Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- SureshBoddu - CF - MeritIncrementLetter - 20200131 - 0053031580415448Document1 pageSureshBoddu - CF - MeritIncrementLetter - 20200131 - 0053031580415448sooriroyPas encore d'évaluation
- Mobile Services: Your Account Summary This Month'S ChargesDocument7 pagesMobile Services: Your Account Summary This Month'S ChargessooriroyPas encore d'évaluation
- Cervical - Trapezitis (Left) : Care - FitDocument2 pagesCervical - Trapezitis (Left) : Care - FitsooriroyPas encore d'évaluation
- Mobile Services: Your Account Summary This Month'S ChargesDocument4 pagesMobile Services: Your Account Summary This Month'S ChargessooriroyPas encore d'évaluation
- Healthface PVT LTD: Salary Slip For June - 2020Document1 pageHealthface PVT LTD: Salary Slip For June - 2020sooriroyPas encore d'évaluation
- Essa AccreditationsDocument13 pagesEssa AccreditationssooriroyPas encore d'évaluation
- Chittoor - Sarpanch List-2013Document19 pagesChittoor - Sarpanch List-2013sooriroyPas encore d'évaluation
- Exercise Physiologist Sample ResumeDocument2 pagesExercise Physiologist Sample ResumesooriroyPas encore d'évaluation
- Sixthsensetechnology 120430234445 Phpapp01Document26 pagesSixthsensetechnology 120430234445 Phpapp01sooriroyPas encore d'évaluation
- Mahanati Savithri - Compressed PDFDocument243 pagesMahanati Savithri - Compressed PDFsooriroy50% (2)
- May JYI 2Document5 pagesMay JYI 2sooriroyPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Muscle MechanicsbDocument15 pagesMuscle MechanicsbTamas KalmarPas encore d'évaluation
- Normal End Feel Abnormal End Feel: ST NDDocument2 pagesNormal End Feel Abnormal End Feel: ST NDsungmin kimPas encore d'évaluation
- Body Beast Build Legs Workout SheetDocument1 pageBody Beast Build Legs Workout SheetDavid JanuszewskiPas encore d'évaluation
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDocument11 pagesMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoPas encore d'évaluation
- Skeletal Muscle StructureDocument38 pagesSkeletal Muscle Structuretoyy100% (1)
- 10 Week Vertical Jump Training Program PDFDocument49 pages10 Week Vertical Jump Training Program PDFMauricio Andres Mongui Molina50% (2)
- 1 2muscular System 1Document23 pages1 2muscular System 1api-343368893Pas encore d'évaluation
- Ant Shoulder DislocationDocument3 pagesAnt Shoulder DislocationÉva KappéterPas encore d'évaluation
- LABORATORY PRACTICE: Range of Motion WorksheetDocument12 pagesLABORATORY PRACTICE: Range of Motion WorksheetMike ConnorsPas encore d'évaluation
- Jonathan Edwards TrainingDocument8 pagesJonathan Edwards TrainingMark100% (1)
- How To Fix Flat Feet (Pes Planus) - Posture Direct PDFDocument77 pagesHow To Fix Flat Feet (Pes Planus) - Posture Direct PDFBosco DominicPas encore d'évaluation
- OMT Range of MotionDocument1 pageOMT Range of MotionMedShare100% (2)
- Bones HWDocument6 pagesBones HWWendi KongPas encore d'évaluation
- Easy PNF DVD BrochureDocument48 pagesEasy PNF DVD BrochurePaolaEspinolaPas encore d'évaluation
- The Bench Press PDFDocument10 pagesThe Bench Press PDFMarco TorrePas encore d'évaluation
- Isometric ExerciseDocument3 pagesIsometric ExerciseSam IsaacPas encore d'évaluation
- 10.1016@j.csm.2009.09.004 2Document26 pages10.1016@j.csm.2009.09.004 29661jackPas encore d'évaluation
- CApsules StretchDocument26 pagesCApsules StretchAnujPas encore d'évaluation
- Management of Sports InjuriesDocument35 pagesManagement of Sports InjuriesabdulazizmochammadPas encore d'évaluation
- Ann Cools 3Document38 pagesAnn Cools 3Walter PelaezPas encore d'évaluation
- Musculoskeletal XXXXXXXXXDocument25 pagesMusculoskeletal XXXXXXXXXIgnatius Erik Dwi WahyudiPas encore d'évaluation
- 5 Biomechanical Model Diagonal-Spiral Stecco PDFDocument10 pages5 Biomechanical Model Diagonal-Spiral Stecco PDFDaniele Mei100% (1)
- Test/Sign Procedure (+) INDDocument8 pagesTest/Sign Procedure (+) INDDesi SmithPas encore d'évaluation
- Examination of Shoulder Joint-1Document3 pagesExamination of Shoulder Joint-1adiPas encore d'évaluation
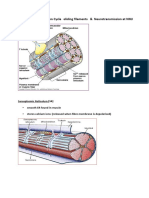
- L3. Muscle Contraction Cycle - Sliding Filaments & Neurotransmission at NMJDocument9 pagesL3. Muscle Contraction Cycle - Sliding Filaments & Neurotransmission at NMJYolande ClothierPas encore d'évaluation
- Task Form (4) AnsweredDocument5 pagesTask Form (4) AnsweredALLAN JAY D. LAPIZPas encore d'évaluation
- Fitt Program Plan SethpruittDocument2 pagesFitt Program Plan Sethpruittapi-267357286Pas encore d'évaluation
- Bosco Arms & ShouldersDocument25 pagesBosco Arms & Shouldersmark.mcguigan992100% (3)
- Penerapan Biomekanika, Respons Dan Adaptasi Otot RangkaDocument36 pagesPenerapan Biomekanika, Respons Dan Adaptasi Otot RangkaMohamad Rendy Firdianto100% (1)
- Ergonomi Di Rumah Sakit PDFDocument50 pagesErgonomi Di Rumah Sakit PDFUus Suparman100% (9)