamber relaxation compliance pressure overload concentric hypertrophy resistance to atrial emptying / volume overload eccentric hypertrophy but decreased altered collagen matrix nonuniformity (regional variation in coronary reserve relaxation load contraction load (obstruction) myocardial compliance altered chamber geometry myocardial compliance (deposits, deposits (e.g. sarcoid) altered collagen matrix diastolic capacity diastolic calcium overload retarded inactivation altered collagen matrix end-diastolic volume retarded inactivation (diastolic calcium nonuniformity (regional variation in myocardial compliance (altered retarded inactivation contraction load nonuniformity (regional variation in regional fibrosis regional myocardial compliance afterload ( contraction load) nonuniformity (regional variation in coronary reserve myocardial compliance (fibrosis) altered chamber geometry coronary turgor
atrial ventricular pressure
idem
Diastolic function: focus on the present thesis
Rapid filling. When left ventricular pressure falls below left atrial pressure the mitral valve will open. The left ventricle will then be filled by the blood which is accumulated in the left atrium in the previous systole. The rate of early left ventricular filling is determined uniquely by the atrioventricular pressure gradient and the impedance of the mitral valve (Ishida 1986, Yellin 1990, Yellin 1992, Yellin 1994). The atrioventricular pressure difference, in turn, is determined by the active and passive properties (relaxation and compliance) of both left atrium and left ventricle. Thus, factors which determine these properties, like e.g. loading conditions, contractility, and heart rate influence the early diastolic filling pattern by means of their influence on the pressure difference. In experimental canine models in which the left ventricle was withheld from filling by end-systolic volume clamping, the left ventricular pressure frequently fell below zero (Yellin 1986, Sabbah 1981). This diastolic suction of the left ventricle is caused by the storage of potential energy generated by preceding systolic contraction to below the equilibrium volume, i.e. the volume that the left ventricle exhibits when there is no transmural pressure (Brecher 1966, Yellin 1994). In an experimental setting in dogs the degree of pressure negativity after volume clamping was increased when contractility was increased (Hori 1982). Evidence was provided by Udelson et al. that elastic recoil and restoring forces are also operative in the intact human heart during -adrenergic stimulation (Udelson 1990). When, in this experiment, end-systolic volume was further reduced below the equilibrium volume, minimal diastolic pressure was also reduced. This probably resulted from an augmentation of internal restoring forces and elastic recoil, which in turn may result in negative transmural pressure and diastolic suction. So, the fall in left ventricular pressure at the time of opening of the mitral valve is not only resulting from left ventricular relaxation, it is also caused by elastic recoil. The atrioventricular pressure gradient, the driving force of left ventricular filling, is also determined by left atrial pressure. In experiments by Ishida et al. increased left atrial pressures by volume loading of mongrel dogs resulted in increased peak rapid filling rates induced by increased atrioventricular pressure gradients, despite decreased rate of left ventricular relaxation induced by increased loading conditions (Ishida 1986). Left atrial compliance will also affect the peak atrioventricular pressure difference (Keren 1985, Suga 1974). In early diastolic filling, blood leaves the left atrium faster than it is filled by the pulmonary veins, and its pressure will fall (y-descent). At first, left ventricular pressure will continue to decline despite early left ventricular filling, thus accelerating blood into the left ventricle. With increasing left ventricular volume, left ventricular pressure will rise according to the passive filling characteristics, that are determined by viscoelastic properties of the myocardium, myocardial thickness, and external constraints, e.g. pericardium, right ventricle and lungs (Yellin 1990, Little 1990, Janicki 1990, Little 1995). Once relaxation and elastic recoil are completed, left ventricular filling will continue because of inertia, i.e. the mass of flowing blood (Yellin 1990). Early left ventricular filling rate, i.e. the first derivative of
10
Chapter 2
volume-versus-time curve, will diminish when atrioventricular pressure is reversed (Courtois 1988). This "deceleration" of rapid left ventricular filling is greatly determined by left ventricular chamber stiffness, so that early diastolic filling deceleration time decreases as left ventricular chamber stiffness increases (Little 1995). Conversely, early diastolic filling deceleration time may increase in the presence of mitral stenosis as a consequence of increased impedance of the mitral valve with prolonged atrioventricular pressure difference associated with elevated left atrial pressure (Meisner 1991). Diastasis. This stage of ventricular filling is generally addressed as being the phase of passive filling in which the filling rate is slow, the rise in ventricular pressure is moderate, and the pressures of the left atrium and ventricle have reached an equilibrium (Arrighi 1995). Some authors however observed a mid diastolic inflow peak into the left ventricle, arising from a reestablishment of a positive atrioventricular gradient due to left atrial filling via the pulmonary veins (Keren 1986, Yellin 1992, Biasucci 1990). Middiastolic inflow may contribute more than 20 % of total filling of the left ventricle in dogs, but is absent in the dilated heart and in mitral stenosis (Biasucci 1990, Yellin 1992). Atrial systole. The last phase of ventricular filling is dominated by the contraction of the atria, which causes atrial pressure to rise again above ventricular pressure and induce a new blood flow into the left ventricle. This phase is influenced by left atrial function, loading, and heart rate (Wang 1995 , Courtois 1994, Udelson 1994). Atrial dysrhythmia, hypertrophy, and dilatation may alter this phase considerably (Rowlands 1967, Bonow 1983a, Kono 1992). ASSESSMENT OF DIASTOLIC FUNCTION The generally applied non invasive methods to assess diastolic left ventricular function are radionuclide angiography (RNA), two-dimensional echocardiography and Doppler echocardiography. The principles of measuring diastolic function with RNA will be discussed below, whereas the methodology of the latter two techniques will be discussed only briefly. Cardiac catheterisation with ventriculography is an invasive method of assessing diastolic properties of the heart and will be discussed as well. The newer methods of assessing diastolic function, including 2-D colour Doppler, colour Mmode Doppler, and cardiac magnetic resonance imaging, will be mentioned but are not discussed because they are not (yet) used in routine clinical practice for the purpose of assessing diastolic left ventricular function. In all techniques, temporal resolution and filtering strongly influence measurements of left ventricular volume change rate. Cardiac catheterisation. With cardiac catheterisation it is possible to collect measures of left ventricular function invasively. When focusing on diastolic function, the parameters can be divided into those expressing (passive) compliance, and those
Diastolic function: focus on the present thesis
11
expressing (active) relaxation of the left ventricle (Gaasch 1994). Chamber compliance, the inverse of chamber stiffness can be defined as the instantaneous volume change per unit change in pressure (dV/dP) and can be calculated when measures of diastolic left ventricular volume and pressure have been gathered together (Grossman 1986, Van der Werf 1991). Relaxation can be described with help of the left ventricular pressure curve during isovolumic relaxation. The first derivative of this curve describes the rate of left ventricular pressure decline (dP/dt). Although relaxation can be described by peak dP/dt, this factor is influenced by changes in loading (Grossman 1986). A better parameter to describe left ventricular relaxation is obtained when the time constant of left ventricular pressure decline is calculated (Grossman 1986, Van der Werf 1991, Shintani 1994). In slow myocardial relaxation may be prolonged and vice versa. Radionuclide angiography. The assessment of global left ventricular diastolic function with radionuclide angiography is derived from the time activity curve of the left ventricle, which closely matches the left ventricular volume curve (Figure 2.2). It therefore represents relative volume changes throughout the cardiac cycle. This curve is also used for the assessment of global left ventricular ejection fraction. When appropriate data acquisition has taken place and attention has been paid to the technical considerations (see below) this volume curve may also be used to study left ventricular filling, which, as outlined before, is dependent on diastolic left ventricular function. Parameters of diastolic function include those expressing the filling rate at a certain moment (e.g. peak filling rate), the timing of this event (e.g. time to peak filling rate), and relative filling fractions (e.g. early diastolic filling fraction and atrial contribution to diastolic filling, Udelson 1994). In the interpretation of diastolic function parameters technical details as well as physiological variations (the dependency of left ventricular filling parameters on
FIGURE 2.2. Time-activity curve obtained from radionuclide angiography after temporal smoothing with 5 Fourier harmonics. Variables used to describe the diastolic part of the curve are the contributions of early diastolic filling (EDF) and atrial contraction (AC) to the filling volume; peak filling rate (PFR), measured as the peak instantaneous slope of early diastolic filling; time to peak filling rate (TPFR) measured from minimal left ventricular counts or from maximal left ventricular counts.
Left ventricular volume (% end-diastolic volume) )
100 80 60 40 TPFR 20 0 EDF PFR
AC
0,0
0,2
0,4
0,6
0,8
1,0
Time (sec)
12
Chapter 2
variables as age, heart rate and ejection fraction, see chapter 3) must be taken into account (Bonow 1991, Udelson 1994). The acquisition of left ventricular gated blood pool scintigraphy can lead to many technical errors (Wagner 1989). Cycle length fluctuations have a detrimental effect on the diastolic part of the left ventricular volume curve (Hammermeister 1974). It is therefore essential to exclude extrasystolic and postextrasystolic beats and use an appropriate cycle-length window (Juni 1988). In the Martini Hospital in Groningen count drop-off was minimised using a 5% cycle length window with forward gating (Juni 1988). Further, temporal resolution with a high framing rate is necessary to accurately reflect the instantaneous deflections in the time activity curve (Udelson 1994). High temporal resolution in the multigated studies of the present thesis was achieved with a framing rate of 50 frames per second (20 msec per frame). Obviously, high temporal resolution should not lead to a decrease of the count number per frame, which might lead to an increasing degree of statistical imprecision. We used a minimum of 150,000 counts per frame in the present studies of this thesis. Temporal smoothing could therefore be achieved with five Fourier harmonics, thereby keeping the risk of systematic underestimation of the filling parameters low (Bacharach 1983, Bonow 1989, Bonow 1991). Because of an unpredictable variation in red cell tagging with technetium-99m pertechnetate, and a variable amount of absorption between patients, measurements of count changes in the time-activity curve must be related (normalised) to a physiologic variable derived from the time activity curve, e.g. enddiastolic volume and stroke (or filling) volume. Therefore this normalised parameter is not only influenced by the true filling rate (in milliliters/second) but also by the normalisation parameter. It is therefore recommended to perform normalisation to more than one parameter (Udelson 1994). From the obtained time activity curve which closely resembles the left ventricular volume curve, a number of determinants of left ventricular filling can be taken (Figure 2.2). These parameters are used throughout the present thesis. The peak filling rate (PFR in end diastolic volume (EDV) or filling volume (FV) per second) is the most widely used parameter of left ventricular filling, and measures the maximum instantaneous filling rate during early rapid filling. The normal value varies widely, and is dependent on age, heart rate, and ejection fraction (see Chapter 3). The time to peak filling rate (TPFR) is the time interval from minimal left ventricular counts to the peak filling rate expressed in milliseconds. In the present thesis this interval is used for TPFR, unless otherwise stated. Time to peak filling rate can alternatively be measured from maximal left ventricular counts to peak filling rate (Friedman 1986). The duration of systole is then included. This parameter therefore concerns the entire contractionrelaxation cycle. This may be of importance since in many clinical conditions of diastolic failure impaired relaxation and prolonged contraction are present in combination depending on aetiology and stage of the disease (Brutsaert 1993). The atrial contribution to diastolic filling can be assessed by measuring the increase in relative left ventricular volume that is due to atrial contraction. The moment of
Diastolic function: focus on the present thesis
13
onset of atrial contraction can either be determined from the time-activity curve or one of its derivatives, or by using the onset of the P wave on the electrocardiogram and adding 40 ms for assumed atrial electrical-mechanical delay as starting-point for the atrial contribution phase in the time-activity curve (see Chapter 4). In chapter 8 the term additional filling fraction (AFF) is introduced because passive diastolic left ventricular filling is assumed to be partly responsible for left ventricular filling in late diastole. Echocardiography. The dynamics of left ventricular filling is studied with Doppler echocardiography of the mitral inflow pattern, which can be divided in an early (E) and an atrial (A) peak filling velocity (Thomas 1991, Quinones 1991). Deceleration time of the peak early transmitral Doppler recording and isovolumic relaxation time can be measured with this technique as well. These parameters have been successfully correlated with invasive measures of diastolic function, e.g. left ventricular filling pressures, the time constant of relaxation , and pulmonary wedge pressure (Scalia 1997, Strk 1989, Yamamoto 1997, Temporelli 1999). An important Doppler echocardiographic pattern associated with impaired prognosis in patients with depressed systolic left ventricular function is the restrictive filling pattern (Nijland 1997). This pattern has a high ratio of peak E and peak A, accompanied by a short deceleration time. Information on diastolic left ventricular function can be supplemented by Doppler pulmonary venous flow parameters (Gentile 1997). High temporal and velocity resolution are important advantages of the Doppler echocardiographic examination of left ventricular diastolic function (Thomas 1994). One of the draw-backs of Doppler echocardiographic measurement of left ventricular diastolic function is however its reproducibility (Heesen 1998). For repeated measurements in twodimensional echocardiography it is therefore advised to have the patients followed by one single investigator (Otterstad 1997). Studies which compared radionuclide angiographic parameters of left ventricular filling with Doppler echocardiographic measurements show a good correlation, provided that the parameters are normalised correctly (Friedman 1986, Bowman 1988). Many observations on left ventricular filling physiology and pathophysiology by radionuclide angiography are paralleled by similar observations on Doppler echocardiography of the mitral inflow pattern, like e.g. the findings with ageing, hypertension, and myocardial ischaemia (Mantero 1995, Hoit 1994, Thomas 1994). More recent techniques like e.g. colour kinesis (Vignon 1998) and colour M-mode (Stugaard 1993) still lack comparison with radionuclide angiography but are promising. Magnetic resonance imaging. With magnetic resonance (MR) imaging it is not only possible to collect anatomic data, but also functional data of the heart (Van Rossum 1998). These functional data can be obtained using different MR techniques, including cine MR imaging and myocardial tagging with radiofrequency pulses (Van Rossum 1998). With phase velocity mapping it is possible to evaluate parameters of diastolic
14
Chapter 2
left ventricular function, i.e. left ventricular inflow propagation and vortex flow in the left ventricle (Yoganathan 1997). How these parameters relate to specific cardiac disease remains to be investigated. DIASTOLIC DYSFUNCTION IN CARDIAC DISEASE Normal systolic function. An increasing number of studies have reported on the presence of congestive heart failure in patients with normal systolic function (Cohn 1990, Bonow 1992, Vasan 1995). The prevalence of normal systolic function among patients with congestive heart failure varies widely between 13% to 74%. The majority of studies suggest a prevalence of about 40% (Vasan 1995). The criteria used for identification of congestive heart failure, age, and the ratio between acute and chronic congestive heart failure in the study groups are responsible for the variability of the reported prevalences (Vasan 1995). Patients with congestive heart failure and normal systolic function at rest are often presumed to have heart failure on the basis of left ventricular diastolic dysfunction (Vasan 1995). However, the presence of diastolic dysfunction needs to be substantiated where possible, although uniform criteria for diastolic dysfunction are not available and have not been applied (Vasan 1995). In order to come to standardisation of diagnostic criteria for diastolic heart failure, the European study group on diastolic heart failure proposed guidelines for the diagnosis of diastolic heart failure (European study group on heart failure 1998). According to these guidelines, diagnosis of diastolic heart failure requires the presence of signs and symptoms of congestive heart failure, presence of normal or only mildly abnormal left ventricular systolic function, and evidence of abnormal left ventricular relaxation, filling, diastolic distensibility or diastolic stiffness (European study group on heart failure 1998). Radionuclide angiographic abnormalities are only described for PFR: < 2.0 EDV/s (age < 30 year), PFR < 1.8 EDV/s (age 30 - 50 year), PFR < 1.6 EDV/s (age > 50 year) based on a study performed by Bonow et al (Bonow 1988). In isolated diastolic dysfunction the left ventricle is unable to fill adequately at normal diastolic pressures (Grossman 1991). Exercise intolerance is one of the important early symptoms of patients with diastolic heart failure (Kitzman 1991). In the genesis of acute pulmonary oedema diastolic dysfunction can play an important role (Grossman 1990). Identification of patients with diastolic left ventricular dysfunction is important because pathophysiology and therapy differ from that of patients with primarily systolic dysfunction. Congestive heart failure with normal systolic function may be seen in a variety of disorders (Table 1; Grossman 1991). These disorders include structural abnormalities of the pericardium, and of the myocardium (e.g. amyloidosis, and fibrosis; Kushwaha 1997, Janicki 1994). Valvular heart disease (primarily mitral and tricuspid stenosis) may cause elevated atrial pressure without systolic dysfunction. In chronic left ventricular volume overload, e.g. in aortic and mitral regurgitation, diastolic dysfunction expressed by increased slope of the end-diastolic pressure volume relation may be present without
Diastolic function: focus on the present thesis
15
systolic dysfunction (Grossman 1976). An acute increase of volume load however causes elevated diastolic filling pressures without primary myocardial dysfunction (Arrighi 1995). In the presence of right ventricular dilatation, left ventricular diastolic dysfunction may be present due to ventricular interdependence (Janicki 1990). In left ventricular hypertrophy diastolic dysfunction may be present as a result of increased myocardial fibrosis and altered myocardial relaxation. Finally, dynamic disorders resulting in relaxation abnormalities, e.g. pressure overload in hypertension with or without left ventricular hypertrophy, and myocardial ischaemia may result in diastolic dysfunction. The prognosis of patients with congestive heart failure and normal systolic function is variable and depends on the underlying pathophysiologic mechanism responsible for the diastolic filling abnormalities. Reported annual mortality rates are lower than that of systolic heart failure, and range between 1.3% and 17.5% depending on aetiology of diastolic dysfunction and age (Vasan 1995). The definite diagnosis of diastolic congestive heart failure is based on the evaluation of systolic and diastolic performance showing elevated left ventricular filling pressures with normal systolic function. A diagnosis of diastolic heart failure is likely when non-invasive techniques show abnormalities of the left ventricular filling pattern with normal systolic function (Arrighi 1995). Depressed systolic function. Signs and symptoms of cardiac failure in patients with depressed systolic function may partly be due to concomitantly altered diastolic properties of the myocardium (Grossman 1976). In patients with heart failure and depressed systolic left ventricular function the severity of systolic dysfunction correlates with prognosis, but not with exercise capacity or symptom status. (Franciosa 1981, Rihal 1994). Diastolic function parameters are found to correlate significantly to symptom status in such patients (Franciosa 1985, Szlachcic 1985, Rihal 1994). An early sign of diastolic heart failure is diminished exercise tolerance (Packer 1990). Recent studies on chronic tachycardia-induced cardiomyopathy leading to marked systolic dysfunction demonstrate that this is associated with an impairment of intrinsic myocardial relaxation (Shinbane 1997, Zile 1996). In patients with left ventricular systolic dysfunction the common finding of diastolic dysfunction, a restrictive filling pattern in particular, appears in addition to left ventricular ejection fraction to be correlated with increased cardiac mortality (Pinamonti 1993, Rihal 1994, Nijland 1997). Coronary artery disease. Myocardial ischaemia may cause transient abnormalities of left ventricular diastolic filling (Arrighi 1995). The majority of patients with coronary artery disease have abnormal diastolic parameters at rest resulting in decreased early diastolic filling and increased atrial transport function (Mahmarian 1990). After coronary artery bypass grafting and percutaneous transluminal coronary angioplasty abnormalities of diastolic filling appear to normalise (Bonow 1982, Lawson 1988).
16
Chapter 2
Impaired relaxation is caused by increased myocardial cytosolic calcium ion concentrations arising from decreased calcium sequestration or increased calcium entry (Bonow 1990). In patients with coronary artery disease left ventricular asynchrony due to regional ischaemia affects global left ventricular filling (Perrone-Filardi 1992). Regional left ventricular nonuniformity can be present in ischaemia, after myocardial infarction, but also in other cardiac conditions e.g. hypertrophic cardiomyopathy and the normal ageing process (Bonow 1990). After myocardial infarction a restrictive filling pattern is indicative of diastolic dysfunction due to initial myocardial stiffness or myocardial failure (Algom 1995). Impaired diastolic filling is a constant pathological finding in patients with previous myocardial infarction, and is more severe in patients with concomitant heart failure (Bareiss 1990). In a recent study with Doppler echocardiography, a restrictive left ventricular filling pattern was a good predictor of cardiac death (Nijland 1997). Tachycardia. Left ventricular diastolic dysfunction may emerge in the presence of inappropriately high heart rates and chronic tachycardia (Brutsaert 1993, Zile 1996). In the presence of chronic tachycardia left ventricular diastolic dysfunction coincides with systolic abnormalities (Shinbane 1997). In the experimental setting of chronic pacing induced cardiomyopathy, the nature of diastolic dysfunction has not been made exactly clear. Generally, in chronic tachycardiomyopathy impaired left ventricular relaxation, increased left ventricular diastolic wall stress, and decreased compliance have been found (Komamura 1992, Zile 1995, Ohno 1994). Administration of inotropic agents could however normalise decreased early left ventricular relaxation, and decreasing loading conditions could normalise increased left ventricular end-diastolic wall stress by reduction of both increased myocardial stiffness and increased time constant of relaxation (Sasayama 1991, Komamura 1992). After cessation of pacing in chronic pacing induced tachycardiomyopathy the normalisation of left ventricular systolic function which may occur, is accompanied by development of left ventricular hypertrophy with persistent diastolic dysfunction, consisting of decreased relaxation and decreased compliance (Tomita 1991). In humans with chronic atrial fibrillation with rapid ventricular response, intrinsic tachycardiomypathy characterised by decreased systolic left ventricular function normalises after restoration of sinus rhythm or adequate rate control (Morris Jr 1965, Packer 1986, Grogan 1992, Rodriguez 1993). This tachycardiomyopathy may be caused by inadequate high heart rate at rest and/or with exercise (Van den Berg 1993). In chronic atrial fibrillation also the atria itself are dilated (Davies 1972). Most authors however agree on (partial) functional recovery of atrial function after chemical and electrical cardioversion, and the maze procedure (Manning 1989, Jovic 1997, Yashima 1997). The increase in Doppler echocardiographic A wave velocity, and decreased E/A ratio after cardioversion of atrial fibrillation may also indicate (transient) impairment of left ventricular relaxation (Xiong 1995). New data on this subject are further discussed in
Diastolic function: focus on the present thesis
17
Chapter 8. Other cardiovascular disease. Impairment of diastolic function is the most characteristic pathophysiologic abnormality in patients with hypertrophic cardiomyopathy, leading to decreased early diastolic filling and increased atrial filling due to diminished relaxation and increased chamber stiffness (Hess 1993, Posma 1994). Also hypertension and secondary left ventricular hypertrophy are manifested by such diastolic abnormalities (Hoit 1994). Patients with cardiac syndrome X also have impaired resting left ventricular diastolic filling which improves after the betablocker atenolol (Fragasso 1997). The normal ageing process is generally associated with structural and functional changes in the heart, leading to decreased early diastolic filling and increased atrial filling (Nixon 1994). A recent study addressed the changes of left ventricular relaxation with age to presence of coronary artery disease, systemic hypertension, left ventricular systolic dysfunction or hypertrophy (Yamakado 1997). In addition, restrictive cardiomyopathy including cardiac amyloidosis and sarcoidosis is associated with impaired ventricular filling (Kushwaha 1997). THERAPEUTIC CONSEQUENCES In the choice of a therapeutic regimen for the treatment of congestive heart failure it is of great importance to know whether it originates from systolic dysfunction or diastolic dysfunction or a combination (Bonow 1992). The identification of the underlying mechanisms responsible for diastolic dysfunction has therapeutic significance as well. Diastolic left ventricular dysfunction may originate from structrural pericardial (e.g. constrictive pericarditis), myocardial changes, (e.g. myocardial fibrosis or amyloidosis), or valvular disease (e.g. mitral stenosis, Covell 1990, Kushwaha 1997). These conditions may require specific surgical or medical interventions. Diastolic dysfunction may originate from functional changes of the heart as well. Here, diastolic dysfunction may be reduced by treatment of the underlying disease, e.g. myocardial ischaemia, blood pressure in case of hypertension, or tachycardia in case of arrhythmia. Calcium channel blockers in heart failure. The negative inotropic effects of calcium channel blockers result from depression of calcium transmembrane transport (Iliceto 1997, Packer 1989). In the intact hemodynamic system this negative inotropic effect is however counterbalanced by peripheral vasodilatation, which reduces left ventricular afterload, but also initiates neurohormonal activation. Despite these factors, verapamil and diltiazem reduce ventricular contractility (Packer 1989, Su 1994, Clozel 1989). Nifedipine however, being a dihydropyridine, increases all contractile indices, probably resulting from reflex stimulation of the sympathetic system (Ferrari 1997, Iliceto 1997). Second generation dihydropyridines may also exert their positive hemodynamic effect by the same mechanism (Lambert 1990). The improvement in cardiac performance after dihydropyridine administration is however less marked than after the
18
Chapter 2
administration of vasodilators that do not depress cardiac contractility (Packer 1989). In ischaemic heart disease, regional systolic dysfunction may lead to global left ventricular dysfunction by remodelling. Calcium channel blockers can play an important role here, by reducing the extent of dysfunctioning myocardium caused by ischaemia, and improving the functional recovery of post-ischaemic but viable myocardium (Iliceto 1997). This effect is obtained by coronary vasodilation thereby improving the myocardial oxygen supply and removing harmful by-products of anaerobic glycolysis (Nayler 1994). Calcium channel blockers also have an energy saving effect on the myocardium by means of their peripheral vasodilative action, which reduces afterload, and by means of their direct negative inotropic myocardial effect. In addition, myocardial energy demand is depressed by heart rate reduction after administration of verapamil or diltiazem (Iliceto 1997, Nayler 1994). Despite beneficial haemodynamic effects of calcium channel blockers in coronary artery disease, the administration of these drugs in congestive heart failure can be detrimental (Packer 1989, Elkayam 1993). The unfavourable effects of shortterm administration have been attributed to the negative inotropic properties of calcium channel blockers. In addition, the reflex augmentation of sympathetic activity in nifedipine often fails to compensate its direct negative inotropic properties in patients with congestive heart failure (Elkayam 1990). Long-term treatment with calcium channel blockers may also have deleterious effects which are probably related to the activation of neurohormonal systems, including the sympathetic nervous system and the reninangiotensin system (Packer 1989, Elkayam 1993). Although second generation calcium antagonists do not induce significant neurohormonal activation, no data are available justifying the use of these drugs in the treatment of heart failure (De Vries 1997). In the treatment of concomitant angina pectoris, the anti-ischaemic effects of calcium antagonists may however be useful (The DEFIANT II Research Group 1997). Several approaches have been suggested to improve the safety of calcium channel blockers in patients with heart failure including development of calcium channel blockers that do not activate the neurohormonal system (Iliceto 1997, Elkayam 1993). In one study the short term treatment of patients with heart failure with the T-channel selective calcium antagonist mibefradil did not raise sympathetic activity (Van der Vring 1998). Because of serious drug interactions and arrhythmogenic effects the drug was however withdrawn from the market by the manufacturer in 1998. Calcium channel blockers and myocardial relaxation. In coronary artery disease regional and global left ventricular diastolic function may be impaired as a result of 'silent' myocardial ischaemia (Mahmarian 1990, Bareiss 1990). Relaxation, being an energy consuming process, may be improved by reversing myocardial ischaemia e.g. by bypass surgery or percutaneous transluminal coronary angioplasty (Lawson 1988, Bonow 1982). Calcium channel blockers are also capable of increasing coronary blood
Diastolic function: focus on the present thesis
19
flow significantly, either via natural vessels or collaterals or both. In the presence of left ventricular relaxation abnormalities due to myocardial ischaemia, they may therefore improve diastolic function (Dienstl 1992, The DEFIANT II Research Group 1997, Hanet 1990). In addition, a reduction in afterload of the left ventricle by peripheral vasodilatation may also improve diastolic left ventricular function, as it decreases myocardial oxygen demand (The DEFIANT II Research Group 1997). The negative inotropic effect of calcium channel blockers may decrease myocardial energy demand directly, thus decreasing ischaemia, and improving myocardial relaxation. The latter explanation is more likely in the administration of phenylalkylamines or benzothiazepines, but not in dihydropyridines for they may enhance myocardial contractility (Lahiri 1990). In hypertensive left ventricular hypertrophy and hypertrophic cardiomyopathy, left ventricular filling is often impaired as a result of reduced left ventricular relaxation, reduced subendocardial coronary reserve, a reduction in adenosine triphosphate, or increased chamber stiffness due to increased myocardial collagen content (Smith 1985, Vatner 1990). In addition, regional nonuniformity which arises from nonhomogeneous distribution of these factors may further impair global left ventricular filling (Bonow 1990). Indexes of left ventricular relaxation have been shown to be improved after the administration of nifedipine, diltiazem, and verapamil (Bonow 1990). In addition, in these patients verapamil improved exercise tolerance and diastolic pressure volume relations despite its negative inotropic effect, normalised atrial contribution to left ventricular filling, and reduced left ventricular asynchrony (Bonow 1985, Bonow 1983b, Bonow 1983a, Bonow 1987). Finally, the structural and functional changes in diastolic function in the normal ageing process, may at least in part be reversed by the administration of verapamil (Nixon 1994, Arrighi 1994). Diuretics. Diuretics effectively reduce pulmonary congestion and oedema. In haemodynamic studies with diuretics, filling pressures of both left and right ventricles are reduced (Udelson 1993). Exercise tolerance can thus be improved with little change in systolic performance (Brutsaert 1993). Nitrates. A favourable effect on diastolic performance is also noted with nitroprusside and nitroglycerin resulting in diminished filling pressures at smaller chamber volumes (Udelson 1993). However, in diastolic heart failure a drastic reduction of preload may result in decreased cardiac output with fatigue and exercise intolerance as a consequence. -Blocking agents. In systolic heart failure -blockers depress left ventricular contractility and relaxation initially (Eichhorn 1992). Long term treatment of heart failure with -blockers may eventually result in increased contractility and improved early
20
Chapter 2
diastolic relaxation (Udelson 1993, Eichhorn 1990). Although the direct effect of blockers on the myocardium are unfavourable for diastolic function, the favourable effects on diastolic function result from reduction of heart rate, blood pressure, left ventricular hypertrophy, and left ventricular ischaemia, (Bonow 1992, Fragasso 1997). -Adrenergic drugs. Although the short-term infusion of -adrenergic drugs has a favourable effect on early diastolic relaxation, there is no influence on the end-diastolic pressure-volume relation (Udelson 1990). Because in patients with diastolic dysfunction, increased heart rate may be unfavourable, -adrenergic drugs must be prescribed with great caution (Smith 1992). Angiotensin-converting enzyme inhibitors. Angiotensin converting enzyme inhibitors possibly have a favourable effect on diastolic function. They diminish filling pressures of both left and right ventricles (Udelson 1990). In addition, left ventricular hypertrophy and blood pressure are decreased (Bonow 1992). In patients with dilated right ventricles, the impeding effect of pericardial constraint and ventricular interdependence on early diastolic filling is diminished by acute angiotensin converting enzyme inhibition (Konstam 1990). In patients with severe systolic left ventricular dysfunction long-term therapy with the angiotensin converting enzyme inhibitor enalapril prevented left ventricular dilatation accompanied by a decreased left ventricular chamber stiffness (Pouleur 1993). Digitalis glycosides. Because digitalis glycosides increase intracellular calcium concentration, they possibly have unfavourable effects in diastolic heart failure. In contrast, possible indirect effects of digitalis including afterload reduction and lower end-systolic volumes may provide an association with lowered filling pressures (Udelson 1993). In a recent study on the effects of chronic digitalisation in systolic heart failure a decrease in the rate and degree of ventricular relaxation was confirmed (Hassapoyannes 1998). This effect did however not abolish favourable effects of digitalis on mortality. A general approach of patients with diastolic heart failure in terms of drug treatment does not (yet) belong to present-day practice. Although effects on heart rate, remodelling and relaxation must be taken into account, the aetiology of heart failure and the type of diastolic dysfunction are often the key to treatment. In clinical trials no internationally accepted uniform diagnostic criteria are used for diastolic heart failure. The lack of uniformity in diagnostic criteria explains why diastolic heart failure in present day practice often is not recognised and poorly understood. Prognosis of patients with heart failure and diastolic left ventricular dysfunction differs from patients with systolic heart failure. Because of the rising incidence of diastolic dysfunction and heart failure in ageing populations it is of
Diastolic function: focus on the present thesis
21
importance to define normal values and variability in cardiac disease of measures of diastolic left ventricular function. Then tailored treatment options for patients with diastolic heart failure may be tested successfully.
References
1. Algom M, Schlesinger Z. Serial changes in left ventricular diastolic indexes derived from doppler echocardiography after anterior wall acute myocardial infarction. Am J Cardiol 1995;75:12721273. Apstein CS, Morgan JP. Cellular mechanisms underlying left ventricular diastolic dysfunction. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;3-24. Arrighi JA, Dilsizian V, Perrone-Filardi P, Diodati JG, Bacharach SL, Bonow RO. Improvement of the age-related impairment in left ventricular diastolic filling with verapamil in the normal human heart. Circulation 1994;90:213-219. Arrighi JA, Soufer R. Left ventricular diastolic function: physiology, methods of assessment, and clinical significance. J Nucl Cardiol 1995;2:525-543. Bacharach SL, Green MV, Vitale D, White G, Douglas MA, Bonow RO, Larson SM. Optimum fourier filtering of cardiac data: a minimum-error method: concise communication. J Nucl Med 1983;24:1176-1184. Bareiss P, Facello A, Constantinesco A, Demangeat JL, Brunot B, Arbogast R, Roul G. Alterations in left ventricular diastolic function in chronic ischemic heart failure. Assessment by radionuclide angiography. Circulation 1990;81(supp III):III-71-III-77. Biasucci LM, Pajaro OE, Tanoue T. Mid-diastolic mitral flow rebound: mechanisms, importance and relation to Doppler indexes of diastolic function. (Abstract). Circulation 1990;82(suppl III):III127. Bonow RO, Kent KM, Rosing DR, Lipson LC, Bacharach SL, Green MV, Epstein SE. Improved left ventricular diastolic filling in patients with coronary artery disease after percutaneous transluminal coronary angioplasty. Circulation 1982;66:1159-1167. Bonow RO, Frederick TM, Bacharach SL, Green MV, Goose PW, Maron BJ, Rosing DR. Atrial systole and left ventricular filling in hypertrophic cardiomyopathy: effect of verapamil. Am J Cardiol 1983a;51:1386-1391. Bonow RO, Ostrow HG, Rosing DR, Cannon RO 3d, Lipson LC Maron BJ, Kent KM,Bacharach SL, Green MV. Effects of verapamil on left ventricular systolic and diastolic function in patients with hypertrophic cardiomyopathy: pressure-volume analysis with a nonimaging scintillation probe. Circulation 1983b;68:1062-1073. Bonow RO, Dilsizian V, Rosing DR, Maron BJ, Bacharach SL, Green MV. Verapamil-induced improvement in left ventricular diastolic filling and increased exercise tolerance in patients with hypertrophic cardiomyopathy: short- and long-term effects. Circulation 1985;72:853-864. Bonow RO, Vitale DF, Maron BJ, Bacharach SL, Frederick TM, Green MV. Regional left ventricular asynchrony and impaired global left ventricular filling in hypertrophic cardiomyopathy: effect of verapamil. J Am Coll Cardiol 1987;9:1108-1116 Bonow RO, Vitale DF, Bacharach SL, Maron BJ, Green MV. Effects of aging on asynchronous left ventricular regional function and global ventricular filling in normal human subjects. J Am Coll Cardiol 1988;11:50-58. Bonow RO, Bacharach SL, Crawford-Green C, Green MV. Influence of temporal smoothing on
2.
3.
4. 5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
22
Chapter 2 quantitation of left ventricular function by gated blood pool scintigraphy. Am J Cardiol 1989;64:921-925.
15.
Bonow RO. Regional left ventricular nonuniformity. Effects on left ventricular diastolic function in ischemic heart disease, hypertrophic cardiomyopathy, and the normal heart. Circulation 1990;81(suppl III):III-54-III-65. Bonow RO. Radionuclide Angiographic Evaluation of Left ventricular diastolic function. Circulation 1991;84(suppl I):I-208-I-215. Bonow RO, Udelson JE. Left ventricular diastolic dysfunction as a cause of congestive heart failure. Mechanisms and management. Ann Intern Med 1992;117:502-510. Bowman LK, Lee FA, Jaffe CC, Mattera J, Wackers FJTh, Zaret BL. Peak filling rate normalized to mitral stroke volume: a new doppler echocardiographic filling index validated by radionuclide angiographic techniques. J Am Coll Cardiol 1988;12:937-943. Braunwald E. Pathofysiology of Heart Failure. In: Braunwald E, ed. Heartdisease. Philadelphia: Saunders, 1992; 393-418. Brecher GA, Kolder H, Horres AD. Ventricular volume of nonbeating excised dog hearts in the state of equilibrium. Circ Res 1966;19:1080. Brutsaert DL, Housmans PR, Goethals MA. Dual control of relaxation. Its role in the ventricular function in the mamalian heart. Circ Research 1980;47:637-652. Brutsaert DL, Rademakers FE, Sys SU. Triple control of relaxation: implications in cardiac disease. Circulation 1984;69:190-196. Brutsaert DL, Sys SU, Gillebert TC. Diastolic failure: pathofysiology and therapeutic implications. J Am Coll Cardiol 1993;22:318-325. Brutsaert DL, Sys SU. Relaxation and diastole of the heart. Physiol Rev 1989;69:1228-1315. Clozel JP, Banken L, Osterrieder W. Effects of Ro 40-5967, a novel calcium antagonist, on myocardial function during ischemia induced by lowering coronary perfusion pressure in dogs: comparison with verapamil. J Cardiovasc Pharmacol 1989;14:713-721. Cohn JN. Heart failure with normal ejection fraction. The V-HeFT Study. Circulation 1990;81(suppl III):III-48-III-53. Courtois M, Kovacs SJ, Ludbrook PA. Transmitral pressure-flow velocity relation. Importance of regional pressure gradients in the left ventricle during diastole. Circulation 1988;78:661-671. Courtois M, Mechem CJ, Barzilai B, Gutierrez F, Ludbrook PA. Delineation of determinants of left ventricular early filling. Saline versus blood transfusion. Circulation 1994;90:2041-2050. Covell JW. Factors influencing diastolic function. Possible role of the extracellular matrix. Circulation 1990;81(suppl III):III-155-III158. Davies MJ, Pomerance A. Pathology of atrial fibrillation in man. Br Heart J 1972;34:520-525. De Vries RJ. Second generation calcium channel blockers in chronic heart failure. Thesis, University of Groningen, 1997. Dienstl F, Motro M, Poole Wilson PA, Schartl M, Bassand JP, Van Dalen FJ, Emmott SN,Horowitz M, Hugenholtz PG. Improved diastolic function with the calcium antagonist nisoldipine (coat-core) in patients post myocardial infarction: results of the DEFIANT study. Eur Heart J 1992;13:1496-1505. Ebstein. Die diastole des herzens. Ergebnisse der Physiologie 1904;3 (2):123-194. Eichhorn EJ, Bedotto JB, Malloy CR, Hatfield BA, Deitchman D, Brown M, Willard JE,Grayburn PA. Effect of -adrenergic blockade on myocardial function and energetics in congestive heart failure. Improvement in hemodynamic, contractile, and diastolic performance with bucindolol. Circulation 1990;82:473-483. Eichhorn EJ. The paradox of -adrenergic blockade for the management of congestive heart
16. 17. 18.
19. 20. 21. 22. 23. 24. 25.
26. 27. 28. 29. 30. 31. 32.
33. 34.
35.
Diastolic function: focus on the present thesis failure. Am J Med 1992;92:527-538. 36.
23
Elkayam U, Amin J, Anilkumar M, Vasquez J, Weber L, Rahimtoola SH. A prospective, randomized, double-blind, crossover study to compare the efficacy and safety of chronic nifedipine therapy with that of isosorbide dinitrate and their combination in the treatment of chronic congestive heart failure. Circulation 1990;82:1954-1961. Elkayam U, Shotan A, Mehra A, Ostrzega E. Calcium channel blockers in heart failure. J Am Coll Cardiol 1993;22(suppl A):139A-144A. European study group on diastolic heart failure. How to diagnose diastolic heart failure. Eur Heart J 1998;19:990-1003. Ferrari R. Major differences among the three classes of calcium antagonists. Eur Heart J 1997;18 (suppl A):A56-A70. Figueredo VM, Camacho SA. Basic mechanisms of myocardial dysfunction: cellular pathophysiology of heart filure. Curr Opin Cardiol 1993;8:369-375. Fragasso G, Chierchia SL, Pizetti G, Rossetti E, Carlino M, Gerosa S, Carandente O,Fedele A, Cattaneo N. Impaired left ventricular filling dynamics in patients with angina and angiographically normal coronary arteries: effect of beta adrenergic blockade. Heart 1997;77:32-39. Franciosa JA, Baker BJ, Seth L. Pulmonary versus systemic hemodynamics in determining exercise capacity of patients with chronic left ventricular failure. Am Heart J 1985;110:807-813. Franciosa JA, Park M, Levine TB. Lack of correlation between exercise capacity and indexes of resting left ventricular performance in heart failure. Am J Cardiol 1981;47:33-39. Friedman BJ, Drinkovic N, Miles H, Shih WJ, Mazzoleni A, De Maria AN. Assessment of left ventricular diastolic function: comparison of doppler echocardiography and gated blood pool scintigraphy. J Am Coll Cardiol 1986;8:1348-1354 Gaasch WH. Passive elastic properties of the left ventricle. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;143149. Gentile F, Mantero A, Lippolis A, Ornaghi M, Azzolini M, Barbier P, Beretta L,Casazza F, Cornot R, Faletra F, Giagnoni E, Gualtierotti C, Lombroso S, Mattioli R. Pulmonary venous flow velocity patterns in 143 normal subjects aged 20 to 80 years old. An echo 2D colour Doppler cooperative study. Eur Heart J 1997;18:148-164. Gillebert TC, Sys SU. Physiologic control of relaxation in isolated cardiac muscle and intact left ventricle. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;25-42. Grogan M, Smith HC, Gersh BJ, Wood DL. Left ventricular dysfunction due to atrial fibrillation in patients initially believed to have idiopathic dilated cardiomyopathy. Am J Cardiol 1992;69:15701573. Grossman W, McLaurin LP. Diastolic properties of the left ventricle. Ann Intern Med 1976;84:316-326. Grossman W. Diastolic dysfunction in congestive heart failure. N Engl J Med 1991;325:1557-64. Grossman W. Evaluation of systolic and diastolic function of the myocardium. In: Grossman W, Baim DS, ed. Cardiac catheterization, angiography and intervention. Philadelphia: Lea & Febiger, 1990;333. Grossman W. Evaluation of systolic and diastolic function of the myocardium In: Grossman W, Baim DS, ed. Cardiac catheterization, angiography and intervention. Philadelphia: Lea & Febiger, 1986;301-319. Hammermeister KE, Warbasse JR. The rate of change of left ventricular volume in man: diastolic events in health and disease. Circulation 1974;49:739-747. Hanet C, Rousseau MF, Van Eyll C, Pouleur H. Effects of nicardipine on regional diastolic left
37. 38. 39. 40. 41.
42. 43. 44.
45.
46.
47.
48.
49. 50. 51.
52.
53. 54.
24
Chapter 2 ventricular function in patients with angina pectoris. Circulation 1990;81(suppl III):III-148-III-154.
55. 56. 57. 58.
Hassapoyannes CA, Bergh ME, Movahed MR, Easterling BM, Omoigui NA. Diastolic effects of chronic digitalization in systolic heart failure. Am Heart J 1998;136:688-695. Heesen WF. Isolated systolic hypertension. Pathophysiology and effects of treatment. Thesis. Groningen University, The Netherlands, 1998. Hess OM, Krayenbuehl HP. Management of hypertrophic cardiomyopathy. Curr Opin Cardiol 1993;8:434-440. Hoit BD, Walsh RA. Diastolic dysfunctionin hypertensive heart disease. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;354-372. Hori M, Yellin EL, Sonnenblick EH. Left ventricular diastolic suction as a mechanism of ventricular filling. Jpn Circ J 1982;46(1):124-129. Iliceto S. Left ventricular dysfunction: Which role for calcium antagonists? Eur Heart J 1997;18(suppl A):A87-A91. Ishida Y, Meisner JS, Tsujioka K, Gallo JI, Yoran C, Frater RWM, Yellin EL. Left venricular filling dynamics: influence of left ventricular relaxation and left atrial pressure. Circulation 1986;74:187196. Janicki JS, Matsubara BB. Myocardial collagen and left ventricular diastolic dysfunction. In: Gaasch WH, LeWinter MM ,ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;125-140. Janicki JS. Influence of the pericardium and ventricular interdependence on left ventricular diastolic and systolic function in patients with heart failure. Circulation 1990;81(suppl III):III-15-III20. Jovic A, Troskot R. Recovery of atrial systolic function after pharmacological conversion of chronic atrial fibrillation to sinus rhythm: a Doppler echocardiographic study. Heart 1997;77:4649. Juni JE, Chen CC. Effects of gating modes on the analysis of left ventricular function in the presence of heart rate variation. J Nucl Med 1988;29:1272-1278. Keren G, Meisner JS, Sherez J, Yellin EL, Laniado S. Interrelationship of mid-diastolic mitral valve motion, pulmonary venous flow, and transmitral flow. Circulation 1986;74:36-44. Keren G, Sherez J, Megidish R, Levitt B, Laniado S. Pulmonary venous flow pattern-its relationship to cardiac dynamics. Circulation 1985;71:1105-1112. Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan MJ. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the FrankStarling mechanism. J Am Coll Cardiol 1991;17:1065-72. Komamura K, Shannon RP, Pasipoularides A, Ihara T, Lader AS, Patrick TA, Bishop SP,Vatner SF. Alterations in left ventricular diastolic function in conscious dogs with pacing-induced heart failure. J Clin Invest 1992;89:1825-1838. Kono T, Sabbah HN, Rosman H, Alam M, Stein P, Goldstein S. Left atrial contribution to ventricular filling during the course of evolving heart failure. Circulation 1992;86:1317-1322. Konstam MA, Kronenberg MW, Udelson JE, Metherall J, Dolan N, Edens TR, Howe DM,Yusuf S, Youngblood M, Toltsis H, and the SOLVD Investigators. Effect of acute angiotensin converting enzyme inhibition on left ventricular filling in patients with congestive heart failure. Relationto right ventricular volumes. Circulation 1990;81(suppl III):III-115-III-122. Kushwaha SS, Fallon JT, Fuster V. Restrictive cardiomyopathy N Eng J Med 1997;336:267-276. Lahiri A, Rodrigues EA, Carboni GP, Raftery EB. Effects of long-term treatment with calcium antagonists on left ventricular diastolic function in stable angina and heart failure. Circulation 1990;81(suppl III):III-130-III-138.
59. 60. 61.
62.
63.
64.
65. 66. 67. 68.
69.
70. 71.
72. 73.
Diastolic function: focus on the present thesis 74. 75. 76. 77.
25
Lambert CR, Buss DD, Pepine CJ. Effect of nicardipine on myocardial function in vitro and in vivo. Circulation 1990;81 (suppl III):III-139-III-147. Lawson WE, Seifert F, Anagnostopoulos C, Hills DJ, Swinford RD, Cohn PF. Effect of coronary artery bypass grafting on left ventricular diastolic function. Am J Cardiol 1988;61:283-287. Little WC, Downes TR. Clinical evaluation of left ventricular diastolic performance. Prog Cardiovasc Dis 1990;32:273-290. Little WC, Ohno M, Kitzman DW, Thomas JD, Cheng CP. Determination of left ventricular chamber stiffness from the time for deceleration of early left ventricular filling. Circulation 1995;92:1933-1939. Mackenzie J. Diseases of the heart. London: Oxford medical publications, 1914;148. Mahmarian JJ, Pratt CM. Silent myocardial ischemia in patients with coronary artery disease: possible link with diastolic left ventricular dysfunction. Circulation 1990;81(suppl III):III-33-III-40 Manning WJ, Leeman DE, Gotch PJ, Come PC. Pulsed Doppler evaluation of atrial mechanical function after electrical cardioversion of atrial fibrillation. J Am Coll Cardiol 1989;13:617-623. Mantero A, Gentile F, Gualtierotti C, Azzolini M, Barbier P, Beretta L, Casazza F,Corno R, Giagnoni E, Lippolis A, Lombroso S, Mattioli R, Morabito A, Ornaghi M, Pepi M, Pezzano A. Left ventricular diastolic parameters in 288 normal subjects from 20 to 80 years old. Eur Heart J 1995;16:94-105. Meijler FL, Brutsaert DL. Relaxation and diastole. Precedings of the fourth workshop on contractile behavior of the heart. Introduction. Eur J Cardiol 1978;7 (supplement 1):1. Meisner JS, Keren G, Pajaro OE, Mani A, Strom JA, Frater RWM, Laniado S,Yellin EL. Atrial contribution to ventricular filling in mitral stenosis. Circulation 1991;84:1469-1480. Morgan JP. Abnormal intracellular modulation of calcium as a major cause of cardiac contractile dysfunction. N Engl J Med 1991;325:625-32. Morris Jr JJ, Entman M, North WC, Kong Y, McIntosh H. The changes in cardiac output with reversion of atrial fibrillation to sinus rhythm. Circulation 1965;31:670-678. Nayler WG. The ischemic myocardium and calcium antagonists. In: Opie LH, ed. Myocardial protection by calcium antagonists. New York: Wiley-Liss, 1994;46-61. Nijland F, Kamp O, Karreman AJP, Van Eenige MJ, Visser CA. Prognostic implications of restrictive left ventricular filling in acute myocardial infarction: a serial Doppler echocardiographic study. J Am Coll Cardiol 1997;30:1618-1624. Nixon JV, Burns CA. Cardiac effects of aging and diastolic dysfunction in the elderly. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;427-435. Ohno M, Cheng CP, Little WC. Mechanism of altered patterns of left ventricular filling during the dvelopment of congestive heart failure. Circulation 1994;89:2241-2250. Otterstad JE, Froeland G, St. John Sutton MS, Holme I. Accuracy and reproducibility of biplane two-dimensional echocardiographic measurements of left ventricular dimensions and function. Eur Heart J 1997;18:507-513. Packer DL, Bardy GH, Worley SJ, Smith MS, Cobb FR, Coleman E, Gallaghar JJ,German LD. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. Am J Cardiol 1986;57:563-570. Packer M. Abnormalities of diastolic function as a potential cause of exercise intolerance in chronic heart failure. Circulation 1990;81(suppl III):III-78-III-86. Packer M. Pathophysiological mechanisms underlying the adverse effects of calcium channelblocking drugs in patients with chronic heart failure. Circulation 1989;80(supplIV):IV-59-IV-67. Perrone-Filardi P, Bacharach SL, Dilsizian V, Bonow RO. Effects of regional systolic
78. 79. 80. 81.
82. 83. 84. 85. 86. 87.
88.
89. 90.
91.
92. 93. 94.
26
Chapter 2 asynchrony on left ventricular global diastolic function in patients with coronary artery disease. J Am Coll Cardiol 1992;19:739-744.
95.
PinamontiB, Di Lenarda A, Sinagra G, Camerini F, and the Heart Muscle Disease Study Group. Restrictive left ventricular filling pattern in dilated cardiomyopathy assessed by Doppler echocardiography: clinical, echocardiographic and hemodynamic correlations and prognostic implications. J Am Coll Cardiol 1993;22:808-815. Posma JL, Blanksma PK, Van der Wall E, Lie KI. Acute intravenous versus chronic oral drug effects of verapamil on left ventricular diastolic function in patients with hypertrophic cardiomyopathy. J Cardiovasc Pharmacol 1994;24:969-973. Pouleur H, Rousseau MF, Van Eyll C, Stoleru L, Hayashida W, Udelson JA, Dolan N,Kinan D, Galagher P, Ahn S, Benedict CR, Yusuf S, Konstam M, for the SOLVD Investigators. Effects of long-term enalapril therapy on left ventricular diastolic properties in patients with depressed ejection fraction. Circulation 1993;88:481-491. Quinones MA. How to assess diastolic function by doppler echocardiography. In: Braunwald E, ed. Heartdisease update. Philadelphia: Saunders, 1991;15;351-358. Rihal CS, Nishimura RA, Hatle LK, Bailey KR, Tajik AJ. Systolic and diastolic dysfunction in patients with clinical diagnosis of dilated cardiomyopathy. Circulation 1994;90:2772-2779. Rodriguez LM, Smeets JLRM Xie B, de Chillou C, Cheriex E, Pieters F, Metzgers J,den Dulk K, Wellens HJJ. Improvement in left ventricular function by ablation of atrioventrcular nodal conduction in selected patients with lone atrial fibrillation. Am J Cardiol 1993;72:1137-1141. Rowlands DJ, Logan WFWE, Howitt G. Atrial function after cardioversion. Am Heart J 1967;74:149-160. Sabbah HN, Stein PD. Pressure-diameter relations during early diastole in dogs: incompatibility with the concept of passive left ventricular filling. Circ Res 1981;48:357-365. Sasayama S, Asanoi H, Ishizaka S. Mechanics of contraction and relaxation of the ventricle in experimental heart failure produced by rapid ventricular pacing in the conscious dog. Eur Heart J 1991;12(Supplement C):35-41. Scalia GM, Greenberg NL, McCarthy PM, Thomas JD, Vandrvoort PM. Noninvasive assessment of the ventricular relaxation time constant (T) in humans by Doppler echocardiography. Circulation 1997;95:151-155. Shinbane JS, Wood MA, Jensen DN, Ellenbogen KA, Fitzpatrick AP, Scheinman MM. Tachycardia-induced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol 1997;29:709-715. Shintani H, Glantz A. The left ventricular diastolic pressure-volume relation, relaxation, and filling. In: GaaschWH, LeWinter MM, eds. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;57-88. Smith TW, Braunwald E, Kelly RA. The management of heart failure. In: Braunwald E, ed. Heartdisease. Philadelphia: Saunders, 1992; 464-519. Smith VE, Schulman P, Karimeddini MK, White WB, Meeran MK, Katz AM. Rapid ventricular filling in left ventricular hypertrophy: II. pathologic hypertrophy. J Am Coll Cardiol 1985;5:869-874 Strk TV, Mller RM, Piske GJ, Ewert CO, Hochrein H. Noninvasive measurement of left ventricular filling pressures by means of transmitral pulsed doppler ultrasound. Am J Cardiol 1989;64:655-660. Stugaard M, Smiseth OA, Risoe C, Ihlen H. Intraventricular early diastolic filling during acute myocardial ischemia. Assessment by multigated color M-mode echocardiography. Circulation 1993;88:2705-2713. Su J, Renaud N, Carayon A, Crozatier B, Hittinger L, Laplace M. Effects of the calcium channel blockers, diltiazem and ro 40-5967, on systemic haemodynamics and plasma noradrenaline levels in conscious dogs with pacing-induced heart failure. Br J Pharmacol 1994;113:395-402.
96.
97.
98. 99. 100.
101. 102. 103.
104.
105.
106.
107. 108. 109.
110.
111.
Diastolic function: focus on the present thesis 112. 113. 114. Suga H. Importance of atrial compliance in cardiac performance. Circ Res 1974;35:39-43.
27
Szlachcic J, Massie BM, Kramer BL, Topic N, Tubeau J. Correlates and prognostic implication of exercise capacity in chronic congestive heart failure. Am J Cardiol 1985;55:1037-1042. Temporelli PL, Scapellato F, Corra U, Eleuteri E, Imparato A, Giannuzzi P. Estimation of pulmonary wedge pressure by transmitral doppler in patients with chronic heart failure and atrial fibrillation. Am J Cardiol 1999;83:724-727. The DEFIANT-II Research group. Doppler flow and echocardiography in functional cardiac insufficiency: assessment of nisoldipine therapy. Results of the DEFIANT-II study. Eur Heart J 1997;18:31-40. Thomas JD, Weyman AE. Echocardiographic doppler evaluation of left ventricular diastolic function. Physics and physiology. Circulation 1991;84:977-990. Thomas JD. Dopller echocardiography and left ventricular diastolic function. In: GaaschWH, LeWinter MM, eds. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;192-218. Tomita M, Spinale FG, Crawford FA, Zile MR. Changes in left ventricular volume, mass, and function during the development and regression of supraventricular tachycardia-induced cardiomyopathy: disparity between recovery of systolic versus diastolic function. Circulation 1991;83:635-644. Udelson JE, Bacharach SL, Cannon RO 3d, Bonow RO. Minimum left ventricular pressure during -adrenergic stimulation in human subjects: Evidence for elastic recoil and diatolic "suction" in the normal heart. Circulation 1990;82:1174-1182. Udelson JE, Bonow RO. Radionuclide angiographic evaluation of left ventricular diastolic function. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;167-191. Udelson JE, Surks H, Konstam MA. The importance of left ventricular diastolic dysfunction and right ventricular performance in the hart failure syndrome. Curr Opin Cardiol 1993;8:383-396. Van den Berg MP, Crijns HJGM, Gosselink ATM, Van den Broek SAJ, Hillege HJ, Van Veldhuisen DJ, Lie KI. Chronotropic response to exercise in patients with atrial fibrillation: relation to functional state. Br Heart J 1993;70:150-153. Van der Vring JAFM, Cleophas AJM, Van der Wall EE, Niemeyer MG, Bernink PJ, Knol HR, Van Veldhuisen DJ, Braun SJ, Kobrin I, Crijns HJGM. Effects of mibefradil, a T-channel-selective calcium channel blocker, on sympathetic activity in patients with congestive heart failure. Cardiologie 1998;;5:506-511. Van der Werf T. Invasief onderzoek van de systolische en diastolische linkerventrikelfunctie. In: Werf T van der, red. Linkerventrikelfunctie tijdens systole en diastole. Utrecht: Bunge, 1991;5673. Van Rossum AC. Magnetic resonance imaging of cardiac function and flow: present and future. In: Van der Wall EE, Blanksma PK, Niemeyer MG, Vaalburg W, Crijns HJGM, ed. Advanced imaging in coronary artery disease. Dordrecht: Kluwer academic publishers, 1998;289-306. Vasan RS, Benjamin EJ, Levy D. Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. J AM Coll Cardiol 1995;26:1565-1574. Vasan RS, Benjamin EJ, Levy D. Congestive heart failure with normal left ventricular systolic function. Clinical approaches to the diagnosis and treatment of diastolic heart failure. Arch Intern Med 1996;156:146-157. Vatner SF, Shannon R, Hittinger L. Reduced subendocardial coronary reserve. A potential mechanism for impaired diastolic function in the hypertrophied and failing heart. Circulation 1990;81(suppl III):III-8-III-14. Vignon P, Mor-Avi V, Weinert L, Koch R, Spencer KT, Lang RM. Quantitative evaluation of global and regional left ventricular diastolic function with color kinesis. Circulation 1998;97:1053-
115.
116. 117.
118.
119.
120.
121. 122.
123.
124.
125.
126. 127.
128.
129.
28
Chapter 2 1061.
130. 131. 132.
Wagner RH, Halama JR, Henkin RE, Dillehay GL, Sobotka PA. Errors in determination of left ventricular functional parameters. J Nucl Med 1989;30:1870-1874. Wang K, Gibson DG. Non-invasive detection of left atrial mechanical failure in patients with left ventricular disease. Br Heart J 1995;74:536-540. WiggersCJ. Studies on the consecutive phases of the cardiac cycle. I. The duration of the consecutive phases of the cardiac cycle and the criteria for their precise determination. Am J Physiol 1921;56:415-438. WiggersCJ. Studies on the consecutive phases of the cardiac cycle. II. The laws governing the relative duration of ventricular systole and diastole. Am J Physiol 1921;56:438-459. Xiong C, Sonnhag C, Nylander E, Wranne B. Atrial and ventricular function after cardioversion of atrial fibrillation. Br Heart J 1995;74:254-260. Yamakado T, Takagi E, Okubo S, Imanaka-Yoshida K, Tarumi T, Nakamura M, Nakano T. Effects of aging on left ventricular relaxation in humans. Analysis of left ventricular isovolumic pressure decay. Circulation 1997;95:917-923. Yamamoto K, Nishimura RA, Chaliki HP, Appleton CP, Holmes Jr DR, Redfield MM. Determination of left ventricular filling pressure by doppler echocardiography in patients with coronary artery disease: critical role of left ventricular systolic function. J Am Coll Cardiol 1997;30:1819-1826. Yashima N. Nasu M, Kawazoe K, Hiramori K. Serial evaluation of atrial function by Doppler echocardiography after the maze procedure for chronic atrial fibrillation. Eur Heart J 1997;18:496-502. Yellin EL, Hori M, Yoran C. Left ventricular relaxation in the filling and nonfilling intact canine heart. Am J Physiol 1986;250 Heart Circ Physiol 19):H620-H629. Yellin EL, Meisner JS, Nikolic SD, Keren G. The scientific basis for the relations between pulsed-doppler transmitral velocity patterns and left heart chamber properties. Echocardiography 1992;9:313-338. Yellin EL, Nikolic S, Frater RWM. Left ventricular filling dynamics and diastolic function. Prog Cardiovasc Dis 1990;32:247-271. Yellin EL, Nikolic SD. Diastolic suction and the dynamics of left ventricular filling. In: Gaasch WH, LeWinter MM, ed. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger, 1994;89-102. Yoganathan AP. Assessment of diastolic function with velocity-encoded magnetic resonance imaging. Heartforum 1997;10 (suppl1):50-56. Zile MR, Mukherjee R, Clayton C, Kato S, Spinale FG. Effects of chronic supraventricular pacing tachycardia on relaxation rate in isolated cardiac muscle cells. Am J Physiol 1995;268 (Heart Circ Physiol 37):H2104-H2113. Zile MR. The development of diastolic dysfunction in chronic tachycardia. In: Spinale FG, ed. Pathophysiology of tachycardia-induced heart failure. Armonk, NY: Futura Publishing Company, Inc.1996;25-44.
133. 134. 135.
136.
137.
138. 139.
140. 141.
142.
143.
144.
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- ACLS Cheat SheetDocument8 pagesACLS Cheat SheetLenTheRN85% (27)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Responses To Altered Oxygenation, Cardiac and Tissue - Anatomy To AssessmentDocument254 pagesResponses To Altered Oxygenation, Cardiac and Tissue - Anatomy To Assessmentlouradel100% (1)
- ECG Crib SheetDocument2 pagesECG Crib Sheetkp180surfingPas encore d'évaluation
- ECG Mastery Blue Belt Workbook PDFDocument135 pagesECG Mastery Blue Belt Workbook PDFPadma Priya Duvvuri100% (5)
- Auspicious Days - MAY 2014: Siddhi YogaDocument2 pagesAuspicious Days - MAY 2014: Siddhi YogaKrishna RathodPas encore d'évaluation
- Tomato Rasam (Indian Spiced Tomato Soup) : Search For Your Favorite RecipeDocument3 pagesTomato Rasam (Indian Spiced Tomato Soup) : Search For Your Favorite RecipeKrishna RathodPas encore d'évaluation
- PranayamDocument8 pagesPranayamKrishna RathodPas encore d'évaluation
- Sankasht ChaturthiDocument3 pagesSankasht ChaturthiKrishna RathodPas encore d'évaluation
- Kali Pratyangira StotraDocument4 pagesKali Pratyangira Stotrasumit girdharwal100% (7)
- Coomb's TestDocument3 pagesCoomb's TestKrishna RathodPas encore d'évaluation
- Parivar, Bhopal, India: Site Info Who Is Trace Route RBL Check What's My IP?Document2 pagesParivar, Bhopal, India: Site Info Who Is Trace Route RBL Check What's My IP?Krishna RathodPas encore d'évaluation
- ArdhanArI MeanDocument3 pagesArdhanArI MeanKrishna RathodPas encore d'évaluation
- 506 1 RBSK Merit List FemaleDocument23 pages506 1 RBSK Merit List FemaleKrishna Rathod0% (1)
- SPW Power of GayathriDocument4 pagesSPW Power of GayathriKrishna RathodPas encore d'évaluation
- Viral Hepatitis B: DR Paul T Francis, MD Community Medicine College of Medicine, ZawiaDocument10 pagesViral Hepatitis B: DR Paul T Francis, MD Community Medicine College of Medicine, ZawiaKrishna RathodPas encore d'évaluation
- Astro Muhurat Spirituality: 5-2-10 Gupt Navratra / Navratri (Muhurat)Document4 pagesAstro Muhurat Spirituality: 5-2-10 Gupt Navratra / Navratri (Muhurat)Krishna RathodPas encore d'évaluation
- Astro Muhurat Spirituality: 8-2-1 REMEDY (GANESHA MANTRA) For Good Education, Good Business, Good JobDocument4 pagesAstro Muhurat Spirituality: 8-2-1 REMEDY (GANESHA MANTRA) For Good Education, Good Business, Good JobKrishna RathodPas encore d'évaluation
- Astro Muhurat Spirituality: 8-2-15 Tryakshar Mrityunjaya MantraDocument4 pagesAstro Muhurat Spirituality: 8-2-15 Tryakshar Mrityunjaya MantraKrishna RathodPas encore d'évaluation
- CSS 6 - Right Ventricular Failure - Dr. Pudji SP - PD-KKV - Rizky Regia Triseynesya 1815136Document16 pagesCSS 6 - Right Ventricular Failure - Dr. Pudji SP - PD-KKV - Rizky Regia Triseynesya 1815136Rizky Regia TriseynesyaPas encore d'évaluation
- Procedure in Assessing Blood PressureDocument4 pagesProcedure in Assessing Blood PressurecrrfrncPas encore d'évaluation
- Myocardial Ischemia: Dr. Wael H. Mansy, MDDocument37 pagesMyocardial Ischemia: Dr. Wael H. Mansy, MDHaleema SultanPas encore d'évaluation
- ECG-Naming The PRST Waves - (6!19!2012)Document7 pagesECG-Naming The PRST Waves - (6!19!2012)cornondaPas encore d'évaluation
- ACLS Drug TherapyDocument8 pagesACLS Drug TherapySahrensPas encore d'évaluation
- Terapi Jus Semangka - 10-20210203Document10 pagesTerapi Jus Semangka - 10-20210203Mhyla MusaPas encore d'évaluation
- 2018.the Right-Sided ECG For The Right DiagnosisDocument3 pages2018.the Right-Sided ECG For The Right DiagnosisWeila dos Santos VieiraPas encore d'évaluation
- Heart Railway RPF by Radhika MamDocument70 pagesHeart Railway RPF by Radhika Mamyakshat.4141ykPas encore d'évaluation
- RN Expert Guides Cardiovascular Care PDFDocument512 pagesRN Expert Guides Cardiovascular Care PDFSteven Berschaminski100% (1)
- EKG Intermediate Tips Tricks ToolsDocument55 pagesEKG Intermediate Tips Tricks Toolsmayas bsharatPas encore d'évaluation
- ACS LectureDocument74 pagesACS Lecturekarin amalia sabrinaPas encore d'évaluation
- Reflection On Taking Blood PressureDocument3 pagesReflection On Taking Blood PressureFarisa MunirahPas encore d'évaluation
- Neurogenic and Myogenic HeartsDocument14 pagesNeurogenic and Myogenic HeartsYCMOUPas encore d'évaluation
- Fetal DisritmiaDocument18 pagesFetal DisritmiaSebastian ChandraPas encore d'évaluation
- Nursing Case StudyDocument21 pagesNursing Case StudyJeyser T. GamutiaPas encore d'évaluation
- High Blood PressureDocument9 pagesHigh Blood PressureshashidharanPas encore d'évaluation
- Heart PathophysiologyDocument20 pagesHeart PathophysiologyDoctorDrapion100% (2)
- E.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentDocument36 pagesE.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentAch ThungPas encore d'évaluation
- CRM-287004-AB - ACCOLADE L321 - SpecSheetDocument2 pagesCRM-287004-AB - ACCOLADE L321 - SpecSheetcesargasgutPas encore d'évaluation
- Imagen Mmultimodal en Falla Cardiaca IsquemicaDocument15 pagesImagen Mmultimodal en Falla Cardiaca Isquemicaalejandro montesPas encore d'évaluation
- Oxygenation Study GuideDocument8 pagesOxygenation Study GuideJohnPas encore d'évaluation
- Drug Study - Nifedipine PODocument1 pageDrug Study - Nifedipine POJet BautistaPas encore d'évaluation
- KLP 3 - Ebp Telaah Artikel Terapi Musik Klasik Pada Lansia Dengan HipertensiDocument12 pagesKLP 3 - Ebp Telaah Artikel Terapi Musik Klasik Pada Lansia Dengan HipertensiIfah KaharPas encore d'évaluation
- Nur 111 Session 7 Sas 1Document8 pagesNur 111 Session 7 Sas 1Zzimply Tri Sha UmaliPas encore d'évaluation
- Assessing The Cardiovascular and Lymphatic SystemsDocument9 pagesAssessing The Cardiovascular and Lymphatic SystemsYAMINIPRIYANPas encore d'évaluation
- NCP Chest PainDocument2 pagesNCP Chest PainLinsae Troy50% (2)