Vous aimerez peut-être aussi
- P.21 Release DocumentsDocument61 pagesP.21 Release DocumentsOutsourcingCouncilPas encore d'évaluation
- Budget Revision Form GuideDocument5 pagesBudget Revision Form GuideKierstine Joy YamatPas encore d'évaluation
- Vendor Request Form (SA, EA, MENA)Document4 pagesVendor Request Form (SA, EA, MENA)tayarbulatPas encore d'évaluation
- AUTHORIZATION, AGREEMENT AND CERTIFICATION OF TRAININGDocument14 pagesAUTHORIZATION, AGREEMENT AND CERTIFICATION OF TRAININGnevdullPas encore d'évaluation
- Canadian Tax Form GST506 E Cover Sheet: InstructionsDocument4 pagesCanadian Tax Form GST506 E Cover Sheet: InstructionsAkash MelethilPas encore d'évaluation
- Request Fees Guide - Add, Edit, Delete Fee RequestsDocument8 pagesRequest Fees Guide - Add, Edit, Delete Fee RequestsBiju C MenonPas encore d'évaluation
- Salary Survey Questionnaire - Group 7Document6 pagesSalary Survey Questionnaire - Group 7Rashi ChoudharyPas encore d'évaluation
- Opportunity Revenue Reporting Probability Progression: Fields For PTS FormDocument4 pagesOpportunity Revenue Reporting Probability Progression: Fields For PTS FormFayaz SyedPas encore d'évaluation
- Ssa 820Document8 pagesSsa 820biokk81Pas encore d'évaluation
- Employment Pass / S Pass Appeal FormDocument6 pagesEmployment Pass / S Pass Appeal FormHso Hwa KyaingPas encore d'évaluation
- Entrepass Application Form (Form 8) : Work Pass DivisionDocument11 pagesEntrepass Application Form (Form 8) : Work Pass DivisionBanyar AungPas encore d'évaluation
- Work Pass Appeal FormDocument7 pagesWork Pass Appeal FormjoegrantosPas encore d'évaluation
- Adjusted Employer's Annual Federal Tax Return For Agricultural Employees or Claim For RefundDocument4 pagesAdjusted Employer's Annual Federal Tax Return For Agricultural Employees or Claim For RefundFrancis Wolfgang UrbanPas encore d'évaluation
- Student FundraisingDocument5 pagesStudent Fundraisingapi-261450647Pas encore d'évaluation
- Form 2: Instructions For Filling of Eform - 2 (Return of Allotment)Document4 pagesForm 2: Instructions For Filling of Eform - 2 (Return of Allotment)Om PrakashPas encore d'évaluation
- Six New Features in Oracle I-ExpenseDocument7 pagesSix New Features in Oracle I-ExpenseSanjay PriyadarshiPas encore d'évaluation
- On Payroll ProcessingDocument32 pagesOn Payroll Processingಹರೀಶ ಆತ್ರೇಯPas encore d'évaluation
- FPF060 Member'sContributionRemittance V01Document3 pagesFPF060 Member'sContributionRemittance V01christine_balanagPas encore d'évaluation
- Pag IbigDocument3 pagesPag IbigSharon Rillo Ofalda100% (1)
- Work For ClassDocument1 pageWork For Classapi-324581059Pas encore d'évaluation
- fss8 PDFDocument4 pagesfss8 PDFalgareh 95Pas encore d'évaluation
- Comp SurveyDocument9 pagesComp SurveyHOSAM HUSSEINPas encore d'évaluation
- HRMS Questionnaire - Important Before Your SetupDocument24 pagesHRMS Questionnaire - Important Before Your SetupMohammed IlyasPas encore d'évaluation
- Ref Deposit RefundDocument11 pagesRef Deposit RefundTeja BabuPas encore d'évaluation
- ESS Claims FeatureDocument45 pagesESS Claims Featureninaddespo99100% (1)
- Shift Differential Request FormDocument3 pagesShift Differential Request FormManish MehraPas encore d'évaluation
- New Vendor Info FormDocument11 pagesNew Vendor Info FormRoseNPrincePas encore d'évaluation
- HR Requirement Gathering RUDocument3 pagesHR Requirement Gathering RURAM SPas encore d'évaluation
- ACE Startups Grant Interest FormDocument4 pagesACE Startups Grant Interest FormGirish KumarPas encore d'évaluation
- SAMPLE BUSINESS PLAN TITLEDocument10 pagesSAMPLE BUSINESS PLAN TITLENanette Amparo100% (1)
- Journal Voucher TestDocument2 pagesJournal Voucher TestDian Pratiwi APas encore d'évaluation
- HRMS Questionnaire GuideDocument16 pagesHRMS Questionnaire Guidearif61400% (1)
- PRINT in BLACK INK. Ovals Must Be Filled in Completely.Document2 pagesPRINT in BLACK INK. Ovals Must Be Filled in Completely.mik2bgPas encore d'évaluation
- IRS Form SS-8 Worker Status DeterminationDocument5 pagesIRS Form SS-8 Worker Status DeterminationClaudia N Anthony McCoppinPas encore d'évaluation
- Payroll Management System PDFDocument6 pagesPayroll Management System PDFsonysamsung100% (1)
- Income TaxCalculator SRS Ver3.0Document8 pagesIncome TaxCalculator SRS Ver3.0rahul_xxxruPas encore d'évaluation
- Cash Flow Statement TemplateDocument8 pagesCash Flow Statement TemplateFam Sin YunPas encore d'évaluation
- ADP Payroll Detail Manual v4 PDFDocument21 pagesADP Payroll Detail Manual v4 PDFchakripsPas encore d'évaluation
- Oracle HRMS Payroll SetupDocument36 pagesOracle HRMS Payroll SetupPrasenjit Gupta100% (1)
- What Is Cart: "Cart" Stands For Credit Appraisal and Rating ToolDocument37 pagesWhat Is Cart: "Cart" Stands For Credit Appraisal and Rating ToolParvez HussainPas encore d'évaluation
- Tms User Guide Applicant ResponseDocument6 pagesTms User Guide Applicant Responseelangovan7232vijayPas encore d'évaluation
- Separation From Employment Withdrawal RequestDocument28 pagesSeparation From Employment Withdrawal Request20210021661Pas encore d'évaluation
- Accounts Receivables User GuideDocument44 pagesAccounts Receivables User GuidemohdbilalmaqsoodPas encore d'évaluation
- GM-RFX RFQ Response Form TemplateDocument12 pagesGM-RFX RFQ Response Form TemplateRaniMannavaPas encore d'évaluation
- Copc Application For CertificationDocument35 pagesCopc Application For CertificationnieotyagiPas encore d'évaluation
- Civil Application For ExaminationDocument6 pagesCivil Application For ExaminationAnonymous EMAJZz90Pas encore d'évaluation
- InstructionalManualEnglish PDFDocument17 pagesInstructionalManualEnglish PDFMuhammad SalmanPas encore d'évaluation
- Park Vendor Credit Memo T.Code FV65Document2 pagesPark Vendor Credit Memo T.Code FV65Mohamad JumaiziePas encore d'évaluation
- Oklahoma Heart Hospital Guide to Earnings Code MaintenanceDocument27 pagesOklahoma Heart Hospital Guide to Earnings Code MaintenanceNate ScarrittPas encore d'évaluation
- Johnson Form 460 12-31-2011Document115 pagesJohnson Form 460 12-31-2011Isaac GonzalezPas encore d'évaluation
- Affidavit of Employment Form: (To Be Completed by Supervisor)Document3 pagesAffidavit of Employment Form: (To Be Completed by Supervisor)Jozef VeraiPas encore d'évaluation
- Intermediate Accounting 1: a QuickStudy Digital Reference GuideD'EverandIntermediate Accounting 1: a QuickStudy Digital Reference GuidePas encore d'évaluation
- Statement of Cash Flows: Preparation, Presentation, and UseD'EverandStatement of Cash Flows: Preparation, Presentation, and UsePas encore d'évaluation
- In Small Independent Businesses: Women Are Like Cats—Men Are Like DogsD'EverandIn Small Independent Businesses: Women Are Like Cats—Men Are Like DogsPas encore d'évaluation
- SAP Time Integration-CATSDocument84 pagesSAP Time Integration-CATSSingh 10100% (3)
- FK06 MarkvendorfordeletionDocument2 pagesFK06 MarkvendorfordeletionSingh 10Pas encore d'évaluation
- Consultant Handbook For New GLDocument53 pagesConsultant Handbook For New GLPrashant SinghPas encore d'évaluation
- Chap 25 PY PayrollDocument98 pagesChap 25 PY Payrollokail72Pas encore d'évaluation
- FK05 Block UnblockVendorDocument2 pagesFK05 Block UnblockVendorSingh 10Pas encore d'évaluation
- Catc ReportDocument5 pagesCatc ReportSingh 10Pas encore d'évaluation
- Mastering The Six SAP Payroll Building BlocksDocument73 pagesMastering The Six SAP Payroll Building BlocksPikiniso100% (1)
- HR and Finance ConfiDocument87 pagesHR and Finance ConfiSingh 10Pas encore d'évaluation
- Payroll & Time Test Tool (PTTT)Document1 pagePayroll & Time Test Tool (PTTT)Singh 10Pas encore d'évaluation
- FS10N-DisplayG LAccountBalanceDocument2 pagesFS10N-DisplayG LAccountBalanceSingh 10Pas encore d'évaluation
- TCodes Abap PDFDocument0 pageTCodes Abap PDFSingh 10Pas encore d'évaluation
- FK04 DisplayVendorAccountChangesDocument2 pagesFK04 DisplayVendorAccountChangesSingh 10Pas encore d'évaluation
- SAP HR Config AllDocument486 pagesSAP HR Config AllSatyendra Gupta100% (1)
- SAP HR InfotypesDocument7 pagesSAP HR InfotypesRamPas encore d'évaluation
- FS10N-DisplayG LAccountBalanceDocument2 pagesFS10N-DisplayG LAccountBalanceSingh 10Pas encore d'évaluation
- FB03 Display GL/AP Documents: PurposeDocument2 pagesFB03 Display GL/AP Documents: PurposeSingh 10Pas encore d'évaluation
- FI03 Display Bank Master Data: PurposeDocument2 pagesFI03 Display Bank Master Data: PurposeSingh 10Pas encore d'évaluation
- View Vendor BalancesDocument2 pagesView Vendor BalancesSingh 10Pas encore d'évaluation
- Create Bank DataDocument2 pagesCreate Bank DataSingh 10Pas encore d'évaluation
- Change Bank Master Data DetailsDocument2 pagesChange Bank Master Data DetailsSingh 10Pas encore d'évaluation
- FK02 ChangeaVendorMasterRecordDocument7 pagesFK02 ChangeaVendorMasterRecordSingh 10Pas encore d'évaluation
- FK03 DisplayavendormasterrecordDocument6 pagesFK03 DisplayavendormasterrecordSingh 10Pas encore d'évaluation
- FK01 CreateaVendorMasterRecordDocument7 pagesFK01 CreateaVendorMasterRecordSingh 10Pas encore d'évaluation
- FCHN DisplayCheckRegisterDocument3 pagesFCHN DisplayCheckRegisterSingh 10Pas encore d'évaluation
- FCH8 CancelCheckPaymentDocument2 pagesFCH8 CancelCheckPaymentSingh 10Pas encore d'évaluation
- FCHN AbandonedcheckprocessDocument11 pagesFCHN AbandonedcheckprocessSingh 10Pas encore d'évaluation
- FCH7 ReprintCheckDocument2 pagesFCH7 ReprintCheckSingh 10Pas encore d'évaluation
- Fch1 Display Check Information: PurposeDocument2 pagesFch1 Display Check Information: PurposeSingh 10Pas encore d'évaluation
- FCH2 DisplayPaymentDocumentChecksDocument2 pagesFCH2 DisplayPaymentDocumentChecksSingh 10Pas encore d'évaluation
- FBL3n-Display ChangeG LAccountLineItemsDocument2 pagesFBL3n-Display ChangeG LAccountLineItemsSingh 10Pas encore d'évaluation
- Donors Tax FAQs: Exemptions and ValuationDocument4 pagesDonors Tax FAQs: Exemptions and ValuationBlesilda OracoyPas encore d'évaluation
- G. L. Bajaj Institute of Technology & Management: Fee ReceiptDocument1 pageG. L. Bajaj Institute of Technology & Management: Fee ReceiptmaniastuntPas encore d'évaluation
- MyVanilla Visa CFPB Long Form PDFDocument1 pageMyVanilla Visa CFPB Long Form PDFOzell Stanley0% (1)
- MINHAJ University Fee Challan for MSC-MTH StudentDocument2 pagesMINHAJ University Fee Challan for MSC-MTH StudentSo NiaPas encore d'évaluation
- Mireillenkuansambumiss DiavuaDocument3 pagesMireillenkuansambumiss DiavuaMayamona Nkuansambu LikePas encore d'évaluation
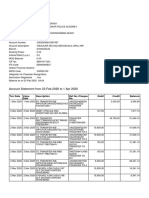
- Mr. Shyam Singh's bank account statement and detailsDocument3 pagesMr. Shyam Singh's bank account statement and detailsShyamPas encore d'évaluation
- Filled Pension Claim Format PDFDocument4 pagesFilled Pension Claim Format PDFAjay BPas encore d'évaluation
- 1-12 Inv-Gb-123115881-2023-14512 33.64Document1 page1-12 Inv-Gb-123115881-2023-14512 33.64pravasunfilteredPas encore d'évaluation
- Fredrickson v. Starbucks CorporationDocument51 pagesFredrickson v. Starbucks Corporationmary engPas encore d'évaluation
- Cashless Economy Period in IndiaDocument11 pagesCashless Economy Period in IndiaVANSH GOYALPas encore d'évaluation
- Haryana CST Return Format Form - 1Document2 pagesHaryana CST Return Format Form - 1Virender SainiPas encore d'évaluation
- BIR HistoryDocument6 pagesBIR HistoryJayphi Taganas BaddungonPas encore d'évaluation
- 3 Month Deferment Tax Instalment CP204Document1 page3 Month Deferment Tax Instalment CP204Alaya VirjaPas encore d'évaluation
- Tax RemediesDocument22 pagesTax RemediesJezreel CastañagaPas encore d'évaluation
- Inv - 2469306Document2 pagesInv - 2469306rajeshPas encore d'évaluation
- 58568990Document2 pages58568990Tomami YukotaPas encore d'évaluation
- MR Sharanabasappa Hosamani 01386452: Sap Labs India Pvt. LTDDocument1 pageMR Sharanabasappa Hosamani 01386452: Sap Labs India Pvt. LTDSharanu HosamaniPas encore d'évaluation
- A Project of KIPS Preparations (PVT) LTD A Project of KIPS Preparations (PVT) LTD A Project of KIPS Preparations (PVT) LTDDocument1 pageA Project of KIPS Preparations (PVT) LTD A Project of KIPS Preparations (PVT) LTD A Project of KIPS Preparations (PVT) LTDTalha AwanPas encore d'évaluation
- Ola ReceiptDocument3 pagesOla Receiptjyotsna jhaPas encore d'évaluation
- Scripts StatusDocument6 pagesScripts StatusGanesh ChimmaniPas encore d'évaluation
- Invoice: Hollyhill Industrial Estate Hollyhill, Cork Ireland VAT No: GB 117223643Document1 pageInvoice: Hollyhill Industrial Estate Hollyhill, Cork Ireland VAT No: GB 117223643Marian BlnPas encore d'évaluation
- Best Price On Swiss Bell HotelDocument4 pagesBest Price On Swiss Bell HotelFahrudin AlkhemiPas encore d'évaluation
- Demand SurveyDocument4 pagesDemand SurveySunilkumar CePas encore d'évaluation
- N3552005822 SKU71 - 2 - 3552005822: Service Number IvrsDocument1 pageN3552005822 SKU71 - 2 - 3552005822: Service Number IvrsShubham NamdevPas encore d'évaluation
- Hire Purchase SystemDocument5 pagesHire Purchase SystemMasoom Farishtah0% (1)
- Introduction to Plastic MoneyDocument70 pagesIntroduction to Plastic MoneyParm Sidhu100% (12)
- Act Madhu BillDocument2 pagesAct Madhu BillMadhuPas encore d'évaluation
- SharonDocument6 pagesSharonLucky LuckyPas encore d'évaluation
- DAMAC MAISON PRIVE 1BR 886SF CondoDocument4 pagesDAMAC MAISON PRIVE 1BR 886SF CondoAnonymous 2rYmgRPas encore d'évaluation
- Transactions: Page 1 of 3Document3 pagesTransactions: Page 1 of 3novelPas encore d'évaluation