Vous aimerez peut-être aussi
- Health Science Students Attitude of Using Educational Simulation in SaudiDocument9 pagesHealth Science Students Attitude of Using Educational Simulation in SaudiVictoriano MendezPas encore d'évaluation
- Toc Is 5Document6 pagesToc Is 5Victoriano MendezPas encore d'évaluation
- Comparing effectiveness of high and low fidelity simulation for paramedic studentsDocument11 pagesComparing effectiveness of high and low fidelity simulation for paramedic studentsVictoriano MendezPas encore d'évaluation
- Bienstock Simulation BasedTraining IJOP N1 2023Document17 pagesBienstock Simulation BasedTraining IJOP N1 2023Victoriano MendezPas encore d'évaluation
- Print Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Document1 pagePrint Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Victoriano MendezPas encore d'évaluation
- Equipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededDocument3 pagesEquipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededVictoriano MendezPas encore d'évaluation
- Risk Based PPE Usage - EMS PPE Project PresentationDocument20 pagesRisk Based PPE Usage - EMS PPE Project PresentationVictoriano MendezPas encore d'évaluation
- INACSLSOBPPast Present FutureDocument7 pagesINACSLSOBPPast Present FutureVictoriano MendezPas encore d'évaluation
- Explorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesDocument7 pagesExplorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesVictoriano MendezPas encore d'évaluation
- Sim DictionaryDocument52 pagesSim DictionaryVictoriano MendezPas encore d'évaluation
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Print Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Document1 pagePrint Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Victoriano MendezPas encore d'évaluation
- ACLS Full Lesson Plans PDFDocument60 pagesACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- 1902JEMS Supp5 PDFDocument32 pages1902JEMS Supp5 PDFVictoriano MendezPas encore d'évaluation
- Jems201803 DLDocument68 pagesJems201803 DLVictoriano MendezPas encore d'évaluation
- Stat Reasoning Homework 1 Hw1Document6 pagesStat Reasoning Homework 1 Hw1Victoriano Mendez0% (1)
- Print Story - Understanding The NFPA 1917 Ambulance Standard - EMS1Document2 pagesPrint Story - Understanding The NFPA 1917 Ambulance Standard - EMS1Victoriano MendezPas encore d'évaluation
- Pi Is 1080603214001124Document16 pagesPi Is 1080603214001124Victoriano MendezPas encore d'évaluation
- Vital Signs: Pulse & Heart Rate: Video 1.1: Basic Heart AnatomyDocument10 pagesVital Signs: Pulse & Heart Rate: Video 1.1: Basic Heart AnatomyVictoriano MendezPas encore d'évaluation
- Print Story - 5 Things Great EMS Supervisors Do Differently - EMS1Document2 pagesPrint Story - 5 Things Great EMS Supervisors Do Differently - EMS1Victoriano Mendez100% (1)
- Masking: Janet Holbrook, PHD, MPH Johns Hopkins UniversityDocument11 pagesMasking: Janet Holbrook, PHD, MPH Johns Hopkins UniversityVictoriano MendezPas encore d'évaluation
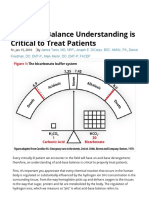
- Acid-Base Balance Understanding Is Critical To Treat Patients - Journal of Emergency Medical ServicesDocument11 pagesAcid-Base Balance Understanding Is Critical To Treat Patients - Journal of Emergency Medical ServicesVictoriano MendezPas encore d'évaluation
- CASE and Experiential LearningDocument11 pagesCASE and Experiential LearningVictoriano MendezPas encore d'évaluation
- 101 Things We Should Teach Every New EMT 1) You..Document6 pages101 Things We Should Teach Every New EMT 1) You..Victoriano MendezPas encore d'évaluation
- Print Story - Faith in EMS - My Karma Ran Over Your Dogma - EMS1Document2 pagesPrint Story - Faith in EMS - My Karma Ran Over Your Dogma - EMS1Victoriano MendezPas encore d'évaluation
- Using Knowledge Checks Throughout TrainingDocument1 pageUsing Knowledge Checks Throughout TrainingVictoriano MendezPas encore d'évaluation
- Multipleintelligences PDFDocument3 pagesMultipleintelligences PDFnitinmisra77Pas encore d'évaluation
- IFRC Yearly Security Report 2008Document16 pagesIFRC Yearly Security Report 2008Victoriano MendezPas encore d'évaluation
- 02prehospitalcervicalspinalimmobilizationaftertrauma Neurosurgery2013 131114031805 Phpapp01Document13 pages02prehospitalcervicalspinalimmobilizationaftertrauma Neurosurgery2013 131114031805 Phpapp01Victoriano MendezPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- AVPU Scale Assesses Consciousness LevelsDocument1 pageAVPU Scale Assesses Consciousness LevelslavnakPas encore d'évaluation
- Pengaruh Elevasi Kepala 30 Terhadap Saturasi Oksigen Dan Kualitas Tidur Pasien Stroke Di Interna 1 Rsud Dr. R. Soedarsono PasuruanDocument13 pagesPengaruh Elevasi Kepala 30 Terhadap Saturasi Oksigen Dan Kualitas Tidur Pasien Stroke Di Interna 1 Rsud Dr. R. Soedarsono PasuruanRudyPas encore d'évaluation
- ASHI PALS Form Field FlyerDocument1 pageASHI PALS Form Field FlyerErwin RomeroPas encore d'évaluation
- ACLS AlgorithmDocument12 pagesACLS AlgorithmwildionPas encore d'évaluation
- KPMG employee health benefits overviewDocument10 pagesKPMG employee health benefits overviewHL LauPas encore d'évaluation
- Abdominal Trauma Signs, Symptoms and Nursing CareDocument24 pagesAbdominal Trauma Signs, Symptoms and Nursing CareSurgeryClassesPas encore d'évaluation
- Gunakan jari telunjuk dan jari tengah untuk membersihkan mulut dari benda asing. Jangan gunakan tangan utuh untuk membersihkan mulutDocument81 pagesGunakan jari telunjuk dan jari tengah untuk membersihkan mulut dari benda asing. Jangan gunakan tangan utuh untuk membersihkan mulutBoby GeaPas encore d'évaluation
- Chapter 1 Powerpoint (Student Copy)Document31 pagesChapter 1 Powerpoint (Student Copy)api-287615830Pas encore d'évaluation
- Crush Syndrome A Case Report and Review of The LiteratureDocument7 pagesCrush Syndrome A Case Report and Review of The LiteratureNur Rahmat WibowoPas encore d'évaluation
- Essential BLS Definitions, Indications and ProtocolsDocument1 pageEssential BLS Definitions, Indications and ProtocolsMoxie MacadoPas encore d'évaluation
- Nursing Leadership Clinical Practicum JournalDocument5 pagesNursing Leadership Clinical Practicum JournalSandra JeffersonPas encore d'évaluation
- POLITRAUMATISMODocument13 pagesPOLITRAUMATISMOJOSEPas encore d'évaluation
- Indian Ambulance SpecificationDocument13 pagesIndian Ambulance Specificationdeepak50% (2)
- Sinhala PPT CPRDocument54 pagesSinhala PPT CPRsl zam zam100% (1)
- Head Trauma Brain InjuryDocument54 pagesHead Trauma Brain Injurymirzabb1Pas encore d'évaluation
- TCCC Quick Reference Guide 2017Document54 pagesTCCC Quick Reference Guide 2017https://www.t-medical.orgPas encore d'évaluation
- START Triage in 30 SecondsDocument10 pagesSTART Triage in 30 SecondsIGDPas encore d'évaluation
- Assesment & Initial Management of Trauma PatientDocument29 pagesAssesment & Initial Management of Trauma PatientSyahnia Wasilatul JannahPas encore d'évaluation
- Pediatric Emergency Assessment Recognition and StabilizationDocument182 pagesPediatric Emergency Assessment Recognition and StabilizationFernando Arancibia100% (2)
- Code Blue in The HospitalDocument26 pagesCode Blue in The HospitalGede Kevin Adhitya SaputraPas encore d'évaluation
- Punjab Emergency Service (Green Book) : ForewordDocument27 pagesPunjab Emergency Service (Green Book) : ForewordManda Khel Apna DesPas encore d'évaluation
- SCAI Shock Classification DeckDocument22 pagesSCAI Shock Classification DeckJimmy JimmyPas encore d'évaluation
- Kohar Hari Santoso, H.R. Eddy Rahardjo, HarjantoDocument8 pagesKohar Hari Santoso, H.R. Eddy Rahardjo, Harjantovela latifahPas encore d'évaluation
- TracheostomyDocument4 pagesTracheostomyJyothiPas encore d'évaluation
- Advance Airway MXDocument17 pagesAdvance Airway MXMardhiyah MusaPas encore d'évaluation
- Initial Evaluation and Management of Penetrating Thoracic Trauma in Adults - UpToDate PDFDocument37 pagesInitial Evaluation and Management of Penetrating Thoracic Trauma in Adults - UpToDate PDFAlberto Mario Zamora RomeroPas encore d'évaluation
- SCI (Spinal Cord Injury)Document51 pagesSCI (Spinal Cord Injury)Awal AlfitriPas encore d'évaluation
- Clinical Fellowships in Medicine and SurgeryDocument26 pagesClinical Fellowships in Medicine and SurgeryKeyser SözePas encore d'évaluation
- 2023 Spring Fling ProgramDocument16 pages2023 Spring Fling ProgramNorth Country EMSPas encore d'évaluation
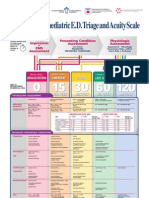
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)