Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Testsv - Final 26971 32528Document63 pagesTestsv - Final 26971 32528Iris BakerPas encore d'évaluation
- Perioperative Nursing Care and ConsiderationsDocument45 pagesPerioperative Nursing Care and ConsiderationsGaoudam NatarajanPas encore d'évaluation
- Dysrhythmia Interpretation Modules 1-6 June 2012Document126 pagesDysrhythmia Interpretation Modules 1-6 June 2012Jess Varose100% (3)
- A Conceptual Guide To MRCP (Uk) Paces Exam.: Station 2, 4 and 5. SampleDocument29 pagesA Conceptual Guide To MRCP (Uk) Paces Exam.: Station 2, 4 and 5. Samplesoe100% (1)
- Layout Plan of School of NursingDocument3 pagesLayout Plan of School of NursingGaoudam Natarajan100% (6)
- Layout Plan of School of NursingDocument3 pagesLayout Plan of School of NursingGaoudam Natarajan100% (6)
- Bronchial Asthma 78753665 by AnilKumarGowdaDocument53 pagesBronchial Asthma 78753665 by AnilKumarGowdaGaoudam NatarajanPas encore d'évaluation
- Prevention and Control of Communicable DiseasesDocument247 pagesPrevention and Control of Communicable DiseasesGaoudam NatarajanPas encore d'évaluation
- FertiQoL ScoringDocument2 pagesFertiQoL ScoringGaoudam Natarajan100% (1)
- Guidelines For GNM PDFDocument133 pagesGuidelines For GNM PDFJeeshanKhanPas encore d'évaluation
- Curriculum Vitae Contact Information: Staff Nurse in Casualty, ICCU, General and Special Wards, Male Medical and SurgicalDocument2 pagesCurriculum Vitae Contact Information: Staff Nurse in Casualty, ICCU, General and Special Wards, Male Medical and SurgicalGaoudam NatarajanPas encore d'évaluation
- 17 2015 Rejected CandidatesDocument1 page17 2015 Rejected CandidatesGaoudam NatarajanPas encore d'évaluation
- Developing Nursing Standards / Protocols For HospitalDocument34 pagesDeveloping Nursing Standards / Protocols For HospitalGaoudam NatarajanPas encore d'évaluation
- Home Science (Eng) Ch-8 PDFDocument14 pagesHome Science (Eng) Ch-8 PDFGaoudam NatarajanPas encore d'évaluation
- Long Work Hours May Raise Risk of Heart DiseaseDocument2 pagesLong Work Hours May Raise Risk of Heart DiseaseGaoudam NatarajanPas encore d'évaluation
- Regular health check-ups keep families healthyDocument2 pagesRegular health check-ups keep families healthyGaoudam NatarajanPas encore d'évaluation
- Long Work Hours May Raise Risk of Heart DiseaseDocument2 pagesLong Work Hours May Raise Risk of Heart DiseaseGaoudam NatarajanPas encore d'évaluation
- Elderly in IndiaDocument63 pagesElderly in IndiaAdesh KumarPas encore d'évaluation
- Acceptanace Letter FormatDocument1 pageAcceptanace Letter FormatGaoudam NatarajanPas encore d'évaluation
- 05 N503 29276Document18 pages05 N503 29276Gaoudam NatarajanPas encore d'évaluation
- Gynecologist Related TestDocument13 pagesGynecologist Related TestGaoudam NatarajanPas encore d'évaluation
- 1.menopausal Problems 99 228Document7 pages1.menopausal Problems 99 228Gaoudam NatarajanPas encore d'évaluation
- Canadian Immigration Assessment Form: 1 - Personal InformationDocument4 pagesCanadian Immigration Assessment Form: 1 - Personal InformationGaoudam NatarajanPas encore d'évaluation
- Top 11 Healthy Snack FoodsDocument1 pageTop 11 Healthy Snack FoodsGaoudam NatarajanPas encore d'évaluation
- Learning TheoriesDocument17 pagesLearning TheoriesGaoudam NatarajanPas encore d'évaluation
- 05 N050 31174Document19 pages05 N050 31174Gaoudam NatarajanPas encore d'évaluation
- Organizingpatientcare 130707231102 Phpapp01Document79 pagesOrganizingpatientcare 130707231102 Phpapp01Gaoudam NatarajanPas encore d'évaluation
- Speciality SeminarDocument1 pageSpeciality SeminarGaoudam NatarajanPas encore d'évaluation
- 05 N028 22376Document17 pages05 N028 22376Gaoudam NatarajanPas encore d'évaluation
- Prevention of BaDocument10 pagesPrevention of BaGaoudam NatarajanPas encore d'évaluation
- 05 N025 5771Document17 pages05 N025 5771Gaoudam NatarajanPas encore d'évaluation
- 05 N502 28881Document24 pages05 N502 28881Gaoudam NatarajanPas encore d'évaluation
- Comparing blood donation knowledge among science and non-science studentsDocument10 pagesComparing blood donation knowledge among science and non-science studentsGaoudam NatarajanPas encore d'évaluation
- AnticoagulantsDocument26 pagesAnticoagulantsimnnayakPas encore d'évaluation
- Adams-Stokes 1º Sintoma Febre ReumáticaDocument5 pagesAdams-Stokes 1º Sintoma Febre Reumáticacarvalho.tr4270Pas encore d'évaluation
- Ebook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFDocument40 pagesEbook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFalexandercampbelldkcnzafgtw100% (10)
- Dexmedetomidine ICU Sedation and UsesDocument2 pagesDexmedetomidine ICU Sedation and UsesWinter HyuckPas encore d'évaluation
- Pic Heart Talk Final Programme (19-10-13)Document4 pagesPic Heart Talk Final Programme (19-10-13)usman9117563Pas encore d'évaluation
- Icu NCP 2Document2 pagesIcu NCP 2James Casauran LandagoraPas encore d'évaluation
- Blood Clots: How Does Blood Clot?Document2 pagesBlood Clots: How Does Blood Clot?Pebrian Diki PrestyaPas encore d'évaluation
- European J of Heart Fail - 2021 - Moura - Integration of Imaging and Circulating Biomarkers in Heart Failure A ConsensusDocument20 pagesEuropean J of Heart Fail - 2021 - Moura - Integration of Imaging and Circulating Biomarkers in Heart Failure A Consensustotya91Pas encore d'évaluation
- 1545Document20 pages1545micjenPas encore d'évaluation
- 12 Lead Ecg or EkgDocument24 pages12 Lead Ecg or EkgSid KhanPas encore d'évaluation
- Palpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Document19 pagesPalpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Navojit ChowdhuryPas encore d'évaluation
- Cardiac Risk Assessemnt FlowchartDocument1 pageCardiac Risk Assessemnt FlowchartjamesomoorePas encore d'évaluation
- Dilated) Adenosine/Dipyridamole (Coronary Arteries Vasodilators) Cause Generalized CoronaryDocument3 pagesDilated) Adenosine/Dipyridamole (Coronary Arteries Vasodilators) Cause Generalized Coronarylang mansiPas encore d'évaluation
- Bowel IschemiaDocument79 pagesBowel IschemiaNovita AnjaniPas encore d'évaluation
- Achd LectureDocument48 pagesAchd LecturedrmdsaeedPas encore d'évaluation
- Brachiocephalic TrunkDocument3 pagesBrachiocephalic TrunkstephPas encore d'évaluation
- Practice ECGStripsDocument300 pagesPractice ECGStripsrobby zayendraPas encore d'évaluation
- CS-EP data collection worksheetDocument2 pagesCS-EP data collection worksheetNnaemeka NwobodoPas encore d'évaluation
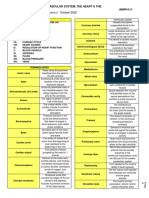
- 1.08 - The Cardiovascular System, The Heart & The Blood VesselsDocument9 pages1.08 - The Cardiovascular System, The Heart & The Blood Vessels13PLAN, SENTH RUEN, APas encore d'évaluation
- Electrocardiography: David M. Mirvis - Ary L. GoldbergerDocument45 pagesElectrocardiography: David M. Mirvis - Ary L. GoldbergerMarius David0% (1)
- Self Measured Blood Pressure 0Document2 pagesSelf Measured Blood Pressure 0Dercio mungoiPas encore d'évaluation
- Inotropes in Term NeonatesDocument6 pagesInotropes in Term Neonateserika lunaPas encore d'évaluation
- Dr. Hande's Cardiology OPD SheetDocument1 pageDr. Hande's Cardiology OPD SheetSunil RahangdalePas encore d'évaluation
- Diagnostic AlgorithmDocument7 pagesDiagnostic AlgorithmindahPas encore d'évaluation
- HDL Cholesterol KitDocument2 pagesHDL Cholesterol KitZumaira AbbasPas encore d'évaluation
- Chapter25Document29 pagesChapter25Evelyn MedinaPas encore d'évaluation
- Drugs Used in CardiologyDocument2 pagesDrugs Used in CardiologymisswongPas encore d'évaluation