Vous aimerez peut-être aussi
- Drug Class Ics LabaDocument25 pagesDrug Class Ics LabaStephanie Louisse Gallega HisolePas encore d'évaluation
- Review HDocument62 pagesReview HStephanie Louisse Gallega HisolePas encore d'évaluation
- Efficacy Safety Suitability Cost-EffectivenessDocument30 pagesEfficacy Safety Suitability Cost-EffectivenessStephanie Louisse Gallega HisolePas encore d'évaluation
- MSE FormDocument3 pagesMSE FormStephanie Louisse Gallega HisolePas encore d'évaluation
- Physical Examination Overview: StephylococcusDocument2 pagesPhysical Examination Overview: StephylococcusStephanie Louisse Gallega HisolePas encore d'évaluation
- Date and Time of AssessmentDocument2 pagesDate and Time of AssessmentStephanie Louisse Gallega HisolePas encore d'évaluation
- I. Review of Systems A) General Health SurveyDocument3 pagesI. Review of Systems A) General Health SurveyStephanie Louisse Gallega HisolePas encore d'évaluation
- Chapter 19 Pediatric Diseases and DisordersDocument5 pagesChapter 19 Pediatric Diseases and DisordersStephanie Louisse Gallega HisolePas encore d'évaluation
- Developmental TablesssDocument1 pageDevelopmental TablesssStephanie Louisse Gallega HisolePas encore d'évaluation
- Ineffective Tissue PerfusionDocument3 pagesIneffective Tissue PerfusionStephanie Louisse Gallega Hisole100% (2)
- B. Lateral Rectus Muscle of The EyeDocument1 pageB. Lateral Rectus Muscle of The EyeStephanie Louisse Gallega HisolePas encore d'évaluation
- Bed Making - ScriptDocument6 pagesBed Making - ScriptStephanie Louisse Gallega Hisole100% (2)
- LaboratoryDocument1 pageLaboratoryStephanie Louisse Gallega HisolePas encore d'évaluation
- Caring For The Pregnant Woman With NeurofibromatosisDocument1 pageCaring For The Pregnant Woman With NeurofibromatosisStephanie Louisse Gallega HisolePas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- PMLS Lesson 5Document7 pagesPMLS Lesson 5Althea EspirituPas encore d'évaluation
- Laparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Document4 pagesLaparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Anuj MisraPas encore d'évaluation
- English Informative EssayDocument1 pageEnglish Informative EssayPaul Christian G. SegumpanPas encore d'évaluation
- Nur 601 - Literature Review Manuscript-Icd-10-Sunny Carrington-HahnDocument22 pagesNur 601 - Literature Review Manuscript-Icd-10-Sunny Carrington-Hahnapi-357138638Pas encore d'évaluation
- ApendikDocument4 pagesApendikSepti AyaPas encore d'évaluation
- Unstable Angina - Cardiovascular Disorders - MSD Manual Professional EditionDocument1 pageUnstable Angina - Cardiovascular Disorders - MSD Manual Professional EditionboynextdoorpkyPas encore d'évaluation
- Infusion PumpDocument14 pagesInfusion PumpSREEDEVI T SURESHPas encore d'évaluation
- Medical Biotechnology Multiple Choice Question (GuruKpo)Document13 pagesMedical Biotechnology Multiple Choice Question (GuruKpo)GuruKPO91% (11)
- Using Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSDocument2 pagesUsing Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSSevina Eka ChannelPas encore d'évaluation
- Parameters of The Model: Name Live Alpha Beta DescriptionDocument5 pagesParameters of The Model: Name Live Alpha Beta DescriptionAngga Prawira KautsarPas encore d'évaluation
- The Role of Radiotherapy in Cancer TreatmentDocument9 pagesThe Role of Radiotherapy in Cancer TreatmentarakbaePas encore d'évaluation
- Unit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheDocument5 pagesUnit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheioakasPas encore d'évaluation
- 2020 Anaphylaxis JACI 2020Document42 pages2020 Anaphylaxis JACI 2020Peter Albeiro Falla CortesPas encore d'évaluation
- Tercera SemanaDocument9 pagesTercera SemanaJesús Torres MayaPas encore d'évaluation
- Manual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFDocument229 pagesManual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFsesjrsPas encore d'évaluation
- Emergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefDocument60 pagesEmergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefHossam atefPas encore d'évaluation
- Mandibulasr Truma ManagementDocument18 pagesMandibulasr Truma Managementjoal510Pas encore d'évaluation
- Case StudyDocument3 pagesCase StudyLouel VicitacionPas encore d'évaluation
- Kleptomania Term PaperDocument6 pagesKleptomania Term Paperbctfnerif100% (1)
- Complications of Insulin TherapyDocument16 pagesComplications of Insulin TherapyIngrid NicolasPas encore d'évaluation
- SeizureDocument10 pagesSeizureRomeo ReyesPas encore d'évaluation
- Parasitology: - IntroductionDocument62 pagesParasitology: - IntroductionHana AliPas encore d'évaluation
- Diabetic Nephropathy BaruDocument24 pagesDiabetic Nephropathy BaruRobiyanti Nur Chalifah HattaPas encore d'évaluation
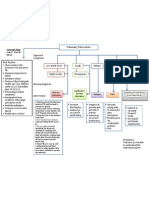
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- +++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchDocument5 pages+++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchEnes ÇakmakPas encore d'évaluation
- HEDING (M-LE-27) : Crane's SummitDocument1 pageHEDING (M-LE-27) : Crane's SummitSilvaPas encore d'évaluation
- All About Rabies Health ScienceDocument28 pagesAll About Rabies Health SciencetototoPas encore d'évaluation
- Daftar Jurnal Kedokteran Internasional GratisDocument3 pagesDaftar Jurnal Kedokteran Internasional GratisdoktermutiaPas encore d'évaluation
- Sports DrinksDocument2 pagesSports DrinksMustofaPas encore d'évaluation
- Anatomy and Physiology - Dengue FeverDocument3 pagesAnatomy and Physiology - Dengue Feverhael yam62% (13)