Vous aimerez peut-être aussi
- Adam Goleman Emotionl Inteligence Non Violent ComunicationDocument655 pagesAdam Goleman Emotionl Inteligence Non Violent Comunicationtomy100% (2)
- Low BackDocument7 pagesLow BackMuhammad FahmyPas encore d'évaluation
- Degenerative Disorders of Lumbar SpineDocument54 pagesDegenerative Disorders of Lumbar Spineapi-19916399Pas encore d'évaluation
- Up To Date in Internal MedicineDocument366 pagesUp To Date in Internal Medicinez13407100% (2)
- Up To Date in Internal MedicineDocument366 pagesUp To Date in Internal Medicinez13407100% (2)
- Knee Exam Guide: Look, Feel, Move, TestsDocument23 pagesKnee Exam Guide: Look, Feel, Move, TestsAaron Nameer Abrar RahmanPas encore d'évaluation
- Dr. Sunil Kumar Sharma Senior Resident, Dept. of Neurology G.M.C., KOTADocument67 pagesDr. Sunil Kumar Sharma Senior Resident, Dept. of Neurology G.M.C., KOTAsuckeydluffyPas encore d'évaluation
- Approach To A Patient With Low Back Ache: DR - Ankur BatraDocument104 pagesApproach To A Patient With Low Back Ache: DR - Ankur BatraAnkur Batra100% (1)
- Clinical Cases NeurologyDocument200 pagesClinical Cases Neurologysimi y100% (1)
- Addressing Selection CriteriaDocument15 pagesAddressing Selection Criterialinh_tran663495% (19)
- ADMEDocument10 pagesADMEdhavalPas encore d'évaluation
- 17 Principles PDFDocument1 page17 Principles PDFKing KarvoPas encore d'évaluation
- Neck and Low Back PainDocument128 pagesNeck and Low Back Painralu_balajPas encore d'évaluation
- LS4 Koica Module 1Document27 pagesLS4 Koica Module 1Kerielle Deane TutongPas encore d'évaluation
- Cns ExaminationDocument17 pagesCns ExaminationJuana Maria Garcia Espinoza100% (1)
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Construction Manpower SafetyDocument48 pagesConstruction Manpower SafetyJohn Dave pogi100% (1)
- Low Back Pain PDFDocument4 pagesLow Back Pain PDFnetifarhatiiPas encore d'évaluation
- Mini-Invasive Surgery of The Hip PDFDocument173 pagesMini-Invasive Surgery of The Hip PDFNoel Alonso Calleros HernandezPas encore d'évaluation
- Dr. Waqas Ayubian Notes For Step 3Document772 pagesDr. Waqas Ayubian Notes For Step 3Muhammad HammadPas encore d'évaluation
- Hemodialysis, Phosphorus and Calcium, Peritoneal DialysisDocument29 pagesHemodialysis, Phosphorus and Calcium, Peritoneal DialysisTrizha MaePas encore d'évaluation
- Nursing Theory of Ramona T. Mercer MaterDocument8 pagesNursing Theory of Ramona T. Mercer MaterMark Norriel Cajandab100% (1)
- PollutionDocument11 pagesPollutionModem BodbenPas encore d'évaluation
- Lumbar Spine: A Guide For Neurologists Surgical Disorders of The Thoracic andDocument8 pagesLumbar Spine: A Guide For Neurologists Surgical Disorders of The Thoracic andchristian_dyrPas encore d'évaluation
- Cardinal Manifestations Back and Neck PainDocument33 pagesCardinal Manifestations Back and Neck PainRoby KieranPas encore d'évaluation
- Spinal cord lesion 2 د.رشاد عبدالغنيDocument58 pagesSpinal cord lesion 2 د.رشاد عبدالغنيMohammad BelbahaithPas encore d'évaluation
- Hip Pain in Young Adults: BackgroundDocument5 pagesHip Pain in Young Adults: BackgroundsamoaPas encore d'évaluation
- Evaluation of The Patient With Hip PainDocument12 pagesEvaluation of The Patient With Hip PainannisaPas encore d'évaluation
- Carpal tunnel syndrome symptoms and causesDocument13 pagesCarpal tunnel syndrome symptoms and causesaditPas encore d'évaluation
- 2017 Spine ExaminationDocument7 pages2017 Spine Examinationradhika thapaPas encore d'évaluation
- Anterior Knee Pain Syndrome ReferatDocument28 pagesAnterior Knee Pain Syndrome ReferatnurulPas encore d'évaluation
- Back Pain Printable VersionDocument43 pagesBack Pain Printable VersionSabin ParajuliPas encore d'évaluation
- Kebelet RatnaDocument8 pagesKebelet RatnaOkyWndPas encore d'évaluation
- Back and Nexk PainDocument7 pagesBack and Nexk PainDenise MathrePas encore d'évaluation
- Articulos Trabajo EcografíaDocument2 pagesArticulos Trabajo EcografíaSim FatPas encore d'évaluation
- Foot Drop: Section Anatomy PrimerDocument2 pagesFoot Drop: Section Anatomy PrimerÐr SalmaPas encore d'évaluation
- Lumbar Disc HerniationDocument7 pagesLumbar Disc HerniationkairalmurielPas encore d'évaluation
- Anks PondDocument32 pagesAnks Pondmiskiah lainunPas encore d'évaluation
- A Case Study of Cauda Equina SyndromeDocument5 pagesA Case Study of Cauda Equina SyndromeProfessor Stephen D. Waner100% (5)
- Cervical Radiculopathy Symptoms, Causes, and TreatmentDocument15 pagesCervical Radiculopathy Symptoms, Causes, and TreatmentRandi SukmanaPas encore d'évaluation
- Herniated Nucleus PulposusDocument5 pagesHerniated Nucleus PulposusNestle FolientePas encore d'évaluation
- Osteoarthritis of The KneeDocument8 pagesOsteoarthritis of The Kneeas3syamut649250% (2)
- Drop Claw FootDocument3 pagesDrop Claw FootfmtaPas encore d'évaluation
- Back Pain: Group 4Document71 pagesBack Pain: Group 4Cesar Guico Jr.Pas encore d'évaluation
- Introduction To Clinical Neurology: Acute Low Back and Neck PainDocument64 pagesIntroduction To Clinical Neurology: Acute Low Back and Neck PainKhan A RehPas encore d'évaluation
- CHAPTER 8 Neck AssestDocument61 pagesCHAPTER 8 Neck AssestLinlin Lindayani KusnandarPas encore d'évaluation
- David Butler Neural Tissue Mobilisation-1Document11 pagesDavid Butler Neural Tissue Mobilisation-1Himani BhondgePas encore d'évaluation
- Cervical Radiculopathy: Nonoperative Management of Neck Pain and Radicular SymptomsDocument8 pagesCervical Radiculopathy: Nonoperative Management of Neck Pain and Radicular SymptomsE=MC2Pas encore d'évaluation
- S Pondy Lols Ys ThesisDocument35 pagesS Pondy Lols Ys ThesisSal LiePas encore d'évaluation
- Elbow InjuriesDocument35 pagesElbow Injurieskarthik venegallaPas encore d'évaluation
- Guide to Lower Back Pain Causes and Treatments (LBPDocument44 pagesGuide to Lower Back Pain Causes and Treatments (LBPMohammed Saad NabhanPas encore d'évaluation
- Spondylolisthesis: The forward slippage of one vertebra on the vertebra belowDocument9 pagesSpondylolisthesis: The forward slippage of one vertebra on the vertebra belowwangPas encore d'évaluation
- Lumbar Spinal Stenosis: Pathophysiology, Clinical Features, and DiagnosisDocument14 pagesLumbar Spinal Stenosis: Pathophysiology, Clinical Features, and DiagnosisAnastasia TjanPas encore d'évaluation
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- Peroneal Mononeuropathy TreatmentDocument13 pagesPeroneal Mononeuropathy TreatmentAnnisa Kinanti AstiPas encore d'évaluation
- Low Back Pain: TriageDocument12 pagesLow Back Pain: TriageabidhashamPas encore d'évaluation
- Cauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipDocument32 pagesCauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipraraPas encore d'évaluation
- Spinal Stenosis and Neurogenic Claudication - StatPearls - NCBI BookshelfDocument8 pagesSpinal Stenosis and Neurogenic Claudication - StatPearls - NCBI BookshelfchhabraanPas encore d'évaluation
- Neck Pain Guide: Causes, Symptoms and TreatmentDocument39 pagesNeck Pain Guide: Causes, Symptoms and Treatmentk.adeputriPas encore d'évaluation
- Retired Marine Officer Suffers From Herniated Lumbar DiscDocument4 pagesRetired Marine Officer Suffers From Herniated Lumbar DiscChester NicolePas encore d'évaluation
- Herniated DiscDocument5 pagesHerniated Disc4gen_7Pas encore d'évaluation
- Shoulder PainDocument6 pagesShoulder Painjrice003Pas encore d'évaluation
- LBP 2Document12 pagesLBP 2Attika DiniPas encore d'évaluation
- Apley Bab 18Document38 pagesApley Bab 18Mohammad SutamiPas encore d'évaluation
- Cauda Equina Syndrome: Signs, Symptoms, and Surgical TimingDocument35 pagesCauda Equina Syndrome: Signs, Symptoms, and Surgical TimingVamsi MohanPas encore d'évaluation
- Week 7 Case Study 7 Chir13009Document7 pagesWeek 7 Case Study 7 Chir13009api-479720222Pas encore d'évaluation
- 2014 Evaluating Anterior Knee PainDocument21 pages2014 Evaluating Anterior Knee PainAni Fran SolarPas encore d'évaluation
- 11 20 1 SMDocument6 pages11 20 1 SMSantoshPas encore d'évaluation
- The Spine and LimbsDocument7 pagesThe Spine and LimbsFrancesca vitalePas encore d'évaluation
- Correct Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsD'EverandCorrect Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsPas encore d'évaluation
- Upper Iin NNDocument8 pagesUpper Iin NNPatricia DianaPas encore d'évaluation
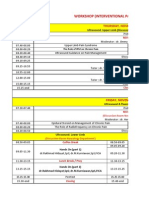
- Workshop (Interventional Pain Management) : Ultrasound: Upper Limb (Discussion Room Neurology Department)Document4 pagesWorkshop (Interventional Pain Management) : Ultrasound: Upper Limb (Discussion Room Neurology Department)Patricia DianaPas encore d'évaluation
- Cme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Document7 pagesCme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Patricia DianaPas encore d'évaluation
- Methylcobalamin for Diabetic NeuropathyDocument49 pagesMethylcobalamin for Diabetic NeuropathyPatricia DianaPas encore d'évaluation
- Biomethylation of Arsenic Is Essentially Detoxicating Event: Teruaki SakuraiDocument0 pageBiomethylation of Arsenic Is Essentially Detoxicating Event: Teruaki SakuraiPatricia DianaPas encore d'évaluation
- Cme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Document7 pagesCme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Patricia DianaPas encore d'évaluation
- Cover JR 2 ZainalDocument1 pageCover JR 2 ZainalPatricia DianaPas encore d'évaluation
- KikkDocument1 pageKikkPatricia DianaPas encore d'évaluation
- Lembar Kemajuan CMDocument6 pagesLembar Kemajuan CMPatricia DianaPas encore d'évaluation
- Anggaran CMEDocument6 pagesAnggaran CMEPatricia DianaPas encore d'évaluation
- Tranexamic Acid for Bleeding StrokesDocument12 pagesTranexamic Acid for Bleeding StrokesPatricia DianaPas encore d'évaluation
- Cme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Document3 pagesCme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Patricia DianaPas encore d'évaluation
- Cme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Document7 pagesCme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Patricia DianaPas encore d'évaluation
- Abstrak IndonesiaDocument1 pageAbstrak IndonesiaPatricia DianaPas encore d'évaluation
- Cme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Document7 pagesCme: Update in Clinical Neurology and Neuroscience: Saturday, November 16Th 2013Patricia DianaPas encore d'évaluation
- Upper Iin NNDocument8 pagesUpper Iin NNPatricia DianaPas encore d'évaluation
- Junedi 5Document5 pagesJunedi 5Patricia DianaPas encore d'évaluation
- Abstrak IndonesiaDocument1 pageAbstrak IndonesiaPatricia DianaPas encore d'évaluation
- Abstrak Indonesia (PatioDocument1 pageAbstrak Indonesia (PatioPatricia DianaPas encore d'évaluation
- HASIL PAP SMEARDocument2 pagesHASIL PAP SMEARPatricia DianaPas encore d'évaluation
- Tranexamic Acid for Bleeding StrokesDocument12 pagesTranexamic Acid for Bleeding StrokesPatricia DianaPas encore d'évaluation
- Junedi 1 OokokDocument16 pagesJunedi 1 OokokPatricia DianaPas encore d'évaluation
- Biomethylation of Arsenic Is Essentially Detoxicating Event: Teruaki SakuraiDocument0 pageBiomethylation of Arsenic Is Essentially Detoxicating Event: Teruaki SakuraiPatricia DianaPas encore d'évaluation
- Junedi 4Document5 pagesJunedi 4Patricia DianaPas encore d'évaluation
- June DikDocument6 pagesJune DikPatricia DianaPas encore d'évaluation
- Upper Iin NNDocument8 pagesUpper Iin NNPatricia DianaPas encore d'évaluation
- Lower Final 11-11Document4 pagesLower Final 11-11Patricia DianaPas encore d'évaluation
- Hematoma Cerebral Intraparenquimatoso e Intraventricular Por Cocaína: Reporte de Un CasoDocument7 pagesHematoma Cerebral Intraparenquimatoso e Intraventricular Por Cocaína: Reporte de Un CasoCarolina GuzmánPas encore d'évaluation
- Shark Fitness Gym 2.0Document1 pageShark Fitness Gym 2.0gourav singhPas encore d'évaluation
- F.I.T.T Principles My Weekly Fitness Work Out Plan: FrequencyDocument6 pagesF.I.T.T Principles My Weekly Fitness Work Out Plan: Frequencyjustine adaoPas encore d'évaluation
- All India VOIPDocument140 pagesAll India VOIPsureesicPas encore d'évaluation
- Online Shopping Stress ReliefDocument2 pagesOnline Shopping Stress ReliefJhyrha Camille FelixPas encore d'évaluation
- Doctoral Dissertation UgentDocument8 pagesDoctoral Dissertation UgentHelpWithFilingDivorcePapersCambridge100% (1)
- ANNEX DQAC Member List 29 OctDocument29 pagesANNEX DQAC Member List 29 OctSpace HR100% (1)
- Theory and Practice of Addiction Counseling 1St Edition Lassiter Test Bank Full Chapter PDFDocument30 pagesTheory and Practice of Addiction Counseling 1St Edition Lassiter Test Bank Full Chapter PDFkatrina.green809100% (11)
- Construct Validity of The Relationship Profile Test Links With Attachment, Identity, Relatedness and Affect. Bornstein 2002Document9 pagesConstruct Validity of The Relationship Profile Test Links With Attachment, Identity, Relatedness and Affect. Bornstein 2002Cualit14Pas encore d'évaluation
- Marbled Pumpkin CheesecakeDocument2 pagesMarbled Pumpkin CheesecakeDewayne AginPas encore d'évaluation
- Lucid Dream QuestionaireDocument14 pagesLucid Dream QuestionairePooja vidhyasagarPas encore d'évaluation
- Brooklyn College Department of Health and Nutrition SciencesDocument13 pagesBrooklyn College Department of Health and Nutrition Sciencesapi-547174770Pas encore d'évaluation
- Journal ReadingDocument53 pagesJournal ReadingRhadezahara PatrisaPas encore d'évaluation
- Swot Analysis of Ggsipu: by Rakhi Dhamija Bba LLB 4th SemesterDocument15 pagesSwot Analysis of Ggsipu: by Rakhi Dhamija Bba LLB 4th SemesterGulka TandonPas encore d'évaluation
- Base Strength 2: My Account (/My-Account/)Document7 pagesBase Strength 2: My Account (/My-Account/)Leonardo ZaraPas encore d'évaluation
- PrognosisDocument10 pagesPrognosisAnida HasnaPas encore d'évaluation
- Guide To Treatment Decision Making For Cleft Type Speech PDFDocument1 pageGuide To Treatment Decision Making For Cleft Type Speech PDFMacarena Paz ÁlvarezPas encore d'évaluation
- University of Glasgow ECG Analysis Program OverviewDocument4 pagesUniversity of Glasgow ECG Analysis Program OverviewMSPas encore d'évaluation
- Future City Outline For StudentsDocument7 pagesFuture City Outline For Studentsapi-237272805Pas encore d'évaluation
- Limus BrochureDocument14 pagesLimus BrochureRick RasenbergPas encore d'évaluation